A case of superior mesenteric artery stenting for small intestinal ischaemia caused by superior mesenteric artery invasion of pancreatic cancer
Hiroshi Kuwamura, Yohsuke Suyama, Yasuhiro Enjoji, Takahiro Einama, Yoji Kishi, Hiroshi Shinmoto

TL;DR
A 75-year-old woman with intestinal ischaemia due to pancreatic cancer had a stent placed in her SMA, which improved her condition but later failed due to tumor growth.
Contribution
This case highlights SMA stenting as a potential treatment for malignant tumor-induced intestinal ischaemia.
Findings
SMA stenting improved small intestinal ulcer caused by pancreatic cancer invasion.
Tumor ingrowth led to stent occlusion and re-stenosis, requiring thrombectomy.
Covered stenting is suggested for long-term patency in such cases.
Abstract
Superior mesenteric artery (SMA) invasion by a malignant tumour is a serious condition leading to intestinal ischaemia. Although SMA stenting has been reported to be useful for SMA dissection and stenosis caused by atherosclerotic plaque, SMA stenting for stenosis caused by malignant tumour invasion is rarely reported and uncertain. A 75-year-old woman presented intestinal ulcer and melena caused by SMA invasion of unresectable pancreatic cancer. The bare metal stent was implanted for the vessel stenosis, and a small intestinal ulcer was markedly improved after stenting. However, one and a half months after stenting the stent was occluded and a thrombectomy was performed. After thrombectomy, residual stenosis caused by tumour invasion was observed in the stent. The patient suddenly died 2 days after thrombectomy before additional covered stenting for residual stenosis. Stent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
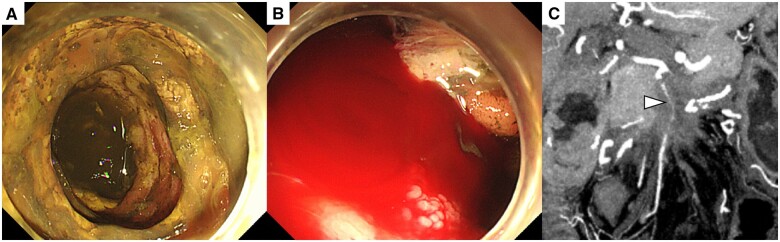 Figure 1
Figure 1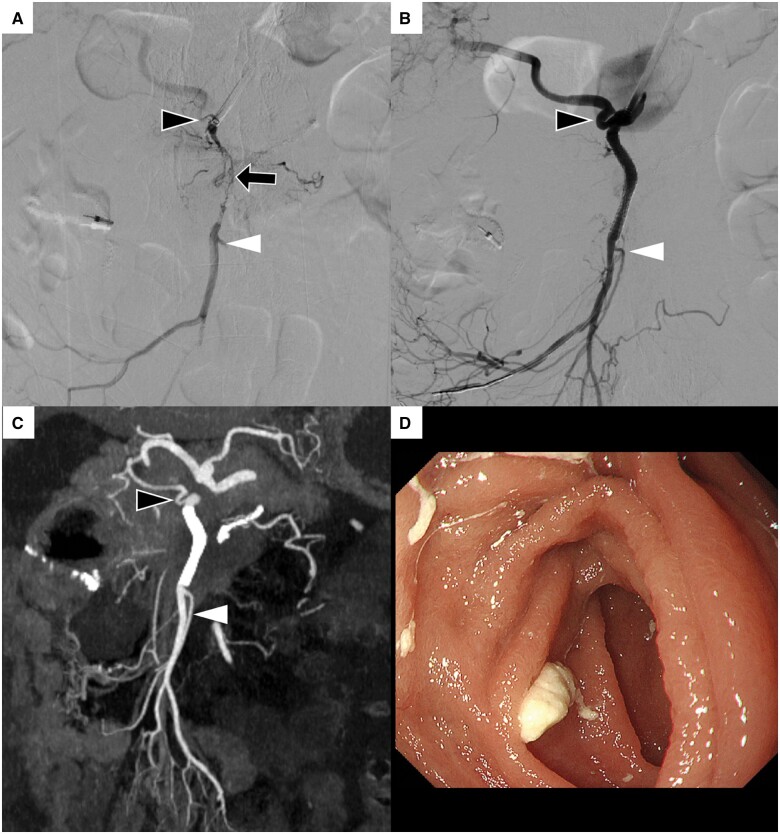 Figure 2
Figure 2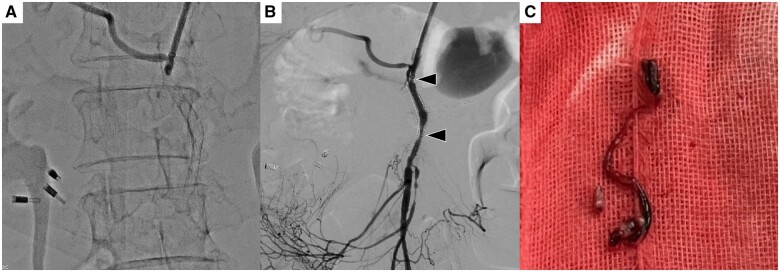 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Renal and Vascular Pathologies · Vascular Anomalies and Treatments
Background
Superior mesenteric artery (SMA) invasion by a malignant tumour is a serious condition leading to intestinal ischaemia. Although SMA stenting has been reported to be useful in SMA dissection and stenosis caused by atherosclerotic plaque,1^,^2 SMA stenting for stenosis caused by malignant tumour invasion is rarely reported and uncertain. This report describes a case in which SMA stenting was performed to treat intestinal ischaemia due to SMA invasion of pancreatic cancer.
Clinical presentation
A 75-year-old woman presented with unresectable pancreatic cancer. The patient underwent partial resection of the small intestine because of necrosis caused by SMA invasion of the tumour. SMA invasion progressed and caused further ischaemia in the remaining small intestine, resulting in a refractory small intestinal ulcer and haemorrhage (Figure 1A and B), and a low haemoglobin level of 4.8 g/dL. Contrast-enhanced computed tomography (CECT) revealed pancreatic cancer surrounding the SMA, which was highly narrowed (Figure 1C). Because further small bowel resection may result in short bowel syndrome, SMA stenting was planned to improve the remaining small bowel ischaemia.
(A, B) Endoscopic images before superior mesenteric artery (SMA) stent placement show multiple ulcers, mucosal erosions and intestinal haemorrhage due to remaining small bowel ischaemia. (C) Coronal contrast-enhanced computed tomography (CECT) image before SMA stenting shows a highly narrowed SMA (arrowhead) due to invasion of pancreatic cancer.
SMA stenting procedure
The left brachial artery was punctured under ultrasound guidance, and a 6 Fr guiding sheath (6 Fr 90 cm Destination, Terumo, Tokyo, Japan) was placed in the abdominal aorta. After placement of the sheath, 2000 units of heparin were injected intravenously. 5 Fr catheter (HHT, Medikit, Tokyo, Japan) and 0.035″ guidewire (radifocus, Terumo, Tokyo, Japan) were used for cannulation of SMA. SMA angiography revealed severe and long stenosis at the area of the tumour invasion, right hepatic artery and ileal artery were branched near the stenosis (Figure 2A). A 0.014″ guidewire (ASAHI CHIKAI V, Asahi Intec, Tokyo, Japan) was used to pass the stenosis and three bare stents (4 mm × 19 mm, 5 mm × 19 mm, and 6 mm × 15 mm Express Vascular SD, Boston Scientific, MN, United States) were implanted, overlapping from distal to proximal of the lesion without covering the origin of important side branches. Angiography of the SMA after stenting showed good patency (Figure 2B).
(A) Superior mesenteric artery (SMA) angiography shows severe and long stenosis (black arrow) at the area of tumour invasion. Right hepatic artery (black arrowhead) and ileal artery (white arrowhead) originate near stenosis. (B, C) SMA angiography and coronal contrast-enhanced computed tomography (CECT) images after stenting show stent patency and improvement of intestinal blood flow. Right hepatic artery (black arrowhead) and ileal artery (white arrowhead) are patent without stent covering. (D) Endoscopic image after SMA stent placement shows the disappearance of multiple ulcers, mucosal erosions and intestinal haemorrhage caused by bowel ischaemia.
Outcome of SMA stenting
The patient underwent double antiplatelet therapy combining aspirin 100 mg/day and clopidogrel 75 mg/day after stenting. Coronal CECT 1 week after stenting confirmed stent patency (Figure 2C). Endoscopy performed 10 days after stenting showed marked improvement of the small intestinal ulcer and mucosal erosions (Figure 2D). Haemoglobin level improved from 4.8 to 9.9 g/dL, and the patient was discharged 13 days after stenting. The stent remained patent, and no symptoms of intestinal ischaemia were observed for more than 1 month after discharge. However, one and a half months after stenting, the patient developed sudden abdominal pain, and CECT showed occlusion of the SMA stent. Therefore, a thrombectomy was performed.
SMA thrombectomy procedure
A 6 Fr guiding sheath (Destination; Terumo, Tokyo, Japan) was inserted into the SMA from the left brachial artery and SMA angiography revealed complete occlusion of the stent (Figure 3A). A 6 Fr large lumen guiding catheter (Cerulean DD6; Medikit, Tokyo, Japan) was used for the thrombectomy. The clot was retrieved and abdominal pain immediately improved. SMA angiography after thrombectomy showed recanalization of the stent and residual stenosis in the middle and proximal portions of the stent (Figure 3B).
(A) Superior mesenteric artery (SMA) angiography shows complete occlusion of the stent. (B) Thrombectomy is performed and SMA angiography shows that the stent is patent; however, there is residual stenosis in the middle and proximal of the stent (black arrowheads). (C) This is a thrombus retrieved by SMA thrombectomy.
Final outcome of this case
Additional covered stent for re-stenosis was planned as a standby procedure because optimal size covered stent was not immediately available in our hospital; however, the patient suddenly went into cardiopulmonary arrest 2 days after thrombectomy and died before additional covered stenting.
Discussion
SMA stenting has been reported to be effective in SMA dissection and atherosclerotic stenosis. Fu et al1 reported that nine patients with symptomatic isolated SMA dissection were treated with bare metal stents, and the false lumen was stable or shrunken in all cases. Girault et al2 placed covered stents in 86 patients with SMA stenosis and reported a high technical success rate of 97% with a primary patency rate of 83% and a secondary patency rate of 99% at 1 year. Covered stenting has also been reported to be useful in the treatment of ruptured SMA pseudoaneurysms, allowing haemostasis while preserving the intestinal blood flow.3 This article reports the case of small bowel ischaemia caused by malignant tumour invasion of the SMA that was treated with SMA stenting; however, similar case reports of SMA stenting for malignant vessel obstruction are rarely reported and the effectiveness is uncertain.
In a multivariate analysis of the risk factors for SMA stent edge stenosis, the diameter ratio of the stent to the vessel and the angle of the distal edge were reported as risk factors for stent edge stenosis, suggesting that the implantation of a stent that is compatible with the vessel diameter is important for long-term stent patency.4^,^5 In our case, stent placement was performed by overlapping the three bare metal stents (4 mm at the distal end of the stenosis, 5 mm in the middle, and 6 mm at the proximal end of the stenosis), which conformed the vessel calibre between distal 4 mm and proximal 6 mm vessel diameter. Although a bare metal stent with a larger diameter may be desirable to prevent early stent occlusion, placement of an over-sized balloon-expandable bare metal stent larger than the distal 4 mm vessel diameter could cause vascular injury. Therefore, a 4 mm balloon-expandable bare metal stent of the same size as the distal vessel diameter was placed. The covered stent was not used for the following reasons: (1) there was a risk of occluding the right hepatic artery and side branches of ileal artery originating near the stenosis which is very important for hepatic and intestinal blood flow, (2) covered stent implantation through severe and long malignant stenosis was expected to be technically difficult because of high-profile delivery shaft compared with the low-profile delivery shaft of the bare metal stent, (3) covered stent optimised for vessel diameter and lesion length was not immediately available in our hospital. Therefore, balloon-expandable bare metal stents were placed, which can easily and accurately adjust the stent position, accommodate a variety of vessel diameters, have a lower risk of branch occlusion, and can easily deliver through severe malignant stenosis.
Neointimal thickening within the stent is a common cause of stent re-stenosis6; however, tumour ingrowth into the stent should also be considered as a cause of stent re-stenosis in the case of vessel obstruction due to malignant tumour.7^,^8 The covered stent is effective for neoplastic vascular occlusion because tumour ingrowth does not occur, whereas there is a risk of occluding important side branches. In our case, acute stent occlusion may have occurred because of thromboembolism triggered by tumour invasion into the stents. Additional covered stents which can prevent tumour invasion should be placed for residual stenosis in the stent after thrombectomy; however, an appropriate covered stent adapted to vessel diameter and lesion length without occluding side branches could not be prepared immediately in our hospital.
We experienced a case of refractory intestinal ischaemia and haemorrhage caused by SMA invasion of malignant tumour treated with SMA bare metal stent implantation, and intestinal ulcers due to intestinal ischaemia improved. On the other hand, re-stenosis and occlusion of the stent due to malignant tumour invasion is a problem, and covered stenting is considered for long-term stent patency.
Learning points
SMA stenting is a treatment option for bowel ischaemia caused by malignant vessel invasion.Covered stent is considered to avoid re-stenosis and occlusion caused by tumour ingrowth.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fu YF , Cao C, Shi YB, Song T. Endovascular bare stenting for isolated superior mesenteric artery dissection. Vasc Endovascular Surg. 2020;54(1):12-16. 10.1177/153857441987493331522622 · doi ↗ · pubmed ↗
- 2Girault A , Pellenc Q, Roussel A, et al Midterm results after covered stenting of the superior mesenteric artery. J Vasc Surg. 2021;74(3):902-909.e 3. 10.1016/j.jvs.2021.02.03833684478 · doi ↗ · pubmed ↗
- 3Kimbara Y , Sato Y, Hasegawa T, et al Covered stent placement for emergency repair of a ruptured superior mesenteric artery pseudoaneurysm in advanced pancreatic head cancer. Radiol Case Rep. 2019;14(1):133-135. 10.1016/j.radcr.2018.10.01230386453 PMC 6206321 · doi ↗ · pubmed ↗
- 4Hang C , Chen W, Su H, Jia Z, Qi C, Gu J. Distal edge stenosis after stent placement for isolated superior mesenteric artery dissection: mechanisms and risk factor analysis. Cardiovasc Intervent Radiol. 2019;42(8):1095-1101. 10.1007/s 00270-019-02244-331093718 · doi ↗ · pubmed ↗
- 5Cho H , Nango M, Sakai Y, et al Neointimal hyperplasia after stent placement across size-discrepant vessels in an animal study. Jpn J Radiol. 2014;32(6):340-346. 10.1007/s 11604-014-0311-324715330 · doi ↗ · pubmed ↗
- 6Clare J , Ganly J, Bursill CA, Sumer H, Kingshott P, de Haan JB. The mechanisms of restenosis and relevance to next generation stent design. Biomolecules. 2022;12(3):430. 10.3390/biom 12030430 PMC 894589735327622 · doi ↗ · pubmed ↗
- 7Takahara Y , Ishige Y, Shionoya I, Fujimoto Y, Oikawa T, Mizuno S. Second SVC stent treatment for tumour ingrowth. Respirol Case Rep. 2020;8(6):e 00619. 10.1002/rcr 2.61932642067 PMC 7330812 · doi ↗ · pubmed ↗
- 8Ju Kim Y , Jin Yoon C, Hwan Lee J, et al Transhepatic stent placement for malignant portal vein obstruction: long term efficacy and factors associated with stent failure. Eur J Radiol. 2022;149:110230. 10.1016/j.ejrad.2022.11023035247667 · doi ↗ · pubmed ↗