Strategic Surgical Intervention in a Rare Presentation of Hip-Spine Syndrome With Lumbosacral Malunion: A Case Report
Miyu Tamaki, Akihiko Hiyama, Daisuke Sakai, Masahiko Watanabe

TL;DR
A 54-year-old man with hip and spine issues was successfully treated with two-stage surgery, showing the importance of considering hip-spine syndrome in similar cases.
Contribution
Demonstrates the efficacy of two-stage corrective surgery with pedicle subtraction osteotomy for hip-spine syndrome.
Findings
The patient's hip synovitis resolved after two-stage corrective surgery.
Symptoms of low back and hip pain improved significantly following the procedure.
Hip-spine syndrome should be considered a potential complication of lumbosacral fusion surgery.
Abstract
The hip and lumbar spine are closely related and can create similar patterns of pain and dysfunction. Furthermore, diagnosing and treating hip and spine conditions can be challenging due to the overlap of symptoms. This report describes the successful treatment of a 54-year-old male with hip-spine syndrome following multiple surgeries for spondylolytic spondylolisthesis. The patient presented with low back pain (LBP) and bilateral hip pain, with radiological findings indicating spinal deformity and hip joint synovitis. Two years after two-stage corrective surgery, including pedicle subtraction osteotomy (PSO), the hip synovitis resolved and the symptoms improved. This case emphasizes the need to consider hip-spine syndrome as a possible complication of lumbosacral spine fusion surgery and demonstrates the efficacy of two-stage corrective surgery with pedicle subtraction osteotomy in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
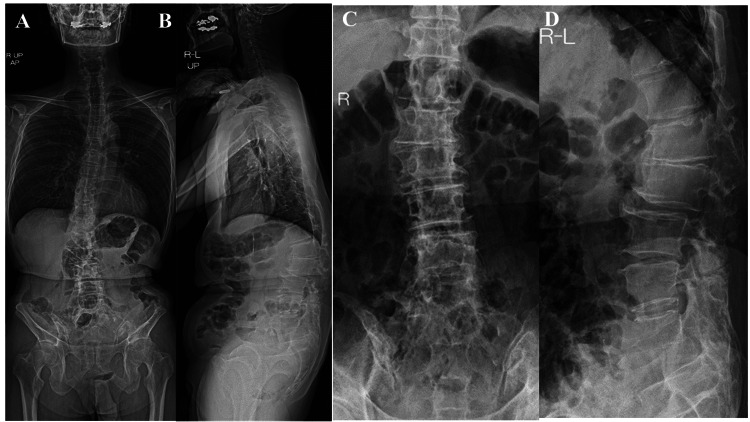 Figure 1
Figure 1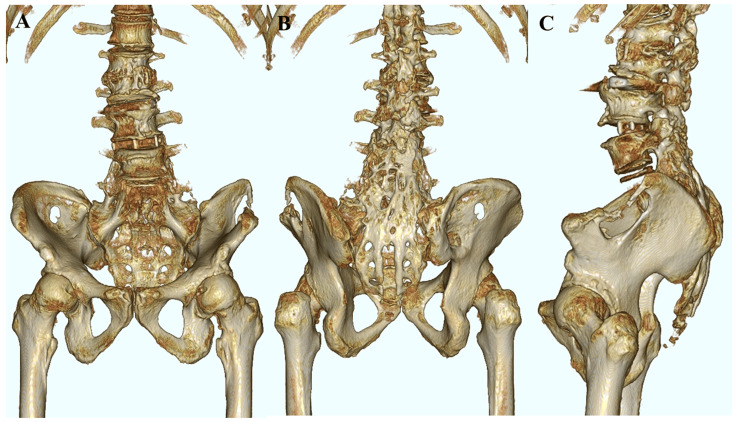 Figure 2
Figure 2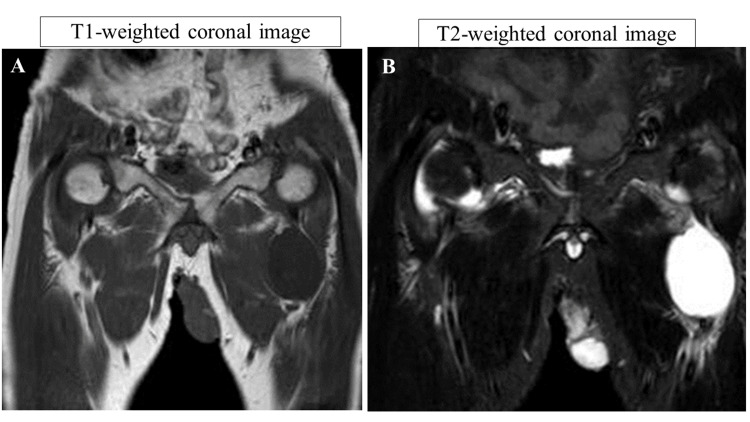 Figure 3
Figure 3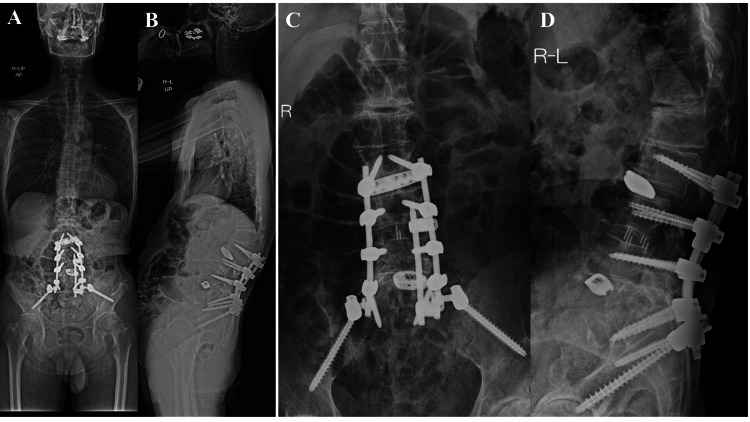 Figure 4
Figure 4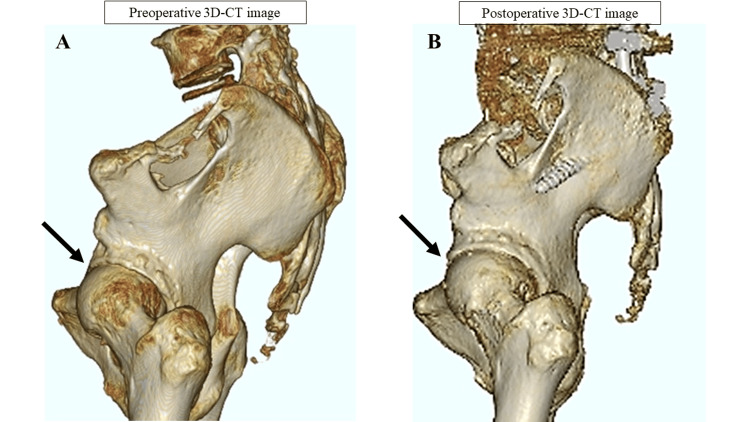 Figure 5
Figure 5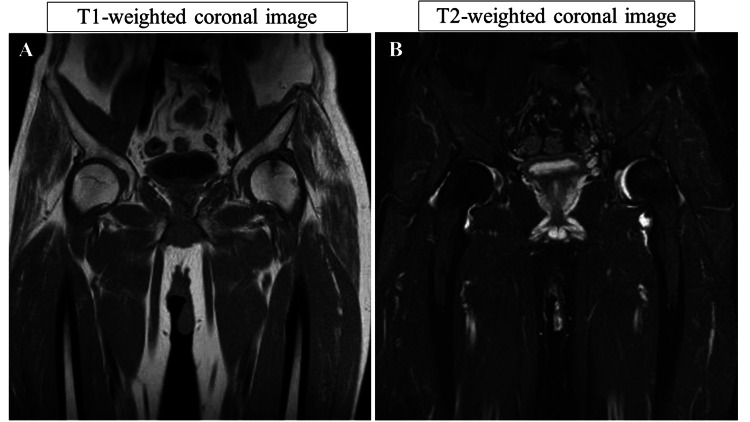 Figure 6
Figure 6| Preoperative | Postoperative 6 months | Postoperative 1 year | Postoperative 2 years | |
| SVA (mm) | 95.5 | 10.9 | 19.7 | 21.5 |
| TPA (°) | 51.6 | 34.7 | 34.4 | 38.5 |
| LL (°) | 3.6 | 17.1 | 29.5 | 20.5 |
| SS (°) | 9.7 | 22.5 | 25.5 | 17.8 |
| PT (°) | 57.7 | 44.8 | 41.8 | 49.5 |
| PI (°) | 67.4 | 67.3 | 67.3 | 67.3 |
| TK (°) | 5.6 | 7.2 | 7.6 | 8.4 |
| PI-LL (°) | 63.8 | 50.2 | 37.8 | 46.8 |
| Preoperative | Postoperative 6 months | Postoperative 1 year | Postoperative 2 years | |
| Low back pain | 0 | 57 | 71 | 71 |
| Lumbar function | 50 | 25 | 42 | 17 |
| Walking ability | 0 | 86 | 64 | 86 |
| Social life function | 24 | 57 | 51 | 57 |
| Mental health | 29 | 54 | 49 | 54 |
| Preoperative | Postoperative 6 months | Postoperative 1 year | Postoperative 2 years | |
| Low back pain (mm) | 30.7 | 20.8 | 9.8 | 3.6 |
| Leg pain (mm) | 92.3 | 14.6 | 5.8 | 5.4 |
| Leg numbness (mm) | 15.3 | 23 | 3.9 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Scoliosis diagnosis and treatment · Hip disorders and treatments
Introduction
Hip-spine syndrome was first reported by Offierski and MacNab in 1983 [1]. The hip and lumbar spine are closely related and can create similar patterns of pain and dysfunction. The hip-spine syndrome poses diagnostic and therapeutic challenges due to overlapping symptoms between hip and spine conditions. This paper describes a rare case of hip-spine syndrome in a patient with lumbosacral dysplasia following malunion after spondylolytic spondylolisthesis surgery at the L5 level.
Case presentation
A 54-year-old male presented with complaints of low back pain (LBP) and pain in both hip joints, with noted swelling in his left hip. His medical history included spondylolisthesis at the L5 level, for which he had undergone posterolateral fusion three times. Physical examination revealed pain upon flexion of both hips. X-ray images of the whole spine demonstrated bilateral degenerative hip arthritis and posterior slippage at L2 (Figure 1). Preoperative spinal parameters were measured using digitized whole-spine standing radiographs. Moreover, three-dimensional computed tomography (3D-CT) revealed lumbosacral malunion at the L5 level (Figure 2). At the same time, magnetic resonance imaging (MRI) of the hips displayed low-intensity signals on T1-weighted images and high-intensity signals on T2-weighted images, indicative of hip synovial bursitis, primarily on the left side (Figure 3).
Preoperative plain X-ray imaging of the spine and hip(A) Standing anterior-posterior view of the whole spine. (B) Standing lateral view of the whole spine. (C) Preoperative plain X-ray anterior-posterior view of the lumbar spine. (D) Preoperative plain X-ray lateral view of the lumbar spine.
Preoperative imaging of the lower thoracic and lumbar spine (3D-CT)(A) Anterior union of the spine in the lumbar and sacral regions. (B) Posterior union of the spine in the lumbar and sacral regions. (C) Lateral union of the spine in the lumbar and sacral regions.3D-CT: three-dimensional computed tomography
Preoperative imaging of the hip (MRI)Hip MRI scan of the hip synovial bursitis, primarily on the left side. (A) Low-intensity signal on the T1-weighted coronal image. (B) High-intensity signal on the T2-weighted coronal image.MRI: magnetic resonance imaging
Consequently, the patient was diagnosed with hip-spine syndrome due to a lumbopelvic alignment disorder resulting from previous surgeries, with the surgical aim being to improve femoral head coverage and correct pelvic retroversion. Considering the surgical invasiveness, corrective surgery was performed in two stages. The first stage involved a lateral lumbar interbody fusion (LLIF) at the L2/L3 and L3/L4 levels using an LLIF cage. One week later, a posterior spinal fusion with pedicle subtraction osteotomy (PSO), extending from L2 to the ilium, was performed [2]. We utilize intraoperative CT navigation for the insertion of implants, including pedicle screws. Intraoperative CT navigation facilitates the placement of bilateral pedicle screws from L2 to the ilium, and a Scoliosis Research Society (SRS)-Schwab Grade 4 osteotomy was performed at L5 [3]. This patient used a banana cage set at a 14-degree angle to achieve significant lordosis at L4/L5.
Table 1 presents the spinal parameters. Table 2 presents the Japanese Orthopedic Association Back Pain Evaluation Questionnaire (JOABPEQ) scores [4]. Table 3 presents Visual Analog Scale (VAS) scores preoperatively, six months postoperatively, one year postoperatively, and two years postoperatively. Two years postoperatively, the spinal parameters showed a notable decrease in the sagittal vertical axis (SVA) from 95.5 mm to 21.5 mm and improved lumbar lordosis (LL) from 3.6° to 20.5°. However, the pelvic incidence (PI)-LL was 46.8°, and PI-LL < 10° was not achieved. JOABPEQ scores indicated significant relief in low back pain from 0 points to 71 points and improved walking ability from 0 points to 86 points, although lumbar function decreased from 50 points to 17 points. VAS scores revealed substantial reductions in low back and leg pain, indicating successful pain management and recovery from surgery.
The X-ray of the left hip joint two years after surgery showed no progression of hip deformity (Figure 4). Additionally, a 3D-CT scan revealed improved coverage of the acetabulum (Figure 5), and postoperative MRI indicated resolution of hip synovial bursitis (Figure 6). Follow-up assessments showed improvements in hip pain and LBP, as noted in the JOABPEQ and VAS scores.
Postoperative plain X-ray imaging of the spine and hip at two years(A) Postoperative plain X-ray of the whole spine (anterior-posterior view). (B) Postoperative plain X-ray of the whole spine (lateral view) shows improved lumbosacral alignment. (C) Postoperative plain X-ray of the lumbar spine (anterior-posterior view). (D) Postoperative plain X-ray of the lumbar spine (lateral view) displays LLIF at the L2/L3 and L3/L4 levels using an LLIF cage, and posterior spinal fusion with PSO.LLIF: lateral lumbar interbody fusion, PSO: pedicle subtraction osteotomy
Postoperative hip imaging (3D-CT)Comparison of pre- and postoperative 3D-CT images of the lumbosacral region: The scans indicate improvements in pelvic retroversion and enhanced femoral head coverage (arrow). (A) Preoperative 3D-CT images of the lumbosacral region. (B) Postoperative 3D-CT images of the lumbosacral region.3D-CT: three-dimensional computed tomography
Postoperative hip imaging (MRI)(A) Postoperative hip MRI (T1-weighted coronal image). (B) Postoperative hip MRI (STIR image). Postoperative hip imaging (MRI) reveals the resolution of synovial bursitis.MRI: magnetic resonance imaging, STIR: short tau inversion recovery
Discussion
Offierski and MacNab originally defined hip-spine syndrome in 1983 and classified it into four distinct types [5]. In this case, we identified lumbosacral malunion as the underlying cause of hip pain and synovitis, categorizing this case as secondary hip-spine syndrome. Multiple lumbar-sacral fusion surgeries performed for spondylolisthesis at the L5 spine fused the lumbosacral vertebrae, affecting the alignment of the spine and pelvis over time. This led to lumbar lordosis and posterior pelvic tilt (PT) changes [6]. Previous reports have indicated that an increase in PT can reduce the anterior coverage of the femoral head within the acetabulum, potentially contributing to the development or exacerbation of hip disorders [7,8]. In our case, we also observed an increased preoperative PT. As a result, there was a decrease in the anterior coverage of the femoral head, indicating an impact on the hip joint due to stress. Therefore, the surgical goal was not to correct the PILL but to address and correct the posterior PT to improve the coverage of the femoral head. Postoperatively, improvements in posterior PT were observed, enhancing the anterior coverage of the femoral head and suggesting a reduction in stress on the femoral head. This was accompanied by improvements in low back pain and leg pain.
Conclusions
Accurate diagnosis and appropriate treatment are crucial for managing hip-spine syndrome. The present case represents a rare instance of a hip-spine syndrome caused by deformity union following multiple spinal fusion procedures performed at a young age. Corrective surgeries, including PSO at the lower lumbar spine, appear beneficial in resolving the issues associated with hip-spine syndrome related to the deformed union at the lumbosacral junction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hip-spine syndrome Spine (Phila Pa 1976) Offierski CM Mac Nab I 31632181983662319810.1097/00007632-198304000-00014 · doi ↗ · pubmed ↗
- 2The comprehensive anatomical spinal osteotomy classification Neurosurgery Schwab F Blondel B Chay E 1121207420142435619710.1227/NEU.0000000000000182 o · doi ↗ · pubmed ↗
- 3SRS-Schwab Grade 4 osteotomy for congenital thoracolumbar kyphosis: a minimum of 2 years follow-up study Spine J Shi B Zhao Q Xu L Liu Z Sun X Zhu Z Qiu Y 205920641820182968051010.1016/j.spinee.2018.04.011 · doi ↗ · pubmed ↗
- 4JOA Back Pain Evaluation Questionnaire (JOABPEQ)/JOA Cervical Myelopathy Evaluation Questionnaire (JOACMEQ). The report on the development of revised versions. April 16, 2007. The Subcommittee of the Clinical Outcome Committee of the Japanese Orthopaedic Association on Low Back Pain and Cervical Myelopathy Evaluation J Orthop Sci Fukui M Chiba K Kawakami M 3483651420091949930510.1007/s 00776-009-1337-8 · doi ↗ · pubmed ↗
- 5Correlation between postoperative imaging parameters and clinical outcomes of percutaneous endoscopic transforaminal decompression for lumbar spinal foraminal and lateral recess stenosis J Pain Res Wu Q Yuan S Zang L 114911571620233702595210.2147/JPR.S 397562 PMC 10072271 · doi ↗ · pubmed ↗
- 6The hip-spine challenge J Bone Joint Surg Am Chavarria JC Douleh DG York PJ 1852186010320213461285010.2106/JBJS.20.01728 · doi ↗ · pubmed ↗
- 7Spinopelvic alignment in patients with osteoarthrosis of the hip: a radiographic comparison to patients with low back pain Spine (Phila Pa 1976) Yoshimoto H Sato S Masuda T Kanno T Shundo M Hyakumachi T Yanagibashi Y 165016573020051602503610.1097/01.brs.0000169446.69758.fa · doi ↗ · pubmed ↗
- 8Sagittal spino-pelvic alignment in rapidly destructive coxarthrosis Eur Spine J Morimoto T Kitajima M Tsukamoto M Yoshihara T Sonohata M Mawatari M 4754812720182884034910.1007/s 00586-017-5282-5 · doi ↗ · pubmed ↗