ECG-gated CT improves diagnosis in prosthetic valve degeneration
Jonathan X Fang, Tiberio M Frisoli, Gennaro Giustino, Pedro A Villablanca, Pedro Engel Gonzalez, Brian P O’Neill, Dee Dee Wang, William W O’Neill, James C Lee

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
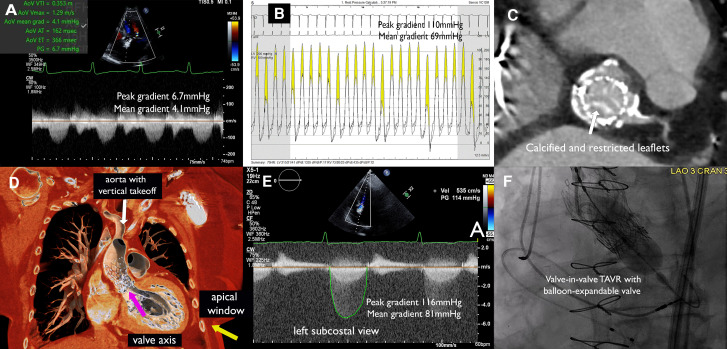 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac pacing and defibrillation studies · Cardiac Structural Anomalies and Repair
An 81-year-old woman with a prior valve-in-valve transcatheter implantation (TAVI) of a 23 mm CoreValve (Medtronic, USA) inside a 21 mm Carpentier (Edwards Lifesciences, USA) bioprosthesis 9 years ago and coronary artery bypass grafting 20 years ago presented dyspnoea and slow-rising pulse with an aortic area ejection-systolic murmur on physical examination. Transthoracic echocardiogram showed a left-ventricular ejection fraction of 59%, aortic transvalvular peak/mean gradients of 6.7/4.1 mmHg, aortic valve area (AVA) of 1.91 cm^2^, and no aortic regurgitation (Figure 1A). The valve was not well-visualized on parasternal view due to acoustic shadowing from the frame, and all standard did not reveal any significant gradient. Owing to discrepancy between clinical and echocardiographic finding, cardiac catheterization was pursued, which showed patent grafts but an aortic peak/mean gradient of 110/69 mmHg with an AVA of 0.37 cm^2^ (Figure 1B). Heart team evaluation for suspected bioprosthetic valve degeneration had computed tomography (CT) done as part of the workup (Figure 1C), showing a vertical-take-off aortic accentuated by the CoreValve, with predicted coaxial alignment of the valve achievable from a left subcostal view (Figure 1D). Transthoracic echocardiogram from this off-axis view showed aortic transvalvular peak/mean gradients of 116/81 mmHg, AVA of 0.28 cm^2^ (Figure 1E). The patient had prohibitive surgical risk and underwent a valve-in-valve TAVI with a 20 mm Sapien 3 valve (Edwards Lifesciences, USA) (Figure 1F) per heart-team decision. This case demonstrates the importance of multimodality approach integrating clinical, imaging, and catheterization findings in diagnosing bioprosthetic degeneration when each modality alone has limitation.
Consent
Patient consent has been obtained for educational use of material, including publication.