Tumour resection and coronary artery bypass grafting for right ventricular fibroma with severe calcification and coronary artery stenosis
Yoshito Ito, Takahide Yoshio, Masao Daimon, Shinsuke Aida, Shuichiro Takanashi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
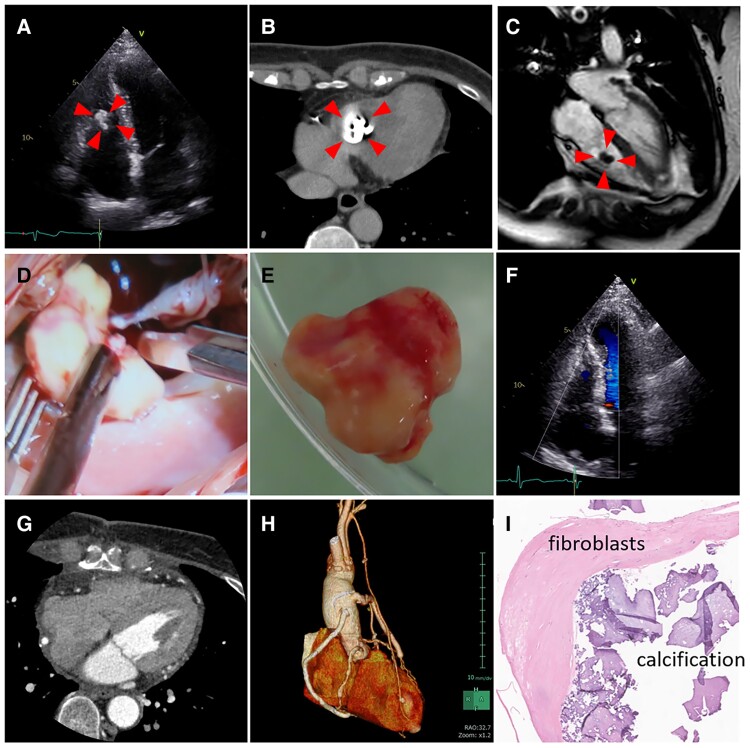 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Cardiac Structural Anomalies and Repair · Metal and Thin Film Mechanics
A 62-year-old female with familial hypercholesterolaemia, hypertension, and lower extremity artery disease presented with intermittent claudication. Although she had no cardiac complaints, cardiac workup was performed because she had multiple risk factors for ischaemic heart disease. Electrocardiogram showed no ischaemic signs or arrhythmia. Echocardiography showed a mobile, highly echogenic 12.7 × 7.3 mm right ventricular (RV) mass (Figure 1A, Supplementary data online, Videos S1–S3). Computed tomography (CT) and magnetic resonance imaging identified a calcified and mobile RV mass, which could be calcified amorphous tumour, calcified myxoma, or papillary fibroelastoma (Figure 1B and C, Supplementary data online, Videos S4–S6). Coronary angiography showed significant stenosis in the left main coronary artery, left anterior descending artery (LAD), left circumflex artery (LCX), and right coronary artery (RCA) (Supplementary data online, Videos S7–S9).
Resection of the RV mass and coronary artery bypass grafting (CABG) to LAD, diagonal branch, LCX, and RCA was performed. The mass, with marked calcification adhering to the anterior chordae of the tricuspid valve, was excised from the RV with preserving the chordae (Figure 1D and E). Post-operative imaging confirmed no residual mass, no worsened tricuspid regurgitation, and all graft patency (Figure 1F–H, Supplementary data online, Videos S10–S12). Histopathological examination revealed the mass was cardiac fibroma with calcification, characterized by fibroblasts and collagen fibres on haematoxylin-eosin staining (Figure 1I). A follow-up CT 1-year later showed no recurrence of the tumour and the patency of the graft.
Cardiac fibromas are rare benign tumours more common in childhood and typically found in the left ventricle. Cardiac fibromas of RV in adult are rare. Additionally, the mechanism of calcification in fibromas is unclear. While simultaneous fibroma resection and CABG have not been reported previously, predisposing factors for arterial sclerosis like ageing and dyslipidaemia may contribute to fibroma calcification.
Supplementary Material
qyae076_Supplementary_Data