Hydrodissection Facilitates Open Resection of Morton’s Neuroma Through a Plantar Approach: Technique Tip
Sufyan Faridi, Amanda Vandewint, Jacob Matz

TL;DR
This paper introduces a new surgical technique using hydrodissection to improve the removal of Morton’s neuroma through a plantar approach.
Contribution
The novel contribution is the use of hydrodissection to enhance visibility and precision during Morton’s neuroma resection.
Findings
Hydrodissection improves surgical access and reduces complications in Morton’s neuroma resection.
The plantar approach with hydrodissection allows for better visualization and preservation of surrounding structures.
This technique offers a refined method for orthopedic surgeons treating Morton’s neuroma.
Abstract
Visual AbstractThis is a visual representation of the abstract. This is a visual representation of the abstract.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1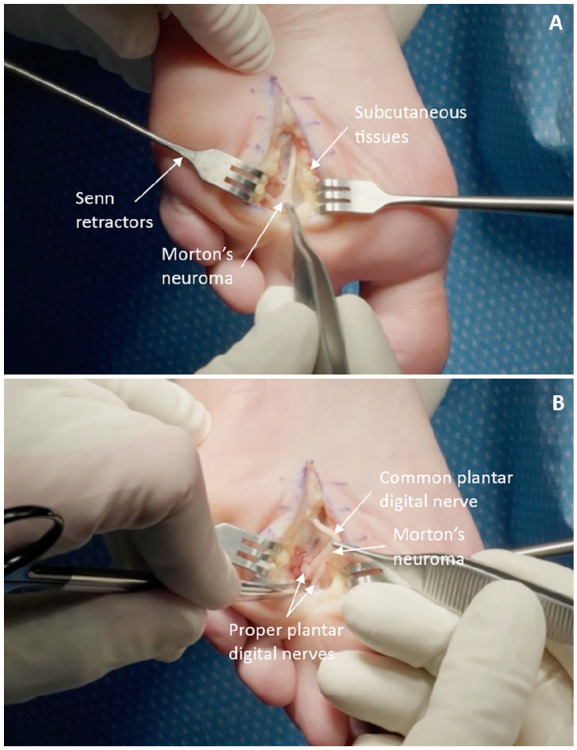 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Nerve Disorders · Nerve Injury and Rehabilitation · Orthopedic Surgery and Rehabilitation
Introduction
Morton’s neuroma is a condition characterized by benign thickening of the plantar digital nerves.^ 5 ^ This perineural fibrosis, primarily affecting the plantar digital nerves in the second and third intermetatarsal spaces, leads to neuropathic symptoms of radiating or burning pain, numbness in the toes, and a sensation of walking on a pebble.^ 4 ^
A common hurdle in the surgical management of Morton’s neuroma is the identification and resection of the neuroma without excessive dissection or damage to the surrounding soft tissue structures.^ 1 ^ In the quest for enhanced surgical outcomes, we propose hydrodissection as a promising adjunct technique. Hydrodissection involves the injection of fluid around the neuroma, creating a plane of separation between the neuroma and surrounding tissues.^ 3 ^ This technique has the potential to facilitate the subsequent surgical resection by enhancing the visualization and identification of the neuroma, thereby minimizing collateral tissue damage.
This technique tip describes the application of hydrodissection in the surgical management of Morton’s neuroma through a plantar approach, thus representing a novel modified approach to the treatment of this challenging condition.
Technique
Anesthesia for this procedure consists of either general anesthetic or awake surgery with a regional ankle block. The patient is secured in a semi-prone position with prepping and draping of the leg undertaken in a usual sterile fashion (Supplemental Video 1).^ 7 ^ An Esmarch ankle tourniquet is applied generating a pressure of approximately 300 mm Hg to achieve ischemia.
The two metatarsal heads between which the neuroma is located (ie, the second and third heads, or the third and fourth heads) are palpated, and a 3-4-cm-long, longitudinal incision is marked in the intermetatarsal space on the plantar aspect. A 10-mL syringe containing the hydrodissection solution of Marcaine 0.25% with epinephrine (1:200 000) is used to simultaneously confirm the placement of the mapped incision by palpating against the metatarsal shafts with the needle, while injecting the solution along the length of the intermetatarsal space (Figure 1). The injection begins at the level of the metatarsal cortex and is continued as the needle is withdrawn to the subcutaneous level. The injected fluid facilitates a hydrodissection process, whereby the nerve tissue will be more easily separated from the surrounding tissue. The epinephrine component of the solution provides the additional benefit of delivering improved hemostasis.
Hydrodissection step involving injection of 10 mL of Marcaine 0.25% with epinephrine solution (1:200 000) into the intermetatarsal space using a 25-gauge needle.
Following dissection of the skin and subcutaneous tissue, the nerve including the neuroma is exposed when separated out from the surrounding tissues, a step noticeably facilitated by the preceding hydrodissection component of the procedure (Figure 2). After excising the neuroma, the fatty tissue is reapproximated with 3-0 Monocryl followed by subcutaneous closure with 3-0 Monocryl. The skin is then evenly aligned with 3-0 Nylon sutures passed in a vertical mattress configuration. A soft dressing is applied and the operative foot is kept heel weightbearing for 3 weeks in a postoperative shoe followed by transition to weightbearing as tolerated in a regular shoe.^1,6^
(A) Visualization of the common plantar digital nerve with the Morton’s neuroma positioned at the distal end. (B) View of the bifurcation of the common plantar digital nerve distal to the site of the Morton’s neuroma into the proper plantar digital nerve branches.
Discussion
We propose in this technique tip that hydrodissection facilitates a more precise and efficient neuroma resection by creating a clear demarcation between the nerve tissue and the surrounding soft tissue structures. This precision is paramount, as it facilitates a more complete resection while minimizing the risk of collateral damage to surrounding tissues, potentially leading to reduced postoperative pain, faster recovery times, and decreased likelihood of recurrence.^1,2^
Complications associated with the plantar approach tend to be wound healing delays, hypertrophic scar formation, and paresthesias.^ 1 ^ The technique illustrated carries the potential of optimizing outcomes in several ways. First, by landmarking the incision during the injection process, the placement of the incision is optimized, avoiding areas of high pressure beneath the metatarsal heads. Second, by exploiting the potential space around the plantar nerve, hydrodissection has the potential of making the procedure more efficient, requiring less invasive dissection, which may help reduce the chances of wound healing complications. Finally, by making the identification of the neuroma simpler, the chances of an inadequate resection are reduced.
Early experiences in 6 patients using this hydrodissection technique have demonstrated its inclusion as beneficial. In comparison to the traditional technique previously used by the senior author, we find that hydrodissection allows for more efficient and less traumatic neuroma excision, with favorable postoperative outcomes. Although this technique demonstrates promising outcomes, it is imperative to consider the need for further research with larger cohorts and longer follow-up periods. These investigations will allow for better elucidation of the long-term benefits and possible complications associated with hydrodissection in the resection of Morton’s neuroma.
In conclusion, hydrodissection provides a simple novel adjunct to the surgical management of Morton’s neuroma that offers the potential of making neuroma identification and resection more efficient and reliable, while decreasing morbidity to adjacent structures.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241274778 – Supplemental material for Hydrodissection Facilitates Open Resection of Morton’s Neuroma Through a Plantar Approach: Technique TipSupplemental material, sj-pdf-1-fao-10.1177_24730114241274778 for Hydrodissection Facilitates Open Resection of Morton’s Neuroma Through a Plantar Approach: Technique Tip by Sufyan Faridi, Amanda Vandewint and Jacob Matz in Foot & Ankle Orthopaedics
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Åkermark C Crone H Skoog A Weidenhielm L . A prospective randomized controlled trial of plantar versus dorsal incisions for operative treatment of primary Morton’s neuroma. Foot Ankle Int. 2013;34(9):1198-204. doi:10.1177/107110071348430023564425 · doi ↗ · pubmed ↗
- 2Bucknall V Rutherford D Mac Donald D Shalaby H Mc Kinley J Breusch SJ . Outcomes following excision of Morton’s interdigital neuroma: a prospective study. Bone Joint J. 2016;98-B(10):1376-1381. doi:10.1302/0301-620X.98B 10.3761027694592 · doi ↗ · pubmed ↗
- 3Lam KHS Hung CY Chiang YP , et al. Ultrasound-guided nerve hydrodissection for pain management: rationale, methods, current literature, and theoretical mechanisms. J Pain Res. 2020;13:1957-1968. doi:10.2147/JPR.S 24720832801851 PMC 7414936 · doi ↗ · pubmed ↗
- 4Matthews BG Thomson CE Harding MP Mc Kinley JC Ware RS . Treatments for Morton’s neuroma. Cochrane Database Syst Rev. 2024;2(2):CD 014687. doi:10.1002/14651858.CD 014687.pub 2PMC 1085397238334217 · doi ↗ · pubmed ↗
- 5Morton TG . A peculiar and painful affection of the fourth metatarso-phalangeal articulation. Am J Med Sci. 1876;71(141):37-45.
- 6Nery C Raduan F Del Buono A Asaumi ID Maffulli N. Plantar approach for a Morton neuroma. JBJS Essent Surg Tech. 2012;2(3):e 14. doi:10.2106/JBJS.ST.L.00006 PMC 655407431321137 · doi ↗ · pubmed ↗
- 7Odutola A Clarke A Harries W Robinson S Hepple S Soar J. Clinical tip: semi-prone position for Achilles tendon surgery. Foot Ankle Int. 2007;28(10):1104-1105. doi:10.3113/FAI.2007.110417923065 · doi ↗ · pubmed ↗