A Systematic Review and Meta-Analysis of 35,409 Patients Undergoing PCI versus CABG for Unprotected Left Main Coronary Artery Diseases
Hao Liu, Dongdong Li, Chuncheng Gao, Huimiao Dai, Lin Kang, Mingming Zhang, Chen Yun, Wangang Guo

TL;DR
This study compares two heart treatments for a serious condition and finds that each has different risks and benefits.
Contribution
The study provides a comprehensive meta-analysis of 35,409 patients comparing PCI and CABG for UPLM disease.
Findings
CABG had lower major adverse events, mainly due to fewer revascularizations.
PCI had lower stroke rates and fewer deaths, heart attacks, and stent issues.
More research is needed to determine the best treatment strategy.
Abstract
Patients with unprotected left main (UPLM) disease who underwent percutaneous coronary intervention (PCI) were found to have inconsistent results compared to those treated with coronary artery bypass grafting (CABG). We identified and enrolled randomized controlled trials (RCTs) and observational studies (OSs) comparing PCI versus CABG for UPLM disease. A meta-analysis was performed using Stata 17.0. The primary endpoints were major adverse cardiovascular and cerebrovascular events (MACCEs). Additionally, all-cause death, cardiac death, myocardial infarction (MI), stroke, target vessel revascularization (TVR), and stent thrombosis (ST) were included as secondary endpoints. The odds ratios and 95% confidence intervals (CIs) were calculated. Sensitivity analyses were implemented if I2 > 50% or p < 0.01. Publication bias analysis was conducted if more than 10 studies were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
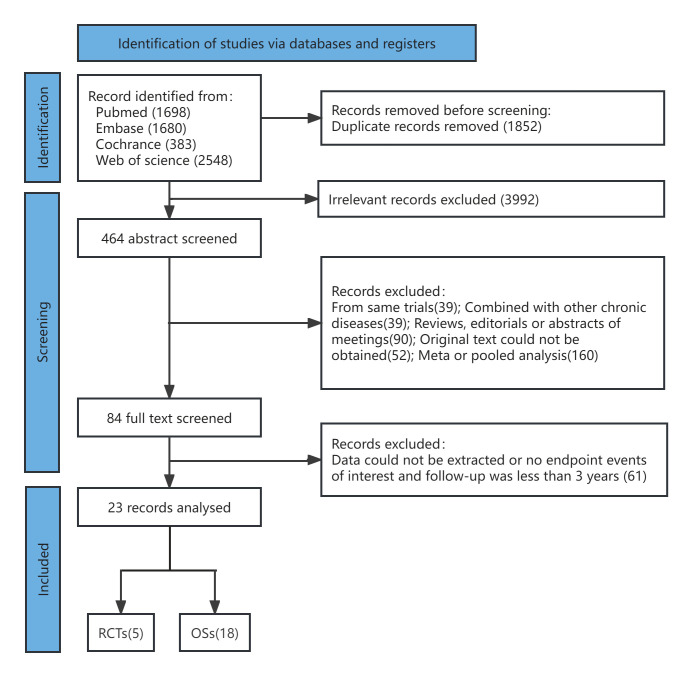 Fig. 1
Fig. 1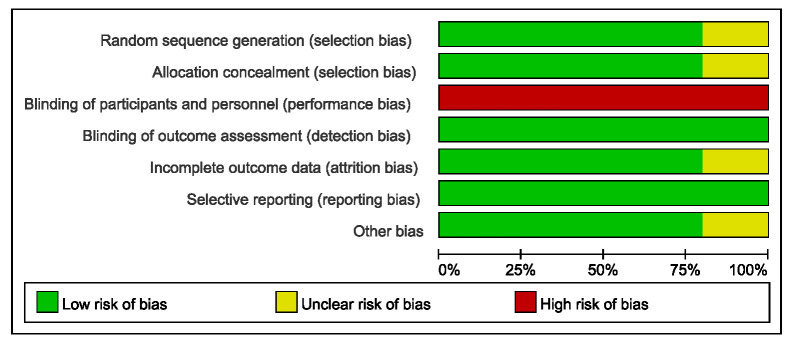 Fig. 2
Fig. 2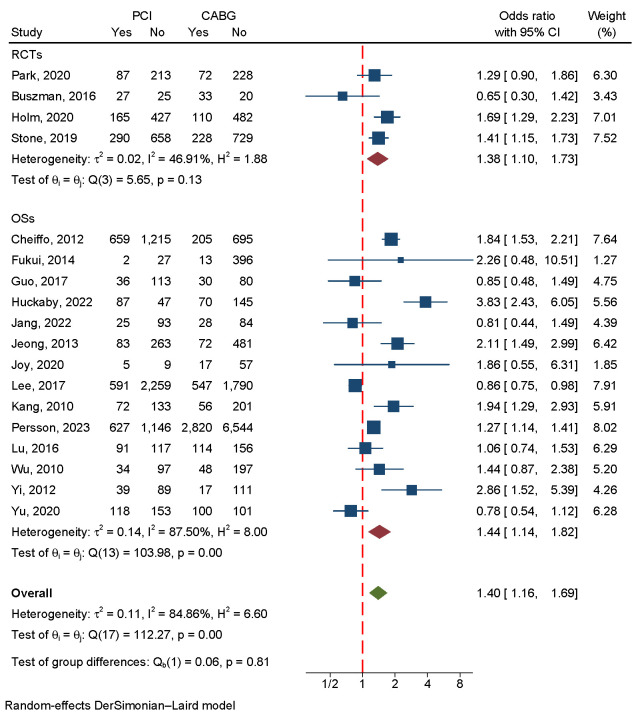 Fig. 3
Fig. 3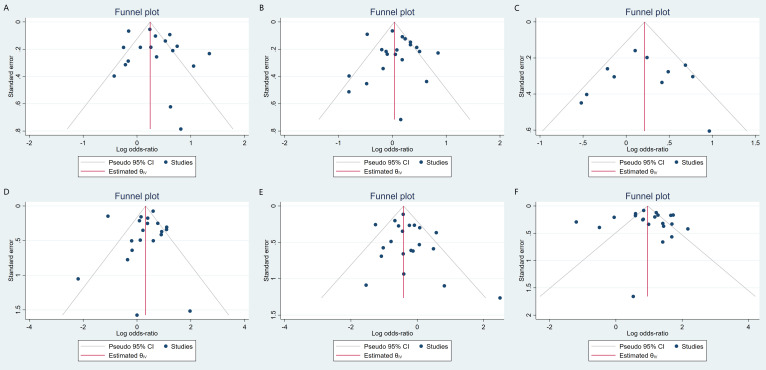 Fig. 4
Fig. 4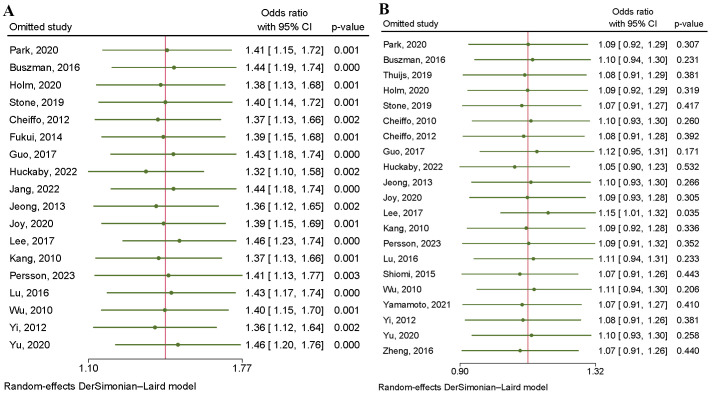 Fig. 5
Fig. 5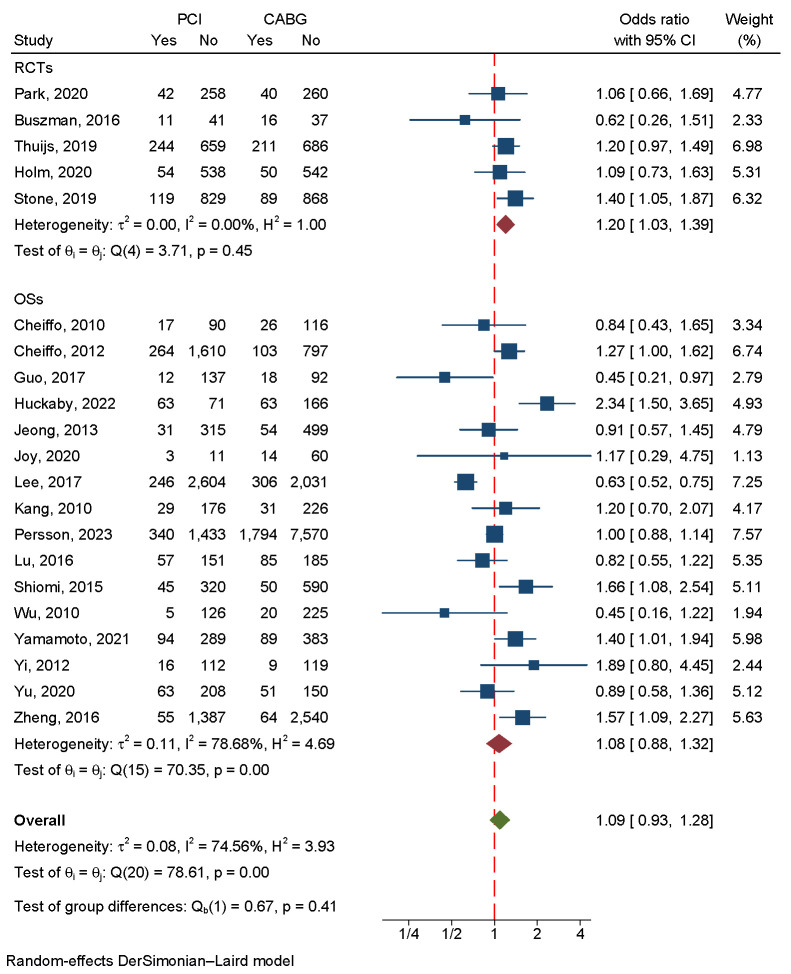 Fig. 6
Fig. 6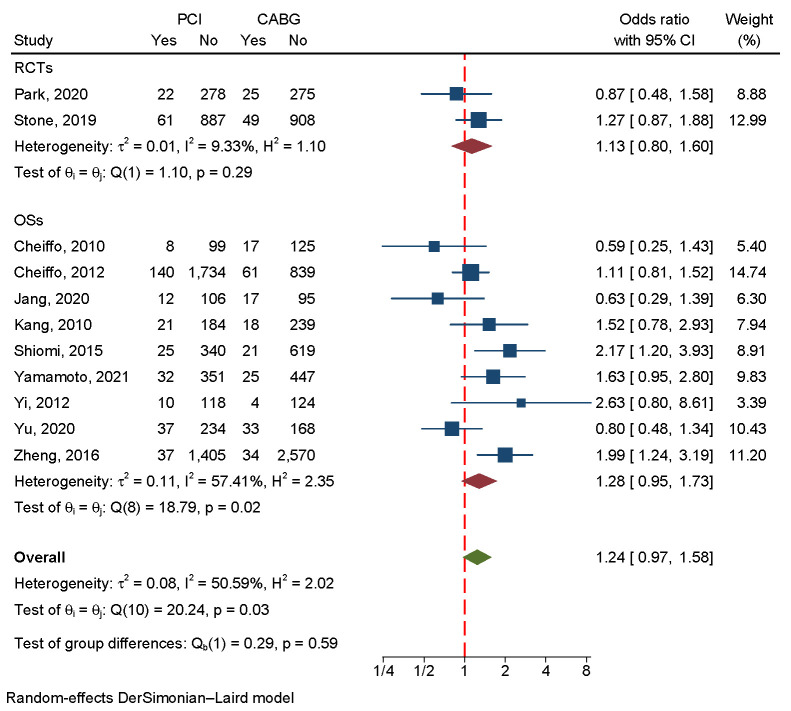 Fig. 7
Fig. 7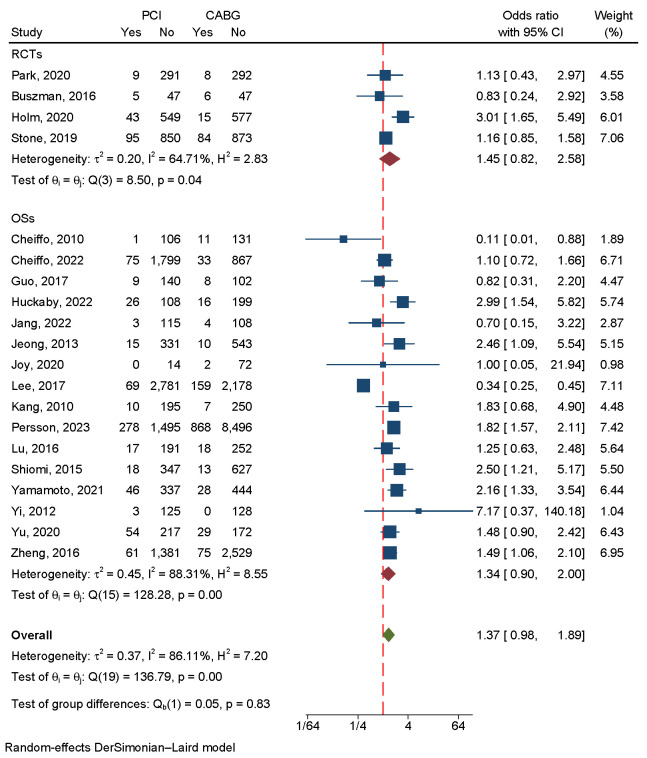 Fig. 8
Fig. 8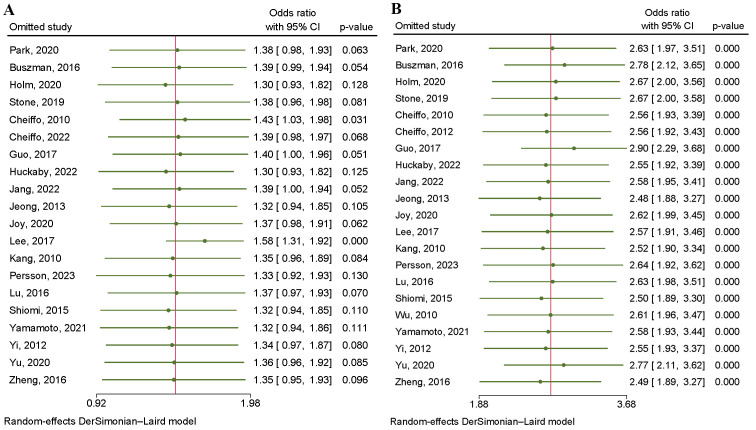 Fig. 9
Fig. 9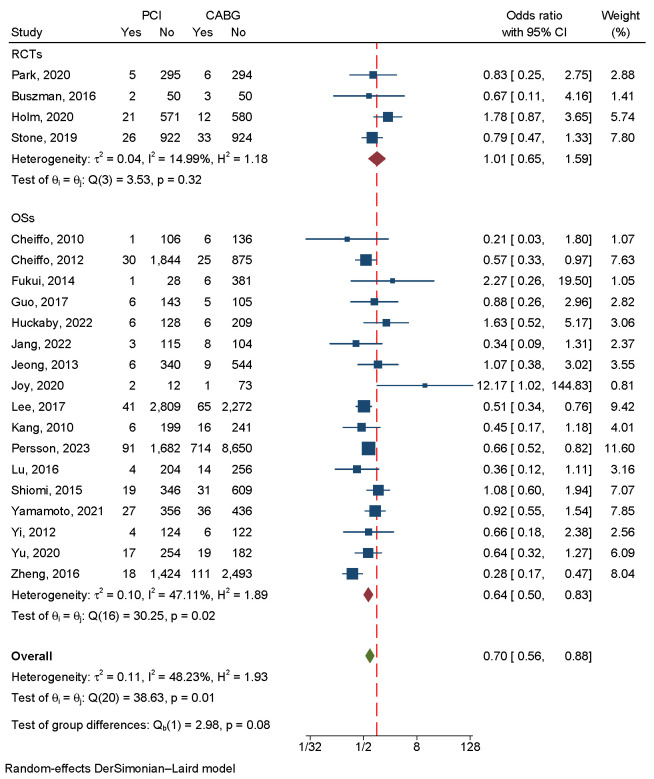 Fig. 10
Fig. 10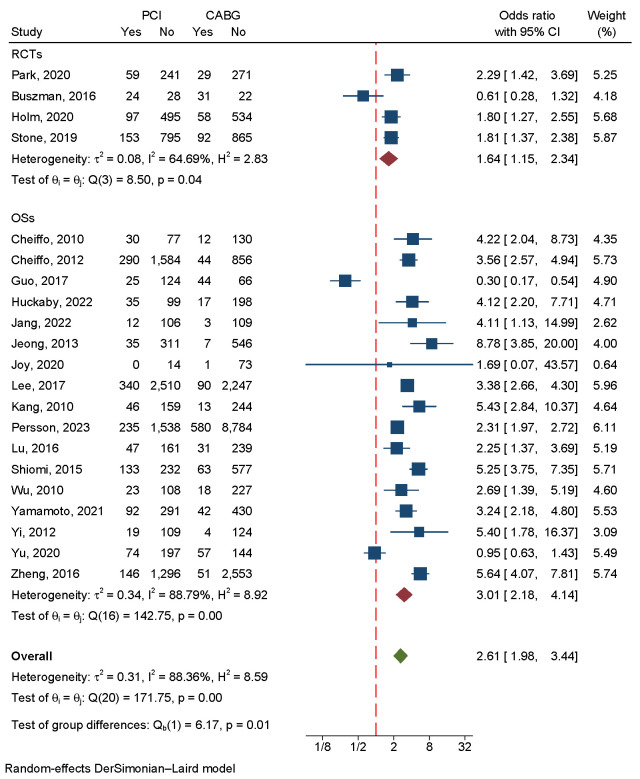 Fig. 11
Fig. 11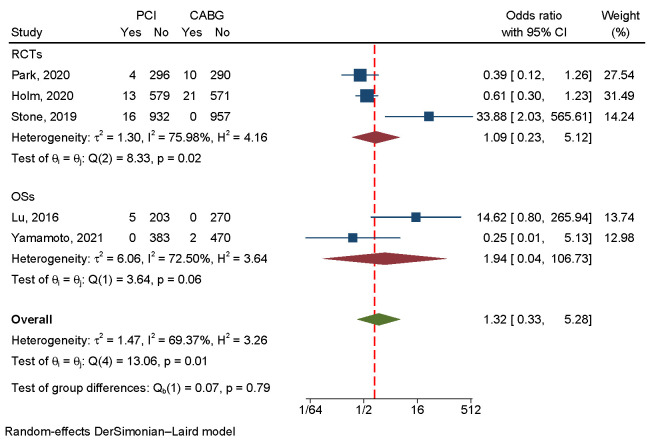 Fig. 12
Fig. 12| Study | Country/Territory | Center | Data from | Study period | Follow-up period | Study type |
| Park, | Korea | 13 centers | PRECOMBAT trial | Apr.2004–Aug.2009 | 1,2,5,10 years | RCT |
| Buszman, | America | Multi-center | LE MANS trial | 2001–2004 | 1,10 years | RCT |
| Thuijs, | 18 North America and European countries | 85 centers | SYNTAX trial | Mar.2005–Apr.2007 | 1,3,5,10 years | RCT |
| Holm, | 9 northern European countries | 36 centers | NOBLE trial | Dec.2009–Jan.2015 | 1,5 years | RCT |
| Stone, | 17 countries | 165 centers | EXCEL trial | Sep.2010–Mar.2014 | 3,5 years | RCT |
| Chieffo, | Milan | Single center | Local database | Mar.2002–Jul.2004 | 1,5 years | Non-RCT |
| Chieffo, | Milan | 14 centers | The DELTA registry | Apr.2002–Apr.2006 | 1295 days | Non-RCT |
| Fukui, | Japan | Single center | Local database | Jan.2005–Dec.2010 | 37.1 months | Non-RCT |
| Guo, | China | Single center | Local database | Jan.2003–Jul.2009 | 7.1 years | Non-RCT |
| Huckaby, | America | Multi-center | Local database | 2010–2018 | 5 years | Non-RCT |
| Jang, | Korea | Single center | Local database | Aug.2005–Apr.2013 | 7 years | Non-RCT |
| Jeong, | Korea | Single center | Local database | Jan.2001–Dec.2009 | 55.9 months | Non-RCT |
| Joy, | United Kingdom | Single center | Local database | Jan.2012–Dec.2012 | 5 years | Non-RCT |
| Lee, | 9 Asian territories | 50 centers | IRIS-MAIN registry | Jan.1995–Dec.2013 | 5.2 years | Non-RCT |
| Kang, | Korea | 2 centers | Local database | Jan.2003–Dec.2006 | 0.5,1,2,3 years | Non-RCT |
| Lu, | China | Single center | Local database | Jan.2004–Dec.2010 | 4.3 years | Non-RCT |
| Persson, | Sweden | 28 centers | SWEDENHEART registry | Jan.2005–Dec.2015 | 4.7 years | Non-RCT |
| Shiomi, | Japan | 26 centers | The CREDO-Kyoto PCI/CABG registry cohort-2 | Jan.2005–Dec.2007 | 3 years | Non-RCT |
| Wu, | China | Single center | Local database | Feb.2003–Dec.2006 | 4 years | Non-RCT |
| Yamamoto, | Japan | 22 centers | The CREDO-Kyoto PCI/CABG registry cohort-3 | Jan.2011–Dec.2013 | 5.5 years | Non-RCT |
| Yi, | Korea | Single center | Local database | Jul.2003–Jun.2007 | 38 months | Non-RCT |
| Yu, | China | Single center | Local database | Jan.2003–Jul.2009 | 12 years | Non-RCT |
| Zheng, | China | Single center | Local database | Jan.2004–Dec.2010 | 3 years | Non-RCT |
| Study | Sample size | Age, year | Male, % | DM, % | Hypertension, % | Dyslipidemia, % | Current smoker, % | Prior PCI, % | Prior MI, % |
| Park, | 300/300 | 61.8/62.7 | 76/77 | 34/30 | 54.3/51.3 | 42.3/40.0 | 29.7/27.7 | 12.7/12.7 | 4.3/6.7 |
| Buszman, | 52/53 | 60.0/61.3 | 60/73 | 19/17 | 75/70 | 65/60 | - | - | 37/32 |
| Thuijs, | 903/897 | 65.2/65.0 | 76/79 | 26/25 | 69/64 | 79/77 | 18/22 | - | 32/34 |
| Holm, | 592/592 | 66.2/66.2 | 80/76 | 15/15 | 65/66 | - | 19/22 | 20/20 | - |
| Stone, | 948/957 | 66.0/65.9 | 76.2/77.5 | 30.2/28.0 | 74.5/73.9 | 71.5/69.3 | 24.1/20.8 | 18.4/15.9 | 18.1/16.9 |
| Chieffo, | 107/142 | 63.6/67.5 | - | 18.7/23.2 | 58.8/76.0 | 70.0/69.0 | 49.5/59.1 | - | - |
| Chieffo, | 1874/900 | 65.8/66.5 | 73.9/63.6 | 27.7/34.0 | 64.0/67.7 | 61.8/64.7 | 45.2/42.7 | 24.8/13.7 | - |
| Fukui, | 29/409 | 69.4/69.1 | 79.3/76.8 | 41.4/37.7 | 69.0/64.3 | 75.9/61.6 | 27.6/55.0 | - | 20.7/35.7 |
| Guo, | 149/110 | 61.9/60.7 | 74.5/74.5 | 28.2/29.1 | 55.7/52.7 | 48.3/39.1 | 47.7/45.5 | - | 18.1/25.5 |
| Huckaby, | 134/215 | 74/74 | 64.9/64.6 | 41.0/41.9 | 88.1/88.0 | 82.8/88.4 | 17.2/16.0 | 35.1/35.0 | 46.3/47.4 |
| Jang, | 118/112 | 64.0/64.3 | 75/69 | 31/39 | 56/63 | 38/24 | 25/20 | 12/14 | 3/5 |
| Jeong, | 346/553 | 62.5/62.5 | 78.3/75.2 | 28.3/37.1 | 44.8/60.0 | 18.5/37.1 | 24.0/30.0 | 25.4/17.0 | 14.5/12.1 |
| Joy, | 14/74 | 69/71 | 92/71 | 12/14 | 36/29 | - | 14/0 | - | - |
| Lee, | 2850/2337 | 62.7/63.5 | 74.7/76.1 | 32.4/37.6 | 57.1/57.2 | 42.1/38.9 | 25.2/28.5 | 17.2/12.2 | 8.1/13.5 |
| Kang, | 205/257 | 64.2/65.7 | 70.2/73.9 | 37.6/43.6 | 63.4/67.3 | 54.6/59.5 | 43.4/49.4 | 22.4/3.5 | 4.4/3.1 |
| Persson, | 1773/9364 | 72.8/69.6 | 71.8/79.0 | 19.1/20.9 | 64.3/63.8 | 52.9/61.2 | 13.3/15.6 | 7.5/5.2 | 19.1/16.3 |
| Lu, | 208/270 | 70/69 | 84.1/85.6 | 47/46 | 78/83 | 54/50 | 50/67 | - | - |
| Shiomi, | 365/640 | 71.4/69.4 | 71/77 | 42/45 | 86/85 | - | 21/25 | - | 19/16 |
| Wu, | 131/245 | 61.9/63.6 | 76/83 | 27/29 | 65/62 | 32/31 | 8/11 | - | 12/15 |
| Yamamoto, | 383/472 | 72.3/70.2 | 75.2/79.7 | 42.6/48.7 | 82.5/81.4 | - | 17.8/14.0 | - | 19.8/18.6 |
| Yi, | 243/269 | 62.3/65.0 | 72/77 | 32.9/38.6 | 57.2/57.2 | - | - | - | - |
| Yu, | 271/201 | 61.7/60.6 | 74.2/76.1 | 28.8/28.9 | 56.1/50.2 | 49.8/38.8 | 48.3/46.2 | 14.0/11.9 | 17.3/26.9 |
| Zheng, | 1442/2604 | 59.9/62.2 | 78.6/82.0 | 24.1/31.0 | 54.2/64.3 | 50.1/59.1 | 46.5/53.6 | 22.5/9.7 | 23.6/38.1 |
| LVEF, % | EuroSCORE (PCI) | EuroSCORE (CABG) | SYNTAX score (PCI) | SYNTAX score (CABG) | LMCA only, % | LMCA+SVD, % | LMCA+DVD, % | LMCA+TVD, % | RCA involvement |
| 61.7 | 2.6 | 2.8 | 24.3 | 25.3 | 9.0/11.3 | 16.7/17.7 | 33.7/30.0 | 40.7/41.0 | - |
| 53.5 | 3.3 | 3.5 | 25.2 | 24.7 | 56/60 | 13/6 | 27/19 | 60/75 | - |
| EF | 3.8 | 3.8 | 28.4 | 29.1 | 12/14 | 19/20 | 31/30 | 38/35 | - |
| 60/60 | median, 2 | median, 2 | 22.5 | 22.4 | 81/81 | - | - | - | - |
| 57.0 | - | - | 20.6 | 20.5 | - | - | - | - | - |
| 52.0 | 4.4 | 4.3 | 28.8 | 29.4 | - | - | - | - | 40.4/69.0 |
| 53.8 | 4.9 | 5.1 | - | - | - | 64.6/84.2 | - | - | 36.5/69.7 |
| 56.3 | 8.8 | 7.6 | - | - | 20.7/2.9 | 44.8/8.1 | 13.8/24.9 | 20.7/64.1 | - |
| 64/62 | 5 (3–6) | 5 (3–6) | - | - | 18.1/6.4 | 26.8/15.5 | 30.2/27.3 | 24.8/50.9 | - |
| 55/53 | - | - | - | - | - | - | - | - | - |
| - | 1.4 | 1.9 | 20.7 | 33.1 | 15/3 | 27/9 | 31/38 | 26/51 | - |
| EF | - | - | 24 | 28 | - | - | - | - | - |
| 52 | - | - | 24 | 25 | - | - | - | - | - |
| 59.7 | - | - | - | - | 16.2/4.5 | 24.4/8.9 | 32.4/22.4 | 27.0/64.1 | - |
| 55.5 | 4.2 | 5.6 | - | - | 14.6/5.8 | 31.7/8.9 | 20.5/24.9 | 33.2/60.3 | 54.6/73.9 |
| - | - | - | - | - | 10.3/4.4 | 28.2/11.1 | 33.2/26.7 | 28.3/57.8 | - |
| 49 | 7.1 | 6.4 | - | - | 4.3/1.9 | 21/4.8 | 31/18 | 44/75 | 56/85 |
| EF | - | - | 26.5 (21–34) | 30 (22–40) | 8.5/8.9 | 24.5/16.9 | 36.0/28.4 | 31.0/45.8 | - |
| 60.0 | 4.2 | 4.3 | - | - | 9/3 | 18/4 | 38/26 | 35/67 | 44/82 |
| 59.4 | - | - | 27.5 (22–36) | 31 (23–38) | 6.5/0 | 24.8/1.3 | 33.2/26.9 | 35.5/71.8 | - |
| EF | - | - | - | - | - | - | - | - | - |
| 64/62 | 5 (3–6) | 5 (3–6) | - | - | 19.9/7.0 | 27.3/15.9 | 30.3/25.9 | 22.5/51.2 | - |
| 63.1 | 1.8 | 2.8 | 23.6 | 33.3 | 7.4/0.7 | 21.1/4.7 | 37.1/15.8 | 34.5/78.7 | 47.1/86.4 |
| Study | Selection | Comparability | Outcome | Total score |
| Chieffo, | ★★★ | ★★ | ★★★ | 8 |
| Chieffo, | ★★★ | ★★ | ★★★ | 8 |
| Fukui, | ★★★ | ★★ | ★★ | 7 |
| Guo, | ★★★ | ★★ | ★★ | 7 |
| Huckaby, | ★★★ | ★★ | ★★ | 7 |
| Jang, | ★★★ | ★★ | ★★ | 7 |
| Jeong, | ★★★ | ★★ | ★★★ | 8 |
| Joy, | ★★★★ | ★★ | ★★★ | 9 |
| Lee, | ★★★ | ★★ | ★★★ | 8 |
| Kang, | ★★★ | ★★ | ★★★ | 8 |
| Lu, | ★★★ | ★★ | ★★ | 7 |
| Persson, | ★★★ | ★★ | ★★ | 7 |
| Shiomi, | ★★★ | ★★ | ★★★ | 8 |
| Wu, | ★★★ | ★★ | ★★★ | 8 |
| Yamamoto, | ★★★ | ★★ | ★★ | 7 |
| Yi, | ★★★ | ★★ | ★★ | 7 |
| Yu, | ★★★ | ★★ | ★★ | 7 |
| Zheng, | ★★★ | ★★ | ★★★ | 8 |
| Aggregated OR (RCTs) | Aggregated OR (OSs) | Aggregated OR (Overall) | ||
| Primary endpoint | ||||
| MACCEs | 1.38* | 1.44* | 1.40* | |
| Secondary endpoints | ||||
| All-cause death | 1.20* | 1.08 | 1.09 | |
| Cardiac death | 1.13 | 1.28 | 1.24 | |
| MI | 1.45 | 1.34 | 1.37 | |
| Stroke | 1.01 | 0.64* | 0.70* | |
| TVR | 1.64* | 3.01* | 2.61* | |
| ST | 1.09 | 1.94 | 1.32 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Cardiac Imaging and Diagnostics · Acute Myocardial Infarction Research
1. Introduction
The left main coronary artery (LMCA) supplies approximately 75 percent of the myocardium in the left ventricle. Left main lesions tend to have worse long-term outcomes and higher death rates than non-left main lesions. Coronary artery bypass grafting (CABG) has long been considered the best treatment strategy for LMCA disease. With the development of stent technology, the assistance of intraoperative imaging, the optimization of anti-thrombotic strategy, and the application of new drugs, there is an increasing use of percutaneous coronary intervention (PCI), with it gradually becoming an alternative treatment option [1]. In the American College of Cardiology (ACC)/American Heart Association (AHA)/Society for Cardiovascular Angiography and Interventions (SCAI) jointly published guidelines for coronary artery revascularization in 2021, CABG is recommended over PCI when revascularization is required for complex left main coronary artery disease [2]. Several randomized controlled trials (RCTs) have been performed to determine the optimum revascularization strategy for LMCA patients. Several studies have, however, found conflicting results when analyzing long-term results [3, 4, 5, 6, 7, 8]. According to the SYNTAX trial, PCI and CABG have similar 10-year all-cause death rates; CABG provides a significant survival advantage for three-vessel disease patients but not for left main disease [6]. The LE-MAIN trial demonstrated a positive long-term outcome for stenting in patients with left main lesions with moderate to low complex coronary artery disease [7]. The MAIN-COMPARE 10-year study found that CABG is superior in terms of death rate and a composite of death, myocardial infarction (MI), or stroke [8]. Therefore, these results are conflicting.
We reviewed the literature to determine which revascularization strategy, PCI or CABG, was superior for treating patients with left main disease. This trial was registered on https://inplasy.com/ (INPLASY202390009).
2. Methods
2.1 Literature Search
We comprehensively searched PubMed, Embase, Cochrane Database, and Web of Science and analyzed RCTs and observational studies (OSs) that compared PCI versus CABG in patients with unprotected left main (UPLM) disease between the initiation of the database and June 30, 2023. The key search terms included “left main”, “percutaneous coronary intervention”, and “coronary artery bypass graft”. The terms were searched for using the free combination method. All the obtained references were evaluated and screened by reading abstracts or full texts, and the eligible references were included. The search strategy is “left main and percutaneous coronary intervention and coronary artery bypass graft”. Details are shown in Supplementary Table 1.
2.2 Literature Inclusion and Exclusion Criteria
Inclusion criteria were (1) RCTs and OSs comparing PCI and CABG for left main bifurcation lesions; (2) studies that contained comparable data about the two treatment strategies; (3) at least one major adverse cardiovascular and cerebrovascular event (MACCE), all-cause death, cardiac death, MI, stroke, target vessel revascularization (TVR), and stent thrombosis (ST) as study outcomes; (4) a follow-up period of at least three years.
Exclusion criteria were (1) endpoint events of interest not being clearly reported or could not be extracted and calculated and (2) studies based on the same patient cohort.
2.3 Data Extraction
We independently reviewed the literature and extracted relevant data from two reviewers in our research group (HL and DL). CG (third reviewer) assisted in resolving any disagreements. Data extracted from the enrolled studies include (1) basic information, including first author, year of publication, data source, follow-up time, and research type; (2) participants’ characteristics, including the size of the sample, the mean age, and the gender ratio; (3) the extent of left main disease according to whether the left anterior descending (LAD)/left circumflex (LCX)/right coronary artery (RCA) were involved, only the LMCA, LMCA+single vessel disease (SVD), LMCA+double vessel diseases (DVD), LMCA+third vessel diseases (TVD); (4) outcomes including MACCEs, all-cause death, cardiac death, MI, stroke, TVR, and ST; (5) other information such as EuroSCORE, and SYNTAX scores.
2.4 Outcomes and Definitions
MACCEs, a composite of death, MI, stroke, and TVR, were the primary endpoint of this meta-analysis. Studies enrolled in the review varied in composition, and the initial definition was adopted in this review. Supplementary Table 2 summarizes the definitions of all primary endpoints in each study. Components of ST and primary endpoint are secondary endpoints. These included all-cause death, cardiac death, MI, TVR, and stroke.
2.5 Risk Assessment of Bias
HL and DL conducted bias risk assessments. Any disparity was resolved through discussion with CG. The Cochrane Collaboration tool [9] was used to assess RCTs, while the Newcastle–Ottawa Quality Assessment Scale (NOS) [10] was used to assess OSs.
2.6 Statistical Analysis
Calculated odds ratios (OR) were based on 95% confidence intervals (CIs) using STATA/SE 17.0 (StataCorp LLC, College Station, TX, America). tests were used to examine heterogeneity between studies. Fixed-effects models were used in cases where *p * 0.01 and 50% rather than random-effects models. An analysis of heterogeneity and sensitivity was conducted to identify its origins. In the case of more than 10 studies, a regression-based Egger test was applied, and a non-parametric pruning and filling analysis was performed. p-values less than 0.05 were considered statistically significant.
3. Results
3.1 Baseline Data and Search Results
As shown in Fig. 1, four databases were searched to identify the enrolled studies. From the 6350 searched studies, 1852 were excluded for being duplicates and 3992 for being irrelevant records. In the 464 screened abstracts, 30 records were from the same trials. A total of 39 records were combined with other chronic diseases; 90 records belonged to reviews/editorials/meeting abstracts, the original text could not be obtained in 52 records, and 160 were meta- or pooled analyses. In the 84 screened papers with full texts, the data could not be extracted in 61, or they had no referred endpoint events and no follow-up over 3 years. Finally, 23 studies were enrolled. Among these studies, 18 had MACCEs data, 21 had data on all-cause death, 11 had data on cardiac death, 20 had data on MI, 21 had data on stroke, 21 had data on TVR, and 5 had data on ST. The included studies reported research results between 1995 and 2015, and the publication dates ranged from 2010 to 2023. In total, 35,409 patients were enrolled in our study. Table 1 (Ref. [3, 4, 5, 6, 7, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28]) lists the general characteristics of the studies. Table 2 (Ref. [3, 4, 5, 6, 7, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28]) provides detailed patient and procedure information.
Literature retrieval process. RCTs, randomized control trials; OSs, observational studies.
3.2 Study Quality Assessment
The Cochrane Collaboration tool was used to evaluate the quality of the RCTs. Fig. 2 shows the seven criteria for the five RCTs. In Table 3 (Ref. [11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28]), NOS judged all 18 observational studies to be low-risk.
RCTs quality assessment using the Cochrane Collaboration tool. RCTs, randomized control trials.
3.3 Primary Endpoint
Major Adverse Cardiac and Cerebrovascular Events
There was a significant difference between CABG and PCI in the four RCTs and 14 OSs that included 26,929 patients. Since there was a large amount of heterogeneity in the data ( = 84.86%, *p * 0.001), a random-effects model was used (Fig. 3). Neither a funnel plot nor a regression-based Egger test showed evidence of publication bias (p = 0.67) (Fig. 4A). According to the sensitivity analysis, heterogeneity was mainly caused by three studies [15, 20, 27] (Fig. 5A). Eliminating these three studies greatly reduced heterogeneity, and the subsequent results matched the primary results (Supplementary Fig. 1).
An analysis of the forest plots of major adverse cardiac and cerebrovascular events between PCI and CABG strategies. RCTs, randomized controlled trials; OSs, observational studies; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting.
Contour-enhanced funnel plots are used to evaluate the publication bias of studies about major adverse cardiac and cerebrovascular events (A), all-cause death (B), cardiac death (C), myocardial infarction (D), stroke (E), and stent thrombosis (F).
Heterogeneity of studies sensitivity analysis about major adverse cardiac and cerebrovascular events (A) and all-cause death (B).
3.4 Secondary Endpoints
3.4.1 All-Cause Death
A total of 35,505 patients were enrolled in five RCTs and 16 OSs. The results indicated that the CABG strategy was not statistically significant but associated with lower all-cause mortality. We used a random-effects model due to the large heterogeneity ( = 74.56%, *p * 0.001) (Fig. 6). Egger’s regression-based test and funnel plots showed no apparent publication bias (p = 0.40) (Fig. 4B). A sensitivity analysis revealed that heterogeneity was largely caused by three studies [15, 20, 23] (Fig. 5B). Eliminating these three studies greatly reduced heterogeneity, and the subsequent results matched the preceding results (Supplementary Fig. 2).
An analysis of the forest plots of all-cause death between the PCI and CABG strategies. RCTs, randomized controlled trials; OSs, observational studies; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting.
3.4.2 Cardiac Death
The incidence of cardiac death was assessed in two RCTs and nine OSs involving 12,854 patients. The results favored the CABG strategy for significantly lower cardiac death. Fixed-effect models were used because the heterogeneity was acceptable ( = 50.59%, p = 0.03) (Fig. 7). A regression-based Egger test and funnel plots revealed no publication bias (p = 0.88) (Fig. 4C).
An analysis of the forest plots of cardiac death between PCI and CABG strategies. RCTs, randomized controlled trials; OSs, observational studies; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting.
3.4.3 Myocardial Infarction
A total of 32,540 patients were included in four RCTs and 16 OSs to evaluate the incidence of MI. The overall effect showed that the CABG strategy has a lower incidence of myocardial infarction. As a result of the heterogeneity, a random-effects model was used ( = 86.11%, *p * 0.001) (Fig. 8). A regression-based Egger test and funnel plots revealed no publication bias (p = 0.66) (Fig. 4D). A sensitivity analysis revealed that heterogeneity was largely caused by three studies [5, 15, 20] (Fig. 9A). Eliminating these three studies greatly reduced heterogeneity, and the subsequent results matched the preceding results (Supplementary Fig. 3).
An analysis of the forest plots of myocardial infarction between PCI and CABG strategies. RCTs, randomized controlled trials; OSs, observational studies; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting.
Heterogeneity of studies sensitivity analysis about myocardial infarction (A) and target vessel revascularization (B).
3.4.4 Stroke
A total of 32,708 patients were included in four RCTs and 17 OSs investigating the incidence of stroke. The overall effect was found to be that the PCI strategy had a significantly lower incidence of stroke. Fixed-effects models were used because heterogeneity was relatively small ( = 48.23%, p = 0.01) (Fig. 10). A regression-based Egger test and funnel plots revealed no publication bias (p = 0.25) (Fig. 4E).
An analysis of the forest plots of stroke between PCI and CABG strategies. RCTs, randomized controlled trials; OSs, observational studies; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting.
3.4.5 Target Vessel Revascularization
A total of 32,646 patients were included in four RCTs and 17 OSs investigating the incidence of TVR. A significant advantage of CABG over PCI was found in the overall analysis. Since there was a large amount of heterogeneity in the data ( = 88.36%, p = 0.00), we used a random-effects model (Fig. 11). A regression-based Egger test and funnel plots revealed no publication bias (p = 0.79) (Fig. 4F). A sensitivity analysis revealed that heterogeneity was largely caused by the studies of Buszman 2016, Guo 2017, Jeong 2013, Yu 2020 and Zheng 2016 [7, 14, 17, 27, 28] (Fig. 9B). Eliminating these five studies greatly reduced heterogeneity, and the subsequent results matched the previous results (Supplementary Fig. 4).
An analysis of the forest plots of target vessel revascularization between PCI and CABG strategies. RCTs, randomized controlled trials; OSs, observational studies; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting.
3.4.6 Stent Thrombosis
Three RCTs and two OSs involving 5022 patients reported the incidence of ST. PCI and CABG did not show a significant difference in ST (Fig. 12). Due to the small number of included studies, funnel plot and sensitivity analyses were not performed.
An analysis of the forest plots of stent thrombosis between PCI and CABG strategies. RCTs, randomized controlled trials; OSs, observational studies; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting.
4. Discussion
This study included five RCTs and 18 OSs. For the primary endpoints of MACCEs, the PCI strategy was associated with a higher incidence of MACCEs, and there was a considerable degree of heterogeneity between strategies, which mainly occurred from the three OSs. The three OSs had conflicting conclusions regarding MACCEs, TVR, and all-cause death. We assumed that the heterogeneity of the three OSs may be closely related to their duration of follow-up. The study by Yu et al. (2020) [27] had a follow-up period of twelve years. Another two studies, Huckaby* et al. (2022) [15] and Lee et al*. (2017) [20], were followed for only five years. PCI might have shown an advantage after a longer follow-up period. In addition, these three studies made appropriate statistical adjustments to compensate for the non-randomized design of the observational study. However, some other factors that might have resulted in differences in clinical outcomes were not considered.
In subgroup analyses, MACCEs, cardiac death, MI, stroke, TVR, and ST were all consistently associated with aggregated ORs in RCTs and OSs. We did not identify publication bias when analyzing primary and secondary endpoint events. As shown in Table 4, the aggregated OR values of all endpoints indicated that the CABG strategy was associated with significantly lower MACCE rates, which were primarily driven by TVR. The PCI strategy was associated with significantly lower stroke rates. There was also a lower tendency for the CABG strategy to result in all-cause death, cardiac death, MI, and ST, although the differences were not statistically significant. Based on these results and considering the importance of survival, CABG might be a better strategy.
In 2023, Feng et al. [29] published a systematic review comparing the two multi-vessel coronary artery (MVCA) or left main (LM) strategies, including nine studies involving 8621 patients. In that review, CABG improved five-year survival among patients with MVCA but not in those with LM. Consequently, we compared PCI and CABG for UPLM disease patients based on their long-term prognosis. A recent study by Persson et al. [22] in 2023 was added to our review to enlarge the sample size.
Benedetto et al. [30] analyzed Bayesian networks for LM disease. According to this network meta-analysis, DES did not result in better PCI outcomes than CABG. Moreover, the results of current trials did not clarify whether drug-eluting stents (DESs) are as safe as CABG in patients with cardiovascular events. Therefore, further research involving the use of the new generation DESs for LM diseases is warranted to help clinicians determine the optimal strategy for managing UPLM disease.
Although CABG had fewer overall MACCEs in treating LM lesions, this advantage was mainly driven by ST and TVR, not all-cause death. This might have been because the combined effects of CABG surgery, anesthesia, and cardiopulmonary bypass offset its advantage in coronary revascularization. Since there was an increase in mortality in patients undergoing CABG, PCI is often recommended as the therapy of choice. Drug-eluted balloon therapy may provide an advantage for PCI since it acts as a bridge to facilitate stent implantation in the stenotic vessel. At present, proprotein convertase subtilisin/kexin 9 (PCSK9) inhibitors and PCSK9 small interfering ribonucleic acid (siRNA) drugs have shown excellent results in preventing cardiovascular events in coronary heart disease. With the popularization of endovascular imaging technology, TVR may be further reduced when PCI is adopted. The widespread use of novel oral antiplatelet agents in LM may also further reduce the risk of ST. In conclusion, minimally invasive strategies have a significant role in treating LM lesions, although technical issues still need to be resolved.
5. Limitations
A major limitation in our review is the variable definition of endpoints across the studies. The study period only ranged from 1995 to 2015, and a few randomized controlled trials were included. The data extracted was only at the time of publication. SYNTAX scores and the EuroSCORE have been regarded as important predictors of cardiovascular survival; however, we could not better analyze the outcomes after PCI or CABG due to the limited data. Another weakness is that the limitations of the observational studies themselves cannot account for the preferences of physicians in selecting treatment strategies, which indirectly results in patients being given CABG or PCI. Finally, this review not have a prepared study protocol.
6. Conclusions
MACCE rates were significantly lower in patients who underwent CABG, primarily due to TVR, but stroke rates were higher. RCTs need to be further investigated to determine the most effective strategy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee PH Ahn JM Chang M Baek S Yoon SH Kang SJ et al Left Main Coronary Artery Disease: Secular Trends in Patient Characteristics, Treatments, and Outcomes Journal of the American College of Cardiology 201668123312462760968710.1016/j.jacc.2016.05.089 · doi ↗ · pubmed ↗
- 2Lawton JS Tamis-Holland JE Bangalore S Bates ER Beckie TM Bischoff JM et al 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation 2022145 e 4e 173488243610.1161/CIR.0000000000001039 · doi ↗ · pubmed ↗
- 3Stone GW Kappetein AP Sabik JF Pocock SJ Morice MC Puskas J et al Five-Year Outcomes after PCI or CABG for Left Main Coronary Disease New England Journal of Medicine 2019381182018303156279810.1056/NEJ Moa 1909406 · doi ↗ · pubmed ↗
- 4Park DW Ahn JM Park H Yun SC Kang DY Lee PH et al Ten-Year Outcomes After Drug-Eluting Stents Versus Coronary Artery Bypass Grafting for Left Main Coronary Disease: Extended Follow-Up of the PRECOMBAT Trial Circulation 2020141143714463222356710.1161/CIRCULATIONAHA.120.046039 · doi ↗ · pubmed ↗
- 5Holm NR Mäkikallio T Lindsay MM Spence MS Erglis A Menown IBA et al Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: updated 5-year outcomes from the randomised, non-inferiority NOBLE trial Lancet (London, England) 20203951911993187902810.1016/S 0140-6736(19)32972-1 · doi ↗ · pubmed ↗
- 6Thuijs DJFM Kappetein AP Serruys PW Mohr FW Morice MC Mack MJ et al Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial Lancet (London, England) 2019394132513343148837310.1016/S 0140-6736(19)31997-X · doi ↗ · pubmed ↗
- 7Buszman PE Buszman PP Banasiewicz-Szkróbka I Milewski KP Żurakowski A Orlik B et al Left Main Stenting in Comparison With Surgical Revascularization: 10-Year Outcomes of the (Left Main Coronary Artery Stenting) LE MANS Trial JACC. Cardiovascular Interventions 201693183272689208010.1016/j.jcin.2015.10.044 · doi ↗ · pubmed ↗
- 8Park DW Ahn JM Yun SC Yoon YH Kang DY Lee PH et al 10-Year Outcomes of Stents Versus Coronary Artery Bypass Grafting for Left Main Coronary Artery Disease Journal of the American College of Cardiology 201872281328223026123610.1016/j.jacc.2018.09.012 · doi ↗ · pubmed ↗