The Association between Cardiac Arrest and Mortality in Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock
Qian-feng Xiao, Xin Wei, Si Wang, Ying Xu, Yan Yang, Fang-yang Huang, Mao Chen

TL;DR
This study finds that cardiac arrest at admission does not significantly affect survival in patients with heart attacks complicated by cardiogenic shock.
Contribution
The study provides new evidence that cardiac arrest at admission is not a significant predictor of mortality in AMI-CS patients.
Findings
Cardiac arrest at admission was not a significant risk factor for 30-day or 1-year mortality in AMI-CS patients.
The IABP-SHOCK II score showed better predictive performance than the GRACE score for mortality in these patients.
Adding cardiac arrest status did not improve the predictive value of the IABP-SHOCK II score.
Abstract
The impact of cardiac arrest (CA) at admission on the prognosis of patients with acute myocardial infarction (AMI) complicated by cardiogenic shock (CS) remains a subject of debate. We conducted a retrospective study at West China Hospital from 2018 to 2021, enrolling 247 patients with AMI complicated by CS (AMI-CS). Patients were categorized into CA and non-CA groups based on their admission status. Univariate and multivariate Cox regression analyses were performed, with 30-day and 1-year mortality as the primary endpoints. Kaplan–Meier plots were constructed, and concordance (C)-indices of the Global Registry of Acute Coronary Event (GRACE) score, Intra-aortic Balloon Pump in Cardiogenic Shock (IABP-SHOCK) II score, and IABP-SHOCK II score with CA were calculated. Among the enrolled patients, 39 experienced CA and received cardiopulmonary resuscitation at admission. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
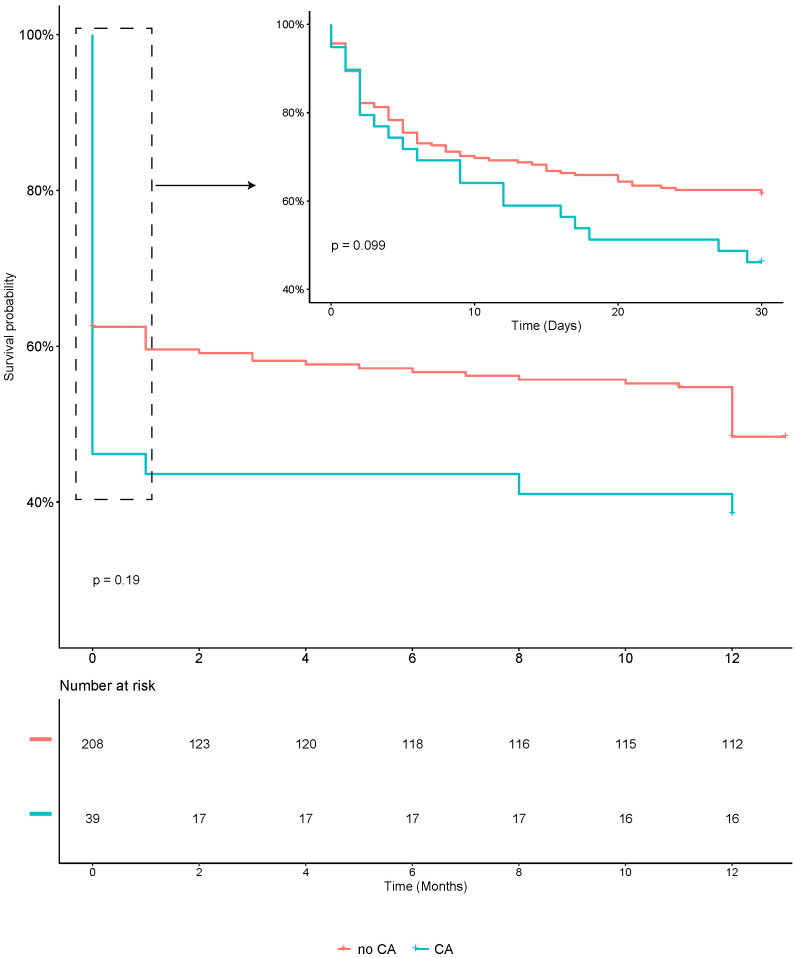 Fig. 1
Fig. 1| Total (n = 247) | CA group (n = 39) | Non-CA group (n = 208) | |||
| Demographic data | |||||
| Age, yrs | 68 (30–89) | 66 (30–89) | 69 (32–89) | 0.281 | |
| Male | 184/247 (74.5) | 29/39 (74.4) | 155/208 (74.6) | 0.983 | |
| BMI, kg/ | 23.4 (13.9–35.6) | 23.7 (16.8–31.3) | 23.4 (13.9–35.6) | 0.613 | |
| SBP, mmHg | 91 (51–135) | 87 (52–122) | 92 (51–135) | 0.044 | |
| MAP, mmHg | 70.7 (40.7–105) | 65.6 (40.7–100) | 71.7 (41–105) | 0.002 | |
| Heart rate, bpm | 97 (39–180) | 100 (52–180) | 96 (39–151) | 0.305 | |
| Cardiovascular risk factors/CVD (%) | |||||
| Smoking | 115/247 (46.6) | 20/39 (51.3) | 95/208 (45.7) | 0.519 | |
| Arterial hypertension | 119/247 (48.2) | 13/39 (33.3) | 106/208 (50.9) | 0.043 | |
| Diabetes mellitus | 77/247 (31.2) | 9/39 (23.1) | 68/208 (32.7) | 0.234 | |
| History of CAD | 48/247 (19.4) | 7/39 (17.9) | 41/208 (19.7) | 0.798 | |
| History of Stroke | 19/247 (7.7) | 2/39 (5.1) | 17/208 (8.2) | 0.513 | |
| Dyslipidemia | 40/247 (16.3) | 3/39 (7.7) | 37/208 (17.8) | 0.116 | |
| Known PAD | 7/247 (2.8) | 0/39 (0) | 7/208 (3.4) | 0.245 | |
| CKD | 19/247 (7.7) | 2/39 (5.1) | 17/214 (8.2) | 0.513 | |
| Laboratory results | |||||
| Arterial lactate, mmol/L | 4.7 (1.0–20) | 6.9 (1.1–20) | 4.3 (1.0–20) | 0.004 | |
| Glucose, mmol/L | 12.06 (3.17–37.47) | 13.34 (3.17–37.47) | 11.82 (3.59–35.91) | 0.176 | |
| Serum creatinine, µmol/L | 149.9 (51–1014) | 177.4 (57–665) | 144.7 (51–1014) | 0.094 | |
| TnT, ng/L | 7295.6 (97.3–10,000) | 7346.7 (699–10,000) | 7285.9 (97.3–10,000) | 0.906 | |
| STEMI (%) | 175/247 (70.9) | 30/39 (76.9) | 145/208 (69.7) | 0.363 | |
| Anterior STEMI (%) | 112/247 (45.3) | 25/39 (64.1) | 87/208 (41.8) | 0.010 | |
| Ventilation (%) | 186/247 (75.3) | 36/39 (92.3) | 150/208 (72.1) | 0.007 | |
| CAG (%) | 221/247 (89.5) | 34/39 (87.2) | 187/208 (89.9) | 0.611 | |
| Coronary lesions (%) | 0.069 | ||||
| Mono-vessel disease | 55/219 (25.1) | 12/34 (35.3) | 43/185 (23.2) | ||
| Bi-vessel disease | 61/219 (27.9) | 9/34 (26.5) | 52/185 (28.1) | ||
| Multi-vessel disease | 103/219 (47.0) | 13/34 (38.2) | 90/185 (48.7) | ||
| Revascularization (%) | 198/247 (80.2) | 34/39 (87.2) | 164/208 (79.4) | 0.231 | |
| Complete revascularization (%) | 94/247 (38.1) | 18/39 (46.1) | 76/208 (36.5) | 0.256 | |
| TIMI flow grade 3 after PCI (%) | 184/221 (83.3) | 29/34 (85.2) | 155/187 (82.9) | 0.730 | |
| IABP (%) | 104/247 (42.1) | 23/39 (59.0) | 81/208 (38.9) | 0.020 | |
| ECMO (%) | 6/247 (2.4) | 2/39 (5.1) | 4/208 (1.9) | 0.233 | |
| GRACE score | 193 (122–265) | 215 (157–265) | 189 (122–237) | 0.000 | |
| IABP-SHOCK II score (%) | 0.130 | ||||
| 0–2 | 137/219 (62.6) | 17/35 (48.6) | 120/184 (65.2) | ||
| 3–4 | 54/219 (24.6) | 9/35 (25.7) | 45/184 (24.5) | ||
| 5–9 | 28/219 (12.8) | 9/35 (25.7) | 19/184 (10.3) | ||
| LVEF, % | 40 (15–75) | 41 (16–75) | 40 (15–70) | 0.856 | |
| Total | CA group | Non-CA group | ||
| Death within 30 days (%) | 101/247 (40.9) | 21/39 (53.9) | 80/208 (38.5) | |
| Cardiac death | 94/101 (93.1) | 20/21 (95.2) | 74/80 (92.5) | |
| Non-cardiac death | 7/101 (6.9) | 1/21 (4.8) | 6/80 (7.5) | |
| Death within 1 year (%) | 116/247 (47.0) | 23/39 (59.0) | 93/208 (44.7) | |
| Cardiac death | 106/116 (91.4) | 20/23 (87.0) | 86/93 (92.5) | |
| Non-cardiac death | 10/116 (8.6) | 3/23 (13.0) | 7/93 (7.5) | |
| Brain injury (%) | 12/247 (4.9) | 10/39 (25.6) | 2/208 (1.0) | |
| CPC score (1–3) | 3/247 (1.2) | 3/39 (7.7) | 0/208 (0) | |
| CPC score (4–5) | 9/247 (3.7) | 7/39 (17.9) | 2/208 (1.0) | |
| Univariable analysis of 30-day mortality | Multivariable analysis of 30-day mortality | |||
| HR (95% CI) | HR (95% CI) | |||
| Male | 0.51 (0.34–0.77) | 0.001 | ||
| Age, yrs | 1.04 (1.02–1.06) | 0.000 | 1.04 (1.02–1.06) | 0.001 |
| BMI, kg/ | 0.97 (0.91–1.03) | 0.293 | ||
| SBP, mmHg | 0.98 (0.97–1.00) | 0.011 | ||
| MAP, mmHg | 0.96 (0.95–0.98) | 0.003 | ||
| Heart rate, bpm | 1.01 (1.00–1.02) | 0.009 | ||
| CA | 1.48 (0.92–2.40) | 0.108 | 0.88 (0.48–1.60) | 0.669 |
| Ventilation | 14.4 (4.58–45.6) | 0.000 | 9.84 (2.38–40.7) | 0.002 |
| Arterial hypertension | 2.36 (1.57–3.55) | 0.000 | ||
| Diabetes mellitus | 1.38 (0.92–2.06) | 0.122 | ||
| History of CAD | 1.05 (0.65–1.72) | 0.835 | ||
| History of stroke | 1.07 (0.52–2.19) | 0.862 | ||
| Dyslipidemia | 0.98 (0.58–1.68) | 0.952 | ||
| Known PAD | 1.50 (0.55–4.08) | 0.427 | ||
| CKD | 2.28 (1.27–4.08) | 0.006 | ||
| Arterial lactate, mmol/L | 1.15 (1.11–1.19) | 0.000 | 1.15 (1.09–1.20) | 0.000 |
| Glucose, mmol/L | 1.06 (1.03–1.08) | 0.000 | ||
| Serum creatinine, µmol/L | 3.18 (2.37–4.26) | 0.000 | 2.24 (1.43–3.52) | 0.000 |
| TnT, ng/L | 1.000 (0.999–1.001) | 0.612 | ||
| STEMI | 0.76 (0.50–1.14) | 0.178 | ||
| Anterior STEMI | 0.98 (0.66–1.45) | 0.930 | ||
| Revascularization | 0.26 (0.17–0.39) | 0.000 | ||
| Complete revascularization | 0.45 (0.29–0.70) | 0.000 | ||
| TIMI flow grade 3 after PCI | 0.17 (0.11–0.28) | 0.000 | 0.20 (0.11–0.31) | 0.000 |
| IABP | 1.17 (0.79–1.73) | 0.428 | ||
| ECMO | 3.77 (1.65–8.33) | 0.002 | ||
| LVEF, % | 0.96 (0.94–0.98) | 0.000 | ||
| GRACE score | 1.03 (1.02–1.04) | 0.000 | ||
| IABP-SHOCK II score | 1.64 (1.47–1.83) | 0.000 | ||
| Univariable analysis of 1 year mortality | Multivariable analysis of 1 year mortality | |||
| HR (95% CI) | HR (95% CI) | |||
| Male | 0.55 (0.37–0.81) | 0.002 | ||
| Age, yrs | 1.03 (1.02–1.05) | 0.000 | 1.03 (1.01–1.05) | 0.010 |
| BMI, kg/ | 0.95 (0.90–1.00) | 0.066 | ||
| SBP, mmHg | 0.99 (0.97–1.00) | 0.07 | ||
| MAP, mmHg | 0.97 (0.96–0.99) | 0.001 | ||
| Heart rate, bpm | 1.01 (1.00–1.02) | 0.005 | ||
| CA | 1.43 (0.90–2.25) | 0.127 | 1.04 (0.59–1.85) | 0.881 |
| Ventilation | 6.42 (3.13–13.2) | 0.000 | 3.56 (1.60–7.91) | 0.002 |
| Arterial hypertension | 2.39 (1.64–3.50) | 0.000 | 1.60 (1.01–2.52) | 0.045 |
| Diabetes mellitus | 1.42 (0.98–2.08) | 0.06 | ||
| History of CAD | 1.05 (0.67–1.66) | 0.829 | ||
| History of Stroke | 1.04 (0.53–2.05) | 0.915 | ||
| Dyslipidemia | 0.95 (0.57–1.57) | 0.837 | ||
| Known PAD | 1.33 (0.49–3.60) | 0.579 | ||
| CKD | 2.01 (1.13–3.59) | 0.018 | ||
| Baseline arterial lactate, mmol/L | 1.15 (1.11–1.19) | 0.000 | 1.12 (1.07–1.18) | 0.000 |
| Baseline glucose, mmol/L | 1.06 (1.03–1.08) | 0.000 | ||
| Baseline serum creatinine, µmol/L | 2.97 (2.21–4.00) | 0.000 | 2.08 (1.37–3.15) | 0.001 |
| TnT, ng/L | 1.11 (0.85–1.44) | 0.435 | ||
| STEMI | 0.75 (0.51–1.10) | 0.144 | ||
| Anterior STEMI | 0.91 (0.63–1.32) | 0.622 | ||
| Revascularization | 0.29 (0.19–0.43) | 0.000 | ||
| Complete revascularization | 0.42 (0.28–0.65) | 0.000 | ||
| TIMI flow grade 3 after PCI | 0.21 (0.13–0.33) | 0.000 | 0.23 (0.14–0.37) | 0.000 |
| IABP | 1.21 (0.84–1.74) | 0.317 | ||
| ECMO | 3.65 (1.60–8.35) | 0.002 | ||
| LVEF, % | 0.96 (0.94–0.98) | 0.000 | ||
| GRACE score | 1.03 (1.02–1.03) | 0.000 | ||
| IABP-SHOCK II score | 1.59 (1.43–1.76) | 0.000 | ||
| Models to predict 30-day death | Models to predict 1 year death | |||
| AUC (95% CI) | AUC (95% CI) | |||
| GRACE score | 0.69 (0.64–0.75) | 0.000 | 0.67 (0.62–0.72) | 0.000 |
| IABP-SHOCK II score | 0.79 (0.74–0.84) | 0.000 | 0.76 (0.71–0.81) | 0.000 |
| IABP-SHOCK II score + CA | 0.79 (0.74–0.84) | 0.000 | 0.76 (0.71–0.81) | 0.000 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrest and Resuscitation · Mechanical Circulatory Support Devices · Cardiac Structural Anomalies and Repair
1. Introduction
Acute myocardial infarction (AMI) complicated by cardiogenic shock (CS) presents a formidable challenge in clinical practice, possessing a mortality rate of approximately 40–50% [1]. Notably, AMI patients with cardiac arrest (CA) are more prone to developing CS. In the subset of AMI complicated by CS (AMI-CS), the incidence of CA ranges from 28.5 to 51% [2, 3, 4, 5], and CA is frequently inferred as the primary cause of death in cases of AMI complicated by CS [6].
While previous studies have established CA as a significant risk factor for mortality in patients with acute coronary syndrome (ACS) [7, 8, 9, 10], this association exhibits inconsistency within AMI-CS patients [2, 3, 11]. Some studies suggest that CA may not independently influence all-cause in-hospital or long-term mortality among patients hospitalized with AMI-CS [2, 3]. Notably, these studies reported low proportions of coronary angiography (61.3%) and revascularization (53.3%), potentially compromising the survival probability of CA patients [2, 3]. In contrast, a comprehensive registry study demonstrated higher rates of coronary angiography (88.8%) and revascularization (77.2%) in AMI-CS patients [12].
Recent advancements in acute percutaneous coronary intervention (PCI) and circulatory support devices have significantly improved the short-term prognosis of AMI patients, particularly through early revascularization [1]. Consequently, in the context of active revascularization, the association between CA and the prognosis of patients with AMI-CS has become a subject of debate. In this study, we aimed to assess the impact of CA on AMI-CS outcomes by analyzing data collected from September 2018 to November 2021. Notably, the study cohort exhibited high proportions of coronary angiography (89.5%) and revascularization (80.2%), providing valuable insights into the contemporary landscape of AMI-CS management.
2. Methods
2.1 Study Population and Definitions
This retrospective study involved 247 patients diagnosed with AMI-CS treated at the West China Hospital of Sichuan University between September 2018 and November 2021. The inclusion criteria encompassed patients within the Society for Cardiovascular Angiography and Interventions (SCAI) shock stages B to E [12, 13]. Cardiac shock was defined as a primary cardiac disorder leading to hypotension (systolic blood pressure 90 mmHg, or vasopressors required to achieve a systolic blood pressure 90 mmHg) persisting for over 30 minutes, accompanied by signs of organ hypoperfusion (e.g., altered mental status, oliguria, cold and clammy skin, increased arterial lactate above 2 mmol/L) in a state of normovolemia or hypervolemia [11]. The cardiogenic shock severity was classified according to the SCAI shock stage [12, 13]. Stage B marked the initial phase of CS, identifying patients with clinical evidence of hemodynamic instability (relative hypotension or tachycardia) without hypoperfusion. Stage C denoted classic CS, where patients exhibited hypoperfusion requiring one intervention (pharmacological or mechanical), and lactate was 2 mmol/L. Stage D represented deteriorating CS, akin to category C but worsening, with failure of the initial support strategy evident through deteriorating hemodynamics or rising lactate. Stage E indicates the end stage of CS, characterized by actual or impending circulatory collapse. AMI was diagnosed according to the fourth universal definition of myocardial infarction [14]. Criteria included the detection of cardiac troponin values rising and/or falling, with at least one value surpassing the 99th percentile upper reference limit, and the simultaneous presence of symptoms of acute myocardial ischemia, new ischemic ECG changes, development of pathological Q waves, imaging evidence of new myocardial damage, or identification of a coronary thrombus. Cardiac arrest was defined as asystole, pulseless electrical activity, ventricular fibrillation, or pulseless ventricular tachycardia (VT) [3]. CS could still occur due to long-time cardiopulmonary resuscitation (CPR), mechanical complications, and VT storm after AMI, and most continuous CPR patients had no return of spontaneous circulation (ROSC). Hence, the exclusion criteria were (a) the time of CPR was more than 30 min due to cardiac arrest before admission, (b) CS caused by mechanical complications after AMI, (c) CS caused by VT storm, (d) age 90 years, and (e) shock being attributed to other causes, such as septic shock and hemorrhagic shock.
2.2 Baseline Data Collection
Demographic characteristics such as body mass index (BMI), blood pressure, heart rate, and respiration status were obtained from nursing records at admission. Medical history (history of hypertension, diabetes, stroke, dyslipidemia, coronary artery disease, peripheral artery disease, and chronic kidney disease), mechanically supported therapies (including circulatory and mechanical respiratory data), and type of AMI were obtained from hospital records. Laboratory parameters were routinely measured after each patient’s admission, and baseline biochemical tests and blood gas results were collected. Coronary artery lesions and intervention information were obtained from in-hospital coronary angiography images and reports. At admission, the left ventricular ejection fraction (LVEF) was evaluated by echocardiography. The Global Registry of Acute Coronary Event (GRACE) and Intra-aortic Balloon Pump in Cardiogenic Shock (IABP-SHOCK) II scores were calculated according to the baseline data of the patients at admission [4, 10]. The GRACE scores of the patients were calculated using the following variables: age, systolic blood pressure, heart rate, serum creatinine level, ST-segment deviation of the electrocardiogram, and cardiac arrest at admission [10]. The IABP-SHOCK Ⅱ scores were calculated by variables such as age, arterial lactate, serum glucose, creatine, history of stroke, and a thrombolysis in myocardial infarction (TIMI) flow grade reaching three after PCI [4].
2.3 Study Endpoints/Outcomes
The primary endpoint was death from any cause within 30 days and 1 year. Moreover, we followed the brain injury of patients with CA, while the severity of hypoxic brain damage was evaluated using cerebral performance categories (CPC) [15]. Follow-up information was obtained through telephonic interviews, medical charts, and outpatient visits. Hospital records were used to corroborate all data.
2.4 Statistical Analysis
The Kolmogorov–Smirnov test was used to assess data distribution. Continuous variables are presented as the mean or median with each range, and we used independent t-tests or the Kruskal–Wallis test to compare variables between groups. Qualitative variables are presented as frequencies and corresponding percentages, and chi-squared or Fisher’s exact tests were used to compare variables between groups. Associations between the clinical variables and endpoints were first assessed using univariate Cox regression analysis. Variables significantly associated with 30-day and 1-year mortality in univariate testing (*p * 0.10) were further examined using multivariate analysis. Survival rates were presented as Kaplan–Meier plots, and differences between groups were tested using the log-rank test. To investigate the additional predictive value of CA, concordance (C) indices were calculated from the time-to-event data proposed by Harrell et al. [16]. Statistical significance was defined as a two-sided p-value 0.05.
Since the mortality rate of AMI-CS was about 40% [1], prior estimates of power were conducted assuming a hazard ratio (HR) of 1.3 for CA; this power analysis showed that a sample size of 247 participants would result in a power of 0.88 ( = 0.05). All analyses were performed using Stata/MP 17.0 (StataCorp LLC, College Station, TX, USA) and R package 4.1.0 (Microsoft, Redmond, WA, USA).
3. Results
3.1 Baseline Clinical Characteristics between AMI-CS Patients with
and without CA
Table 1 summarizes the baseline and clinical characteristics of both the CA and non-CA groups within the cohort of 247 patients experiencing AMI-CS. Among these patients, 39 (15.8%) experienced CA. Most of the cohort was male (74.5%), with no significant difference in sex distribution between the CA and non-CA groups. The average age of all patients was 68 years, with the CA group showing a slightly younger profile (66 13 years vs. 69 13 years) compared to the non-CA group. CA patients exhibited lower mean systolic blood pressure (87 mmHg vs. 92 mmHg, p = 0.044) and mean arterial pressure (65.6 mmHg vs. 71.7 mmHg, p = 0.002). Additionally, the heart rate was higher in the CA group (100 beats per minute) compared to the non-CA group (96 bpm). Comorbidities, such as hypertension, diabetes mellitus, coronary artery disease (CAD), stroke, peripheral artery disease (PAD), and chronic kidney disease (CKD), were more prevalent in the non-CA group. Baseline lactate (6.9 mmol/L vs. 4.3 mmol/L), glucose (13.34 mmol/L vs. 11.82 mmol/L), and serum creatinine (177.5 µmol/L vs. 144.7 µmol/L) were higher in the CA group. Regarding AMI characteristics, 70.9% of total patients had ST-segment elevation myocardial infarction (STEMI), with 45.3% having anterior STEMI. Patients with CA showed a higher incidence of anterior STEMI (64.1%). Mechanical ventilation was utilized in 75.3% of total patients, with a higher proportion in the CA group (92.3% vs. 72.1%). Mechanical circulatory support was implanted in 42.1% of patients, with a higher proportion in the CA group (59.0% vs. 38.9%). Coronary angiography and revascularization rates were 89.4% and 80.2%, respectively. Additionally, 74.9% of patients had bi- or multivessel lesions, and 83.3% achieved a TIMI flow grade of 3 after PCI. Patients in the non-CA group were more likely to present with multivessel disease (38.2% vs. 48.7%). The GRACE score in the CA group was significantly higher than in the non-CA group (215 vs. 189, p = 0.000). According to the IABP-SHOCK II score risk categories, 25.7% and 10.3% of patients were classified as high-risk in the CA and non-CA groups, respectively.
Table 1.: Baseline and clinical characteristics of the AMI-related CS patients.
3.2 The Outcomes between AMI-CS Patients with and without CA
Within the AMI-CS cohort, 101 patients succumbed within 30 days and 116 patients within 1 year, resulting in 30-day and 1-year mortality rates of 40.9% and 47.0%, respectively. In both timeframes, the majority of deaths were attributed to cardiac causes, encompassing sudden cardiac death, ventricular tachycardia or fibrillation, refractory heart failure, or cardiogenic shock, with 93.1% at 30 days and 91.4% at 1 year (Table 2). Survival analysis, as depicted in Fig. 1, did not reveal a significant difference between the groups with and without CA. The overall rate of hypoxic brain damage during the hospital stay was 4.9%. Notably, the CA group exhibited a higher incidence of brain injury (25.6% vs. 1.0%), with 58.3% of these patients succumbing within 30 days and 75% within 1 year. For those surviving cardiac arrest with hypoxic brain injury, the extent of damage was generally mild, as indicated by CPC scores ranging from 1 to 3.
Kaplan–Meier plot of 30-day and 1-year mortality in AMI-related CS patients with and without CA. Abbreviations: AMI, acute myocardial infarction; CS, cardiogenic shock; CA, cardiac arrest.
3.3 Risk Factors for Short- and Long-Term Mortality Caused by AMI in
CS Patients
In the univariate Cox regression analysis, CA did not exhibit a significant association with either short- or long-term mortality, with hazard ratios (HRs) of 1.48 (p = 0.108) and 1.43 (p = 0.127), respectively (Tables 3,4). After adjustment by multivariate analysis, CA continued to lack a significant association with both short- and long-term mortality (HR = 0.88, p = 0.669; HR = 1.04, p = 0.881, respectively; Tables 3,4 and Supplementary Table 1). Exploring the univariate analysis, older age, female gender, higher heart rate, lower SBP and MAP, elevated baseline creatinine, arterial lactate, and glucose levels, presence of hypertension and CKD, TIMI flow grade 3 after PCI, higher GRACE score and IABP-SHOCK II score, lower LVEF, mechanical ventilation, and intra-aortic balloon pump (IABP) implantation were identified as factors associated with increased short- and long-term death (Tables 3,4). Further multivariate analysis revealed that older age, mechanical ventilation, arterial hypertension, higher baseline creatinine and arterial lactate levels, and a TIMI flow grade of 3 after PCI were significant risk factors for both 30-day and 1-year mortality (Tables 3,4).
Table 3.: Univariable and multivariable analyses of 30-day mortality for AMI-related CS patients.
Table 4.: Univariable and multivariable analyses of 1-year mortality for AMI-related CS patients.
3.4 Predictive Value of CA in Risk Models for Short- and Long-Term
Mortality
In the context of C-statistics, the GRACE score exhibited a moderate predictive value for both 30-day and 1-year mortality, with an area under the curve (AUC) of 0.69 [95% confidence interval (CI): 0.64 to 0.75, p = 0.000] and 0.67 (95% CI: 0.62 to 0.72, p = 0.000), respectively. Conversely, the IABP-SHOCK Ⅱ score demonstrated a high predictive value for both short- and long-term mortality, recording AUC values of 0.79 (95% CI: 0.74 to 0.84, p = 0.000) and 0.76 (95% CI: 0.71 to 0.81, p = 0.000), respectively. Comparatively, the GRACE score exhibited lower predictive performance than the IABP-SHOCK II score in forecasting short- and long-term mortality among AMI-related CS patients (p = 0.003). Additionally, incorporating CA into the IABP-SHOCK II score did not improve the predictive power for either short- or long-term mortality (p = 0.863 and 0.888, respectively; Table 5).
Table 5.: Models for predicting 30-day and 1-year mortality in C-statistics for AMI-related CS patients.
4. Discussion
The primary finding of this study was that CA did not emerge as an independent risk factor for either short- or long-term mortality in AMI-CS patients. Despite this, it is noteworthy that CA showed a significant association with the occurrence of brain injury in this patient population. While CA is acknowledged as a crucial element in the GRACE scoring system, our results indicate that the GRACE risk score provides only a moderate predictive value for individuals with AMI-CS. Furthermore, including CA as a risk factor in the IABP-SHOCK II scoring system did not improve its predictive accuracy for either the short- or long-term mortality assessment among AMI-CS patients. This suggests that the predictive value of CA within established risk models may not be as impactful as initially anticipated in shaping the prognosis of individuals with AMI-CS.
Cardiogenic shock after AMI poses a significant threat to life, with an overall 30-day mortality rate of approximately 40–50% [17]. Our study aligns with existing literature, revealing a comparable 30-day mortality rate of 40.7% in patients with AMI-CS. Historically, CA has been identified as a substantial risk factor for mortality in patients with ACS [3, 4, 5, 6]. While the GRACE score, a widely utilized tool for assessing death risk in ACS patients, includes CA as an important predictive factor [18], limited data exists on the correlation between CA and mortality, specifically in AMI-CS patients [11]. Current risk prediction models for CS, such as the IABP-SHOCK Ⅱ score, CARD-SHOCK risk score, SAVE, and ENCOURAGE score, notably omit CA as a risk factor [17]. Our study underscores that CA is not a significant prognostic factor for short- and long-term mortality in AMI-CS patients. Instead, age, lactate level, creatinine level, a TIMI grade 3 after PCI, and ventilation were identified as risk factors for mortality, consistent with previous research [4, 19, 20, 21]. Notably, the GRACE score exhibited moderate predictive performance for mortality in AMI-CS patients, although the addition of CA did not enhance the predictive value of the IABP-SHOCK II score. These observations align with prior studies [2, 3, 5], suggesting that CA may not influence the 7-day, in-hospital, and long-term mortality of AMI-CS patients [2, 3, 5]. The age and comorbidity profile of CA survivors and the simplicity of coronary lesions were proposed to explain these outcomes [4, 19, 20, 21, 22, 23]. Our study also highlighted that effective resuscitation, improved post-resuscitation care, and lower rates of hypoxic brain damage might contribute to the observed low proportion of non-cardiac deaths in the CA group [4, 15, 24]. Contrary to previous reports where hypoxic brain damage and cardiac failure were leading causes of in-hospital death in AMI-CS patients with CA [25], our population predominantly succumbed to cardiac causes. This discrepancy may stem from the impact of effective resuscitation on influencing outcomes, consistent with prior research [26].
This study holds significant clinical implications on multiple fronts. Firstly, it contributes valuable data to the ongoing exploration of whether CA is a prognostic factor for mortality in patients with AMI-CS. This finding emphasizes the importance of proactive rescue efforts for such patients, urging the public to engage in life-saving interventions actively. In China, where awareness regarding cardiac arrest and CPR remains limited [27, 28], our study underscores the critical need for heightened public education on CA and CPR. Importantly, our results suggest that surviving CA does not independently jeopardize the prognosis of AMI-CS patients. Thus, advocating for effective CPR becomes even more imperative, particularly in regions where a substantial number of patients grapple with AMI and cardiogenic shock. Secondly, our study poses a challenge to the GRACE score in predicting outcomes in AMI-CS patients, revealing its limited predictive capability. This observation prompts a reassessment of the GRACE score’s applicability, suggesting that it may not be universally suitable for all patients with ACS. This insight calls for a critical examination of existing risk assessment tools and the potential development of more tailored predictive models for specific subsets of ACS patients, particularly those confronting the complexities of AMI-CS.
While providing valuable insights, this study has limitations. Firstly, the observed rate of CA in our study was 15.8%, lower than previously reported rates [2, 3, 4, 5, 29]. This discrepancy might be attributed to excluding patients who did not survive until hospital admission, potentially leading to an underestimation of the true incidence of CA. The exclusion criteria, particularly limiting CPR time to 30 minutes, aimed to ensure a focus on genuine cases of AMI-CS. Secondly, despite not reaching statistical significance, the 30-day and 1-year mortality rates appeared higher in the CA group (53.9% vs. 38.5% and 59% vs. 44.7%, respectively). While not statistically conclusive, these findings may still bear clinical significance. Previous studies noted comparable outcomes, with one reporting a 62.7% mortality rate at 7 days for the cardiogenic shock population with CA, surpassing that of the non-CA group [3]. Another study, encompassing 1573 patients, identified a relatively higher short-term mortality risk in the CA group, though long-term mortality risk did not reach statistical significance (HR = 1.19, p = 0.055) [30]. Indeed, it is essential to acknowledge these trends, even without statistical significance. Thirdly, our study is limited by its retrospective, single-center design, which may limit the generalizability of findings to the broader Chinese population. However, the study population adhered to the criteria established by large prospective randomized controlled trials of AMI-CS [26, 29], and patients spanned various SCAI stages. Fourthly, the lack of exact timing and detailed information on the cardiac arrest events constitutes another limitation. Nevertheless, the meticulous selection of comprehensive clinical data and a robust sample size, pre-determined through careful sample size estimation, mitigate the likelihood of results occurring by chance. Despite these limitations, the study’s findings contribute valuable insights into the complex interplay of cardiac arrest and mortality in the context of AMI-CS.
5. Conclusions
In the context of AMI-CS in China, cardiac arrest has emerged as a non-contributory factor in predicting both short- and long-term mortality. Contrary to its significant impact on other cardiac conditions, CA does not independently pose an elevated risk in AMI-CS patients. This finding underscores the importance of active CPR efforts for patients facing AMI-CS, as survival from CA does not inherently compromise their overall prognosis. These results advocate for a proactive and vigorous approach to CPR in this specific patient cohort, emphasizing the need for continued efforts to enhance public awareness and responses to cardiac emergencies in the Chinese population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1van Diepen S Katz JN Albert NM Henry TD Jacobs AK Kapur NK et al Contemporary Management of Cardiogenic Shock: A Scientific Statement from the American Heart Association Circulation 2017136 e 232e 2682892398810.1161/CIR.0000000000000525 · doi ↗ · pubmed ↗
- 2Lauridsen MD Josiassen J Schmidt M Butt JH Østergaard L Schou M et al Prognosis of myocardial infarction-related cardiogenic shock according to preadmission out-of-hospital cardiac arrest Resuscitation 20211621351423366252210.1016/j.resuscitation.2021.02.034 · doi ↗ · pubmed ↗
- 3Ostenfeld S Lindholm MG Kjaergaard J Bro-Jeppesen J Møller JE Wanscher M et al Prognostic implication of out-of-hospital cardiac arrest in patients with cardiogenic shock and acute myocardial infarction Resuscitation 20158757622547524910.1016/j.resuscitation.2014.11.010 · doi ↗ · pubmed ↗
- 4Pöss J Köster J Fuernau G Eitel I de Waha S Ouarrak T et al Risk Stratification for Patients in Cardiogenic Shock After Acute Myocardial Infarction Journal of the American College of Cardiology 201769191319202840802010.1016/j.jacc.2017.02.027 · doi ↗ · pubmed ↗
- 5Vallabhajosyula S Payne SR Jentzer JC Sangaralingham LR Yao X Kashani K et al Long-Term Outcomes of Acute Myocardial Infarction with Concomitant Cardiogenic Shock and Cardiac Arrest The American Journal of Cardiology 202013315223281165010.1016/j.amjcard.2020.07.044 · doi ↗ · pubmed ↗
- 6Tyler J Henry J Garberich R Sharkey S Larson D Traverse J et al The impact of cardiac arrest and cardiogenic shock on out- comes in st-elevation myocardial infarction Journal of the American College of Cardiology 201973167
- 7Li Q Goodman SG Yan RT Gore JM Polasek P Lai K et al Pre-hospital cardiac arrest in acute coronary syndromes: insights from the global registry of acute coronary events and the canadian registry of acute coronary events Cardiology 201312627342386021310.1159/000353365 · doi ↗ · pubmed ↗
- 8Granger CB Goldberg RJ Dabbous O Pieper KS Eagle KA Cannon CP et al Predictors of hospital mortality in the global registry of acute coronary events Archives of Internal Medicine 2003163234523531458125510.1001/archinte.163.19.2345 · doi ↗ · pubmed ↗