The Effect of Hypertonic Saline Nebulization on Arterial Blood Gas Parameters Among Patients on a Mechanical Ventilator
Saraswathi M, Priyadharsini Masilamani, Kanniammal Chinnathambi

TL;DR
This study shows that using hypertonic saline nebulization helps improve blood oxygen and carbon dioxide levels in patients on ventilators.
Contribution
The study demonstrates statistically significant improvements in arterial blood gas parameters after hypertonic saline nebulization in ventilated patients.
Findings
Nebulization with hypertonic saline significantly improved PCo2, pO2, and HCo3 levels.
Arterial blood gas pH showed significant improvement at the 5% significance level.
The results suggest hypertonic saline nebulization is effective in enhancing respiratory parameters in ventilated patients.
Abstract
Introduction Care of the airway is an essential part of the management of patients receiving mechanical ventilation. If the airway is not properly managed, an endotracheal airway can result in retained secretions, airway obstructions, and infections. These complications may prolong mechanical ventilation duration and length of hospital stay and may increase the cost of affordability. Hypertonic saline nebulized suctioning is a technique used to lessen the duration of mechanical air flow and enhance airway clearance, which helps patients on mechanical ventilation breathe easier. Aim The objective of the study is to assess the effectiveness of nebulization with hypertonic saline on arterial blood gas parameters among mechanically ventilated patients. Methods The quasi-experimental design adopted with thirty-five mechanically ventilated samples was chosen using a non-probability…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
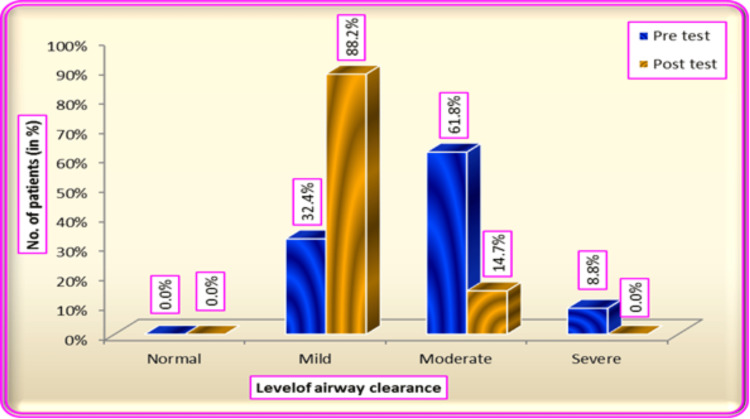 Figure 1
Figure 1| Clinical variables | Hypertonic saline | ||
| No | Percentage (%) | ||
| Reason for mechanical ventilation | CNS disorder | 14 | 40 |
| Lung disorder | 9 | 25.7 | |
| Cardiac disorder | 2 | 5.7 | |
| Renal Disorder | 3 | 8.6 | |
| Metabolic disorder | 7 | 20 | |
| Frequency of suctioning | Every 2 hours once | 21 | 60 |
| Every 4 hours once | 14 | 40 | |
| Every 6 hours once | 0 | 0 | |
| Duration of mechanical ventilation | One week | 19 | 54.3 |
| One month | 12 | 34.3 | |
| More than one month | 4 | 11.4 | |
| Patient position during suctioning | Supine position | 10 | 28.6 |
| Semi-Fowler's position | 25 | 71.4 | |
| Frequency of nebulization | Once a day | 0 | 0 |
| Two times a day | 35 | 100 | |
| Three times a day | 0 | 0 | |
| Four times a day | 0 | 0 | |
| Type of mucus secretion | Thick secretion | 10 | 28.6 |
| Thin secretion | 21 | 60 | |
| Clear secretion | 4 | 11.4 | |
| Bio Physiological variable | Test | N | Mean | SD | T value | Df | P value |
| ABG pH | Pretest | 35 | 7.35 | 0.05 | -2.148 | 34 | 0.039* |
| Posttest | 35 | 7.37 | 0.039 | ||||
| pCo2 | Pretest | 35 | 46.17 | 4.662 | 2.824 | 34 | 0.008** |
| Posttest | 35 | 42.91 | 4.804 | ||||
| pO2 | Pretest | 35 | 81.26 | 14.539 | -4.499 | 34 | >0.001** |
| Posttest | 35 | 93.49 | 14.251 | ||||
| HCo3 | Pretest | 35 | 26.49 | 4.21 | 2.848 | 34 | 0.007** |
| Posttest | 35 | 24.17 | 3.959 |
| Biophysiological variable | N | Mean | SD | T value | Df | p-value |
| Heart rate | 35 | 91.26 | 14.082 | 1.816 | 68 | 0.074 |
| SPO2 | 35 | 96.03 | 3.944 | -4.107 | 68 | >0.001** |
| ETCO2 | 35 | 35.94 | 6.301 | -0.173 | 68 | 0.863 |
| ABG pH | 35 | 7.37 | 0.039 | -2.485 | 68 | 0.015* |
| pCo2 | 35 | 42.91 | 4.804 | 1.999 | 68 | 0.049* |
| pO2 | 35 | 93.49 | 14.251 | -2.618 | 68 | 0.011* |
| HCo3 | 35 | 24.17 | 3.959 | 2.232 | 68 | 0.029* |
| Level of airway clearance | Hypertonic saline nebulization | |||
| Pre-test | % | Post-test | % | |
| Normal | 0 | 0 | 0 | 0 |
| Mild | 11 | 32.4 | 30 | 88.2 |
| Moderate | 21 | 61.8 | 5 | 14.7 |
| Severe | 3 | 8.8 | 0 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory Support and Mechanisms · Nosocomial Infections in ICU · Renal function and acid-base balance
Introduction
Care of the airway is an essential part of the management of patients receiving mechanical ventilation [1]. These complications may prolong mechanical ventilation duration and length of hospital stay and may increase the cost of affordability. Studies have been done over the years to improve airway management strategies [2]. Many of the studies emphasize the importance of airway management strategies and their impact on ventilator-associated events [3]. Mechanical ventilation is the commonly used intervention in intensive care units, such as airway management for patients [4].
A ventilator is a respiratory device that helps patients when they are unable to breathe by themself. An endotracheal tube is used as a port to connect the patient to the ventilator [5]. According to the NCBI Report of 2020, among 165 critically ill patients, 35.7% (59/165) of patients required mechanical ventilators [6]. Airway obstruction is common in mechanically ventilated patients due to various problems such as expiratory muscle weakness, mucociliary dysfunction, and unproductive cough. These causes may lead to endotracheal tube blockage that may be firm due to prescribed fluid therapy. The main goal of ICU is to minimize the duration of mechanical ventilation, as prolonged mechanical ventilation was proven to be associated with an increase in mortality and morbidity [7]. The goal of ICU is to reduce the duration of mechanical ventilation, as prolonged mechanical ventilation was proven to be associated with an increase in mortality and morbidity [8].
According to a study conducted by Haruna et al., 2022 among 400 samples, re-intubation is required for 51 (12.8%) [9]. If the airway is not properly managed, an endotracheal airway can result in retained secretions, airway obstructions, and infections. The most common reason for re-intubation was found to be difficulty in the excretion of secretions. Airway blockage will lead to poor oxygen perfusion in the body. Three essential steps of airway remodeling are humidification, nebulization, and suctioning. Airway clearance techniques will improve mucociliary function and improve the removal of secretions, inflammatory cells, and microorganisms [10]. Saline nebulization is a commonly used procedure to loosen the secretions and remove them easily from the endotracheal tube in intensive care units. Hypertonic saline nebulized suctioning has also proven to be effective in clearing airway secretions; however, it is not under regular use [10]. Generally, prescribed drugs for nebulization will be used to loosen the secretions [11]. Suctioning followed by nebulization with sodium-concentrated saline was demonstrated as an effective treatment to activate the mucociliary function, reduce the thickness of sputum, and reduce the swelling of the airway. It also prevents dryness in the airway. Care of the airway is an essential part of the management of patients receiving mechanical ventilation [12]. Airway blockage is directly proportional to gas exchange and acid-base imbalances. The worldwide incidence of people who require intensive care unit admission and mechanical ventilation is up to 20 million annually. Globally, according to Lance et al. (2015), the rate of seriously ill patients increased, and this study showed that around 4312 patients were admitted to three hundred ICUs within thirty-five nations, and among them, nearly 55% of patients were mechanically ventilated patients during intensive care unit admission.
Chakor et al. (2015) found that among the 1150 intensive care admissions, 3.91% of patients required prolonged ventilator support [13]. Also among 397 clients, 11.3% needed invasive ventilation. Weaning from mechanical ventilation is an essential element of caring for critically ill patients. So, the main focus of the health care provider is to wean the patient from a mechanical ventilator. Maintaining a patent airway has a major role in weaning the patient from the ventilator.
According to a study conducted by Sudarsanam et al., of the 200 mechanically ventilated patients, at discharge 143 patients (71.5%) had died due to various reasons such as respiratory failure, endotracheal tube obstruction, and so on [14]. In the present study, the investigator finds the effect of hypertonic saline nebulization on arterial blood gas parameters among mechanically ventilated patients.
Materials and methods
The research adopted a quantitative evaluative approach with one group pre-test post-test design. In this study, the independent variable was nebulization with hypertonic saline, and the dependent variable was biophysiological measures and the level of airway clearance. The study was conducted in the ICU complex of Sri Ramaswamy Memorial (SRM) General Hospital, with a sample size of 35. The study included patients who were mechanically ventilated with age above 21 years. Patients who were admitted to the intensive care unit, patients' relatives who signed the informed consent, and patients who were discharged within three days were excluded from this study. Biophysiological measures of pre- and post-test values were collected using arterial blood gas (ABG) parameters (ABG-pH, ABG-pCo2, ABG-po2, ABG-HCo3). The validity obtained from experts in medicine and nursing from SRM General Hospital and Research Institute and SRM College of Nursing provided feedback on the tool's validity. The tool's suitability, relevance, and accuracy were confirmed through validation, and the Institutional Ethical Committee granted formal ethical approval. Data was collected from 35 mechanically ventilated patients chosen using a non-probability purposive sampling technique. Pre-test was done, and as an intervention, endotracheal tube nebulization was given for 15-20 minutes with 2 ml of hypertonic saline two times daily for three days. Followed by endotracheal suctioning performed approximately 5-10 seconds. Post-test was carried out about 15-20 minutes after the procedure by using arterial blood gas analysis.
Results
This study concluded, with a total of 35 mechanical ventilator patients admitted to the ICU. Table 1 reveals that the p-values corresponding to the bio-physiological variables SPO2, PCo2, pO2, and HCo3 are less than 0.01 and are significant at 1% level hence there is a high significant difference between the pretest and post-test mean scores of bio-physiological variables SPO2, PCo2, pO2, and HCo3 also the p-value corresponding to the bio-physiological variable ABG pH is less than 0.05 and is significant at 5% level and hence there is a significant difference between the pretest and post-test mean scores of bio-physiological variable ABG pH.
Table 2 explains the p-value corresponding to the bio-physiological variable SPO2 is less than 0.01 and is significant at 1% level hence there is a high significant difference between the post-test level mean scores of bio-physiological variable SPO2. Also, the p+values corresponding to the bio-physiological variables ABG pH, pCo2, pO2, and HCo3 are less than 0.05 and are significant at 5% level, hence, there is a significant difference between the post-test level mean scores of bio-physiological variables ABG pH, pCo2, pO2 and HCo3 of hypertonic saline nebulization.
Table 3 shows in the pre-test 21 (61.8%) patients had moderate levels of airway clearance, 11 (32.4%) had mild levels of airway clearance and three (8.8%) had a severe level of airway clearance whereas the level of airway clearance improved in post-test as 30 (88.2%) had mild level of airway clearance and five (14.7%) had a moderate level of airway clearance after hypertonic saline nebulization. The study findings also show the frequency and percentage distribution of pre-test and post-test biophysiological variables, pre-test values related to heart rate 19 (54.3%) had 100-115, 13 (37.1%) had above 115 or below 70, three (8.6%) had 70-99, whereas in post-test, 22 (62.9%) had 70-99, 12 (34.3%) participants had 100-115 and one (2.9%) had above 115 or below 70. Related to SpO2 in the pre-test, 15 (42.9%) had 99%-85%, 13 (37.1%) had 100%-95% and seven (20%) had below 85%, whereas in the post-test, 25 (71.4%) had 100%-95%, 10 (28.6%) had 94%-85%. Regarding ETCO2 in the pre-test, 17 (48.6%) had 46-50, 14 (40%) had 35-45, and four (11.4%) had above 50, whereas in the post-test, 23 (65.7%) had 35-45, and 12 (34.3%) had 46-50. Related to ABG pH 16(45.7%) belonged to 7.30-7.34, 13 (37.1%) belonged to 7.35-7.46, and six (17.1%) were above 7.46 or below 7.30, whereas in the post-test, 24 (68.6%) had a pH of 7.35-7.46, 11 (31.4%) had 7.30-7.34. Related to pCo2 in the pre-test, 18 (51.4%) had 25-34, 12 (34.3%) had 35-46 and five (14.3%) had below 25 or above 46, whereas in the post-test, 24 (68.6%) had 35-46, nine (25.7%) had 34-25, and two (5.7%) had below 25 or above 46. Po2 in the pre-test, 15 (42.9%) had 70-89, 10 (28.6%) each in above 90 and below 70, whereas in the post-test, 21 (60%) had above 90, 12 (34.3%) had 70-89, and two (5.7%) had below 70. Related to HCO3 in the pre-test, 16 (45.7%) had 27-35, 13(37.1%) had 17-26 and 6(17.1%) had above 35 or below 17, whereas in the post-test, 23 (65.7%) had 17-26 and 12 (34.3%) had 27-35. Table 4 shows the distribution of the level of airway clearance of mechanically ventilated patients, and Figure 1 shows results that hypertonic saline was effective in airway clearance at a p-value of 0.000.
Results showing that hypertonic saline was effective in airway clearance at a p-value of 0.000Percentage distribution of the level of airway clearance of mechanically ventilated patients among the hypertonic saline group
Discussion
In the endotracheal tube, nebulization was given with 2 ml of hypertonic saline over 15-20 mins, two times each day for three days. Followed by endotracheal suctioning performed approximately 5-10 seconds for the patients. The patients who were discharged within three days were excluded from this study. The post-test was carried out about 15-20 minutes after the procedure. Biophysiological measurements were obtained from a continuous cardiac monitor, and arterial blood gas analysis reports were obtained. The level of airway clearance was recorded before and after the administration of hypertonic saline nebulized suctioning. Hypertonic saline nebulization is cheap, safe, and effective in maintaining the airway patency of patients who are connected to an artificial airway. The major findings of the study were there is a highly significant difference between the pre-test and post-test mean scores of airway clearance at the p-value >0.001, and is significant at a 1% level. The mean value at the post-test level is less than the mean value at the pre-test level, and the study concludes that hypertonic saline is effective in airway clearance. The p-values corresponding to the biophysiological variables SPO2, PCo2, pO2, and HCo3 are less than 0.01 and are significant at a 1% level; hence, there is a high significant difference between the pre-test and post-test mean scores of bio-physiological variables SPO2, PCo2, pO2, and HCo3 of hypertonic saline nebulization.
Conclusions
The study concludes that the effectiveness of nebulization with hypertonic saline on biophysiological measures and the level of airway clearance among mechanically ventilated patients. The study also concludes that the nebulization with hypertonic saline for patients with mechanical ventilators is more effective in maintaining arterial blood gas parameter values like SPO2 and pO2, reducing pCO2, and maintaining pH at normal range, and also more effective on airway clearance. The nurse has the primary role in maintaining a patent airway for mechanically ventilated patients. So, it is important to improve their knowledge and practice related to airway clearance. This can be enabled by applying the research into the practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ventilator-associated pneumonia: issues related to the artificial airway Respir Care Diaz E Rodríguez AH Rello J 900906502005 https://pubmed.ncbi.nlm.nih.gov/15972111/15972111 · pubmed ↗
- 2Ventilator-associated pneumonia and suction: a review of the literature Br J Nurs Letchford E Bench S 1318272018 https://pubmed.ncbi.nlm.nih.gov/29323990/2932399010.12968/bjon.2018.27.1.13 · doi ↗ · pubmed ↗
- 3Airway devices in ventilator-associated pneumonia pathogenesis and prevention Clin Chest Med RouzéA Martin-Loeches I Nseir S 7757833920183039074810.1016/j.ccm.2018.08.001 · doi ↗ · pubmed ↗
- 4Fundamentals of Nursing Research Brockopp DY Hastings-Tolsma MT Jones and Bartlet Publication 1995 https://books.google.ee/books?hl=en&lr=&id=pvd P Es 86KVUC&oi=fnd&pg=PR 17&dq=Fundamentals+of+Nursing+Research&ots=Ax SUTK Mv LD&sig=2z 5H 5u RHV_a Ov 6e Wa-bfrc ZV 3n I&redir_esc=y#v=onepage&q=Fundamentals%20of%20Nursing%20Research&f=false
- 5ICU and ventilator mortality among critically ill adults with coronavirus disease 2019 Crit Care Med Auld SC Caridi-Scheible M Blum JM 080448202010.1097/CCM.0000000000004457 PMC 725539332452888 · doi ↗ · pubmed ↗
- 6Effect of nebulized 3% hypertonic saline in the treatment of viral bronchiolitis Pulmon Res Wood C 14915882008 https://www.google.com/url?sa=t&source=web&rct=j&opi=89978449&url=https://www.researchgate.net/publication/345482955_Effect_of_Nebulized_Suctioning_with_3_Hypertonic_Saline_for_Mechanically_Ventilated_Patient_on_Airway_Clearance&ved=2ah UK Ewjt 8p Cgv Iy H Ax W Hi 2MGHS Jt CC 4Q Fno ECBAQAQ&usg=A Ov Vaw 19YCNAIRD 9Kx 9i Opl D 5O 5m
- 7Saline instillation before tracheal suctioning decreases the incidence of ventilator-associated pneumonia Crit Care Med Caruso P Denari S Ruiz SA Demarzo SE Deheinzelin D 32383720091905060710.1097/CCM.0b 013e 3181930026 · doi ↗ · pubmed ↗
- 8Safety and efficacy of N-acetyl-cysteine for prophylaxis of ventilator-associated pneumonia: a randomized, double blind, placebo-controlled clinical trial Med Gas Res Sharafkhah M Abdolrazaghnejad A Zarinfar N Mohammadbeigi A Massoudifar A Abaszadeh S 1923820182977019210.4103/2045-9912.229599 PMC 5937299 · doi ↗ · pubmed ↗