A Curious Case of Pericardial Effusion Diagnosed as Diffuse Large B-cell Lymphoma
Madhulika L Mahashabde, Harin M Bhavsar, Yash R Bhimani

TL;DR
A 64-year-old man with chest pain and heart symptoms was diagnosed with diffuse large B-cell lymphoma after tests revealed a mediastinal mass and pericardial effusion.
Contribution
This case report highlights an unusual presentation of diffuse large B-cell lymphoma as pericardial effusion, emphasizing the need for prompt diagnosis.
Findings
A mediastinal mass and pericardial effusion were found in a patient with progressive heart symptoms.
CT-guided biopsy confirmed the diagnosis of diffuse large B-cell lymphoma.
DLBCL can present with non-specific symptoms requiring thorough evaluation for accurate diagnosis.
Abstract
Lymphoma arises from mature B, T, and natural killer (NK) cells. Lymphomas are classified into Hodgkin's lymphoma (HL) and non-Hodgkin's lymphoma (NHL). Diffuse large B-cell lymphoma (DLBCL) is a type of NHL. It can present with symptoms such as fever, chills, or night sweats, as well as symptoms due to extranodal involvement. Extranodal sites can include the gastrointestinal tract or renal involvement. A higher risk of developing diffuse large B-cell lymphoma (DLBCL) is seen in patients with congenital or acquired immunodeficiency, those on immunosuppression, and those with autoimmune disorders. In this case report, we present a case of pericardial effusion that, upon further evaluation, was diagnosed as diffuse large B-cell lymphoma (DLBCL). A 64-year-old male presented with complaints of retrosternal chest pain that progressed from New York Heart Association (NYHA) Grade II to IV…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
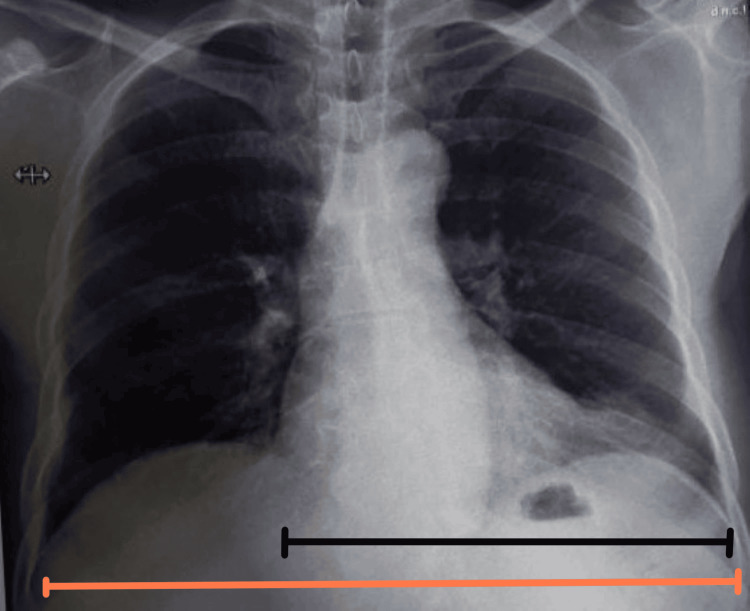 Figure 1
Figure 1 Figure 2
Figure 2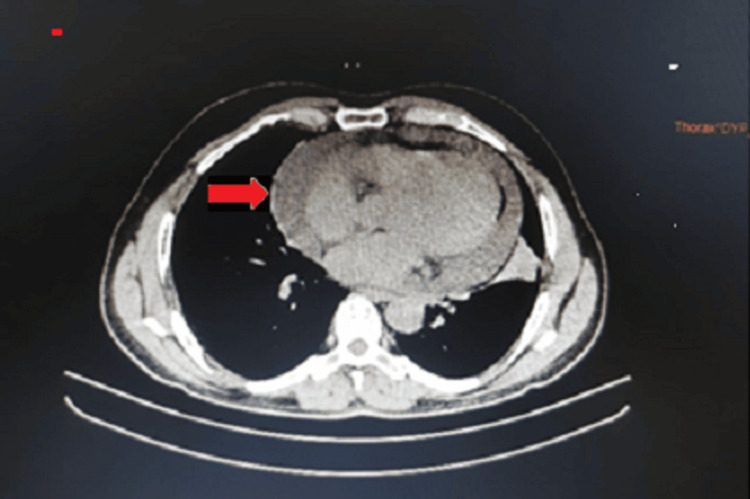 Figure 3
Figure 3 Figure 4
Figure 4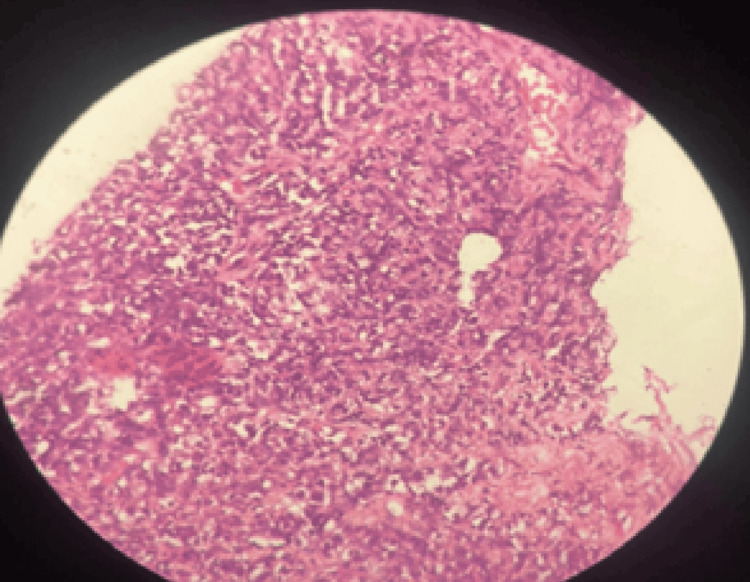 Figure 5
Figure 5| Laboratory investigation | Report | Reference range |
| Hemoglobin | 13 g/dL | 13.2-16.6 g/dL |
| Total leukocyte count | 7,000/µL | 4,000-10,000/µL |
| Platelet | 310,000/µL | 150,000-410,000/µL |
| Urea | 28 mg/dL | 17-49 mg/dL |
| Creatinine | 1.6 mg/dL | 0.6-1.35 mg/dL |
| Total bilirubin | 1.15 mg/dL | 0.2-1.2 mg/dL |
| Direct bilirubin | 0.48 mg/dL | 0.5 mg/dL |
| AST | 34 U/Lt | 8-48 U/Lt |
| ALT | 71 U/Lt | 7-55 U/Lt |
| ALP | 118 U/Lt | 40-129 U/Lt |
| Hba1c | 6.3% | <5.6% |
| Total protein | 7.10 g/dL | 5.5-8 g/dL |
| Serum albumin | 4.2 g/dL | 3.5–5 g/dL |
| A/G ratio | 1.45 | 1.1-2.5 |
| ESR | 44 mm/hour | <20 mm/hour |
| CRP | 15 mg/dL | <2 mg/dL |
| HIV | Negative | Negative |
| HBsAg | Negative | Negative |
| HCV | Negative | Negative |
| D-dimer | 598 µg/L | <500 µg/L |
| CBNAAT | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Cardiac tumors and thrombi · Pericarditis and Cardiac Tamponade
Introduction
Lymphoma is the malignancy of lymphocytes within the lymphoid system, arising from B, T, or natural killer (NK) cells. It encompasses two main categories: non-Hodgkin's lymphoma (NHL) and Hodgkin's lymphoma (HL), with approximately 80% of cases classified as non-Hodgkin's lymphoma. B cells are versatile and capable of differentiating into various pathways, contributing to a spectrum of disorders with diverse clinical and pathological characteristics [1]. There are around 30 recognized subtypes of non-Hodgkin's lymphoma (NHL), with diffuse large B-cell lymphoma (DLBCL) being the most prevalent, comprising about 30% of all NHL cases [2]. The risk factors for DLBCL include immunosuppression, autoimmune disorders, and congenital and acquired immunodeficiency. The symptoms of lymphoma can include swollen lymph nodes in the neck or groin, fatigue, chest pain, cough, dyspnea if chest swelling occurs, back pain from bone involvement, and unusual bleeding or bruising. B symptoms, such as night sweats, fever, and weight loss, are common.
Extranodal involvement occurs in approximately 50% of patients, most frequently affecting the gastrointestinal tract and skin. Tumor lysis syndrome or lymphadenopathy can lead to ureteral obstruction and secondary renal involvement. Aggressive NHL may present with extranodal manifestations, including airway compression and superior vena cava syndrome. The symptoms related to infiltrated organs may develop if extranodal disease extends beyond the lymphatic system. The common sites of extranodal involvement include the skin, bones, spinal cord, and testicles [3]. Cardiac involvement as an initial sign of lymphoma is exceedingly rare, with DLBCL most commonly affecting the right atrium [4]. Primary cardiac lymphoma is confined to the heart and pericardium, whereas mediastinal DLBCL invades the heart [5]. B-cell lymphomas can also be associated with paraneoplastic syndromes. Treatment typically involves rituximab-based chemotherapy regimens, such as rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP), or alternative combinations such as rituximab, polatuzumab vedotin, cyclophosphamide, doxorubicin, and prednisone (R-pola-CHP) [6,7].
Case presentation
A 64-year-old male, a farmer by occupation, came with complaints of precordial chest pain and breathlessness that progressed from New York Heart Association (NYHA) Grade II to IV over a month, along with orthopnea, paroxysmal nocturnal dyspnea, and widespread edema that had been present for 12 days. The patient had retrosternal chest pain that was moderate in intensity, dull aching, and non-radiating. There was no associated history of fever, cold, palpitation, or diaphoresis. There was no history of addiction, smoking, drinking, or tobacco use. Additionally, there were no comorbidities reported, and there was no family history of malignancy. On examination, the patient had tachycardia and raised jugular venous pressure with mild pallor. There was no icterus, cyanosis, clubbing, edema, lymphadenopathy, or distended veins. On systemic examination, crepitations were present in the bilateral infra-axillary region and infra-scapular region, heart sounds were muffled but no additional heart sounds, and no third or fourth heart sounds were present. The patient's laboratory investigations on the day of admission are shown in Table 1.
Chest X-ray (posteroanterior {PA} view) showed cardiomegaly with an increased cardiothoracic ratio, mediastinal widening, and pulmonary congestion (Figure 1). Echocardiography revealed moderate pericardial effusion, with Grade I diastolic dysfunction (Figure 2). Therefore, high-resolution computed tomography (HRCT) of the thorax was performed, revealing moderate to extensive pericardial effusion. A homogenously enhancing mass lesion was observed with an epicenter in the left anterior-superior mediastinum, encasing the arch of the aorta. It extended inferiorly into the middle mediastinum, encasing the ascending aorta, main pulmonary trunk, right superior pulmonary vein, and right pulmonary artery. The mass was also seen extending to the inferior basal aspect of the heart, wrapping around the atrioventricular and interventricular groove (Figure 3). Therefore, a computed tomography (CT)-guided biopsy of the mediastinal mass was performed for further evaluation, and the sample was sent for histological analysis (Figure 4). On histopathological examination, there were large cells with irregular nuclear margins and a few scattered small lymphoid cells. Some of the cells showed large pleomorphic nuclei and pale cytoplasm, suggestive of diffuse large B-cell lymphoma (DLBCL). Immunohistochemistry was positive for cluster of differentiation (CD) 20 in large cells and CD3-positive in background cells, with 80% positivity for Ki-67 (Figure 5).
Chest X-ray posteroanterior view showing increased cardiothoracic ratio suggestive of cardiomegalyThe cardiothoracic ratio is the ratio of the cardiac margin (black line) divided by the thoracic margin (orange line). A ratio of more than 0.5 in adults suggests cardiomegaly
In apical four-chamber view on 2D echocardiography, moderate pericardial effusion can be seen (red arrow)
High-resolution computed tomography (HRCT) of the thorax revealed moderate to gross pericardial effusion with homogenously enhancing mass lesion
Computed tomography (CT)-guided transsternal biopsy of mediastinal mass
Histopathological analysis showed large cells with irregular nuclear margins and few scattered small lymphoid cells, with some of the cells showing large pleomorphic nuclei and pale cytoplasm, suggestive of diffuse large B-cell lymphoma (DLBCL)
Discussion
DLBCL is the most common type of non-Hodgkin's lymphoma. DLBCL comprises one-third of all NHL cases. The risk factors for DLBCL include immunosuppression, autoimmune disorders, and congenital and acquired immunodeficiency [8]. Tumor cells typically express B-cell antigens (CD19, CD20, and CD79a) and monoclonal IgM. The rearrangements of B-cell lymphoma 6 (BCL6) occur in approximately 30% of DLBCLs. About 20%-30% of DLBCLs are associated with the t(14;18) translocation. B symptoms occur in 30% of patients, and serum lactate dehydrogenase (LDH) levels are elevated in over half of them. Extranodal disease is present in 40% of cases and may affect the gastrointestinal tract, testis, bone, thyroid, skin, central nervous system, and/or bone marrow. Typically, heart involvement occurs later in the course of DLBCL. Dissemination occurs through the direct extension of the tumor, hematogenous spread, or lymphatic spread. The direct extension of the tumor leads to pericardial disease. The major involvement of the epicardial-adventitial region is believed to be caused by retrograde lymphatic spread. Hematogenous spread is responsible for the widespread interstitial-perivascular pattern, which is not specific to the heart's endocardial or epicardial elements [9].
For diagnosis, a CT scan is used when a patient's images from other noninvasive techniques are insufficient when they are known to be contraindicated for cardiac magnetic resonance imaging (CMRI) [10]. Heart lymphoma typically presents as hypo-attenuating masses on CT. These masses extend along the epicardium surrounding the coronary arteries and infiltrate the myocardium. The diagnosis of cardiac lymphoma using 18F-fluorodeoxyglucose positron emission tomography (18F-FDG PET) alone presents difficulties as it has low resolution and the radiotracer physiologically accumulates more in the myocardium [11]. The patients with cardiac DLBCL have demonstrated good response rates to chemotherapy using R-CHOP. In one case series, the survival rate was 30 months, and the overall response rate of primary cardiac lymphoma to this treatment was 79% [6]. Alternatives include R-pola-CHP, which, compared to R-CHOP, showed a higher survival rate without progression at two years [7].
In addition to chemotherapy, surgical resection may be undertaken in the early stages of the disease [12,13]. Debulking surgery becomes necessary for patients presenting with hemodynamic impairment and superior vena cava syndrome. Surgery may serve as a palliative intervention in cases of severe right ventricular outflow obstruction to increase lung blood flow. Patients experiencing worsening illness even after chemotherapy may benefit from radiation therapy [14]. Prognosis in cardiac DLBCL varies based on the disease stage, extent of cardiac involvement, and response to treatments such as R-CHOP.
Conclusions
Diagnosing cardiac DLBCL typically requires multimodal imaging because the condition can present with subtle symptoms. Physicians should consider lymphoma in the differential diagnosis when evaluating a cardiac tumor. It is important to distinguish mediastinal DLBCL with cardiac involvement from primary cardiac lymphoma due to differences in prognosis. Given the aggressive nature of DLBCL and its rapid growth, successful treatment relies on early detection and conventional chemotherapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The histological classification of diffuse large B-cell lymphomas Semin Hematol Xie Y Pittaluga S Jaffe ES 57665220152580558510.1053/j.seminhematol.2015.01.006PMC 4374126 · doi ↗ · pubmed ↗
- 2Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001 Blood Morton LM Wang SS Devesa SS Hartge P Weisenburger DD Linet MS 26527610720061615094010.1182/blood-2005-06-2508 PMC 1895348 · doi ↗ · pubmed ↗
- 3Diffuse large B-cell lymphoma-review J Med Sci Singh R Dubey AP Rathore A Kapoor R Sharma D Singh NK Maggo S 137143382018
- 4Primary cardiac diffuse large B cell lymphoma presenting with superior vena cava syndrome Can J Cardiol Johri A Baetz T Isotalo PA Nolan RL Sanfilippo AJ Ropchan G 0225200910.1016/s 0828-282x(09)70110-2PMC 272249919536397 · doi ↗ · pubmed ↗
- 5A rare case of diffuse large B cell lymphoma presenting as a cardiac mass Am J Case Rep Yousif P Kotecha A Thakur A Ismail HM 182118252020193180949310.12659/AJCR.917159 PMC 6913268 · doi ↗ · pubmed ↗
- 6Differential diagnosis of cardiac tumors: general consideration and echocardiographic approach J Clin Ultrasound Pino PG Moreo A Lestuzzi C 117711935020223621820310.1002/jcu.23309 PMC 9828386 · doi ↗ · pubmed ↗
- 7Prognostic utility of differential tissue characterization of cardiac neoplasm and thrombus via late gadolinium enhancement cardiovascular magnetic resonance among patients with advanced systemic cancer J Cardiovasc Magn Reson Chan AT Plodkowski AJ Pun SC 761920172902542510.1186/s 12968-017-0390-2PMC 5639740 · doi ↗ · pubmed ↗
- 8Epidemiology and etiology of diffuse large B-cell lymphoma Semin Hematol Wang SS 2552666020233824277210.1053/j.seminhematol.2023.11.004PMC 10962251 · doi ↗ · pubmed ↗