Challenges in diagnosis and management of aortobronchial fistula: a case report
Mohamed Hamza Abaydi, Safae Dhimene, Amine Ech-chenbouli, Badre El Boussaadani, Zainab Raissuni

TL;DR
This case report discusses the challenges in diagnosing and managing a rare condition called aortobronchial fistula, emphasizing the importance of early detection and multidisciplinary care.
Contribution
The paper presents a rare case of aortobronchial fistula and highlights the diagnostic and therapeutic challenges associated with it.
Findings
Aortobronchial fistulas often present with haemoptysis and can be life-threatening if not treated.
Tranexamic acid showed clinical improvement but bleeding recurred after discontinuation.
Endovascular treatment is a viable option for managing contained ruptures in high-risk patients.
Abstract
Aortobronchial fistulas (ABFs) are rare but potentially life-threatening conditions, often presenting with haemoptysis. They can develop following various thoracic aortic conditions or procedures. A 70-year-old patient with a history of descending aorta replacement and ischaemic stroke presented with chest pain and upper gastrointestinal bleeding. Imaging revealed a fistula between the aortic prosthesis and the lung, along with other cardiovascular abnormalities. Despite the indication for anticoagulant therapy, tranexamic acid was initiated due to bleeding risk. The patient showed clinical improvement with tranexamic acid treatment but experienced recurrence of bleeding after discontinuation. Endovascular treatment for the contained rupture at the proximal stent anastomosis was indicated. Haemoptysis is the primary symptom of ABFs, often recurring until the fistula enlarges.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
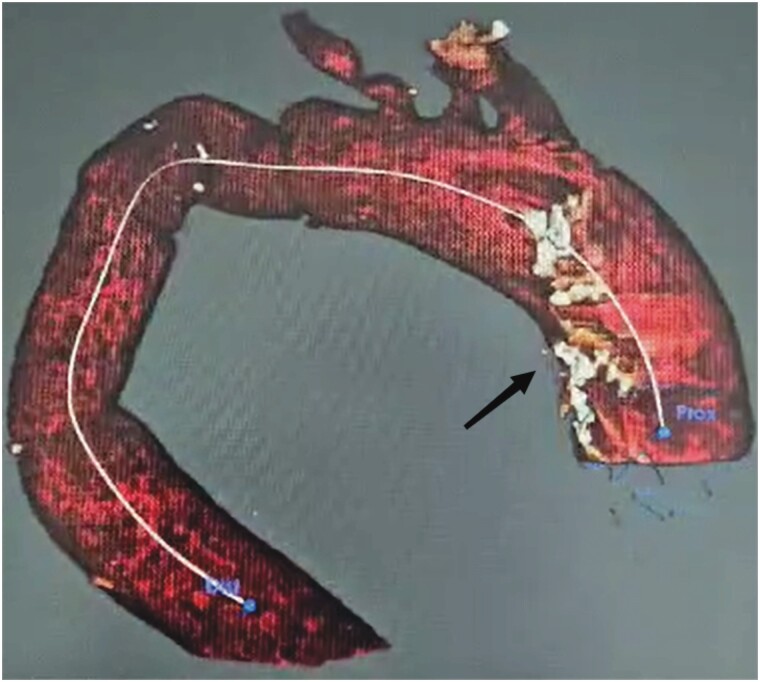 Figure 1
Figure 1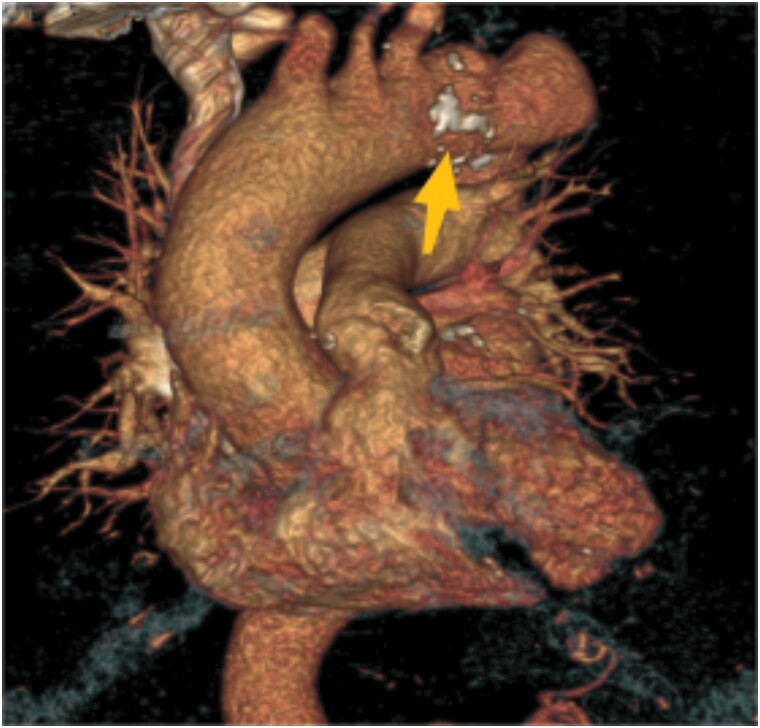 Figure 2
Figure 2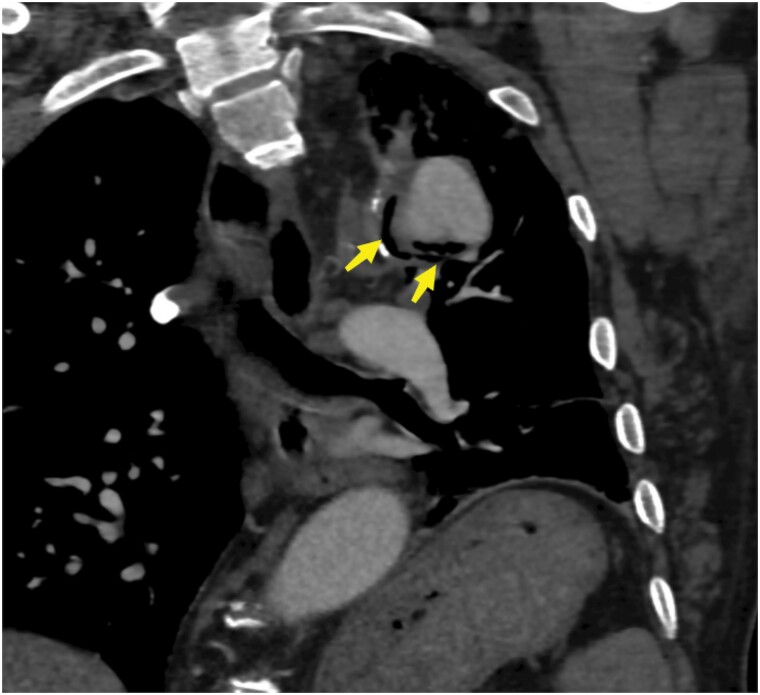 Figure 3
Figure 3 Figure 4
Figure 4| Date | Event |
|---|---|
| 1996 | TEVAR surgery: descending aorta replacement following aortic dissection. |
|
| Ischaemic stroke: 2 months prior to current admission. |
|
|
|
|
| Cardiac MRI revealed ischaemic heart disease with a left ventricular ejection fraction (LVEF) of 38% and a small thrombus lining the apex. Bronchoscopy showed a diffuse inflammatory appearance. |
|
| Endovascular treatment for the contained rupture at the proximal stent anastomosis was considered in multidisciplinary counselling, involving the surgeon who initially operated on him. |
|
| Decision to discontinue tranexamic acid due to stable condition. |
|
| Recurrence of bleeding, and tranexamic acid was reintroduced. |
|
| Patient awaiting preparation of the most appropriate endoprosthesis. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHungarian Social, Economic and Educational Studies
Introduction
Aortobronchial fistulas (ABFs) are rare and late complications of cardiac surgery that can be fatal if left untreated. They most often occur after procedures involving the descending thoracic aorta. Haemoptysis, which can be massive or intermittent, is the primary symptom. The interval between the initial surgery and the onset of haemoptysis ranges from 3 weeks to 25 years. Diagnostic examinations are often unable to directly visualize a fistula. Indication for surgical or endovascular repair typically relies on clinical suspicion and non-specific diagnostic features.^1,2^
This case of a 70-year-old patient with a history of descending aorta replacement underscores several critical aspects of healthcare delivery. It highlights the diagnostic challenges and the importance of multimodal imaging in identifying ABFs. Additionally, the management complexities, particularly balancing anticoagulation needs with bleeding risks, are evident. This case also emphasizes the necessity of a multidisciplinary approach and long-term follow-up to optimize patient outcomes and prevent recurrence.
Summary figure
**: **
Case presentation
A 70-year-old patient with a history of descending aorta replacement and ischaemic stroke presented to the emergency room with chest pain and 500 mL of haematemesis. He had undergone descending aorta replacement for an aortic dissection complicated by a thrombotic aneurysm 27 years prior and had experienced an ischaemic stroke 2 months before this presentation. Following the stroke, the patient was on antiplatelet therapy (Kardegic) and a statin.
One week before hospitalization, the patient underwent an oesophagogastroduodenal endoscopy due to a prior episode of haemorrhage, which did not reveal any source of bleeding or lesions.
Physical examination revealed atypical chest pain, Stage II dyspnoea according to the MRC (Medical Research Council) dyspnoea scale, and Broca’s aphasia. The patient was haemodynamically stable with a blood pressure of 110/70 mmHg and a heart rate of 76 b.p.m. Respiratory examination showed an SpO_2_ of 96% on room air. Neurologically, the patient was stable. He was admitted to the cardiac intensive care unit for close monitoring. The patient subsequently experienced a new episode of bleeding, which was identified as haemoptysis by a physician after careful examination.
Laboratory findings indicated normochromic normocytic anaemia, with a haemoglobin level of 9.8 g/dL (normal range, >12 g/dL). The electrocardiogram revealed a newly identified counterclockwise flutter, occurring with a ventricular rate of 76 b.p.m. Transthoracic ultrasound showed apical akinesia with a left ventricular ejection fraction (LVEF) of 40% and left atrial dilatation. However, femoral coronary angiography could not be performed due to the blockage of the guide at the level of the thoracic aorta.
Thoracic computed tomographic (CT) angiography identified a fistula between the prosthesis and the lung, accompanied by the presence of air and a suspected blood flow during the haemoptysis episode (Figures 1–4). Subsequent bronchoscopy showed a distorted appearance of the entire bronchial tree, with thickened walls and orifices narrowed by extrinsic compression, alongside a diffuse inflammatory appearance.
CT angiography with 3D reconstruction of the aorta showing a contained rupture at the proximal anastomosis of the graft.
CT angiography with 3D reconstruction of the aorta showing a contained rupture at the proximal anastomosis of the graft.
CT angiography in the mediastinal window shows a prosthetic fistula involving the lung.
CT angiography in the parenchymal window shows a prosthetic fistula involving the lung.
Cardiac MRI further revealed ischaemic heart disease with segmental kinetic disturbances in the anterior territory, deemed non-viable, an LVEF of 38%, and a small thrombus lining the apex.
Given the patient’s newly identified counterclockwise flutter and the presence of a small thrombus lining the apex, anticoagulant therapy was clearly indicated. However, due to the risk of bleeding, particularly with the episode of haemoptysis, the decision was made to initiate tranexamic acid therapy at a dosage of 500 mg, three times daily. This approach was chosen to mitigate bleeding risk while balancing the need for anticoagulation. The heart failure treatment administered included beta-blockers, spironolactone, angiotensin-converting enzyme (ACE) inhibitors, and SGLT2 inhibitors. Endovascular treatment for the contained rupture at the proximal stent anastomosis was considered during multidisciplinary counselling but was deemed non-urgent due to the patient’s clinical, haemodynamic, and haematologic improvement.
Follow-up
The patient was treated with tranexamic acid for 5 months while awaiting the preparation of the most suitable endoprosthesis. During this time, significant improvements were observed in both clinical evaluations and echocardiographic assessments. However, 1 month after discontinuing tranexamic acid, the patient experienced streaks of blood in the sputum, indicating a recurrence of bleeding. Tranexamic acid was reintroduced, leading to clinical improvement and the resolution of bleeding episodes.
Discussion
Haemoptysis is often the initial and sometimes the sole symptom of ABFs. The severity of haemoptysis can range from massive to intermittent, depending on the size of the fistula. Typically, the fistula is small and may be occluded by clots, remaining closed for weeks or months. Once the clots dissolve or dislodge, the fistula reopens, leading to recurrent bleeding. Over time, this process can escalate, causing more significant bleeding as the fistula enlarges. Other symptoms, such as dyspnoea, cough, and chest or back pain, are less common.^1^
Postoperative aortic fistulas, including aortobronchial and aortopulmonary fistulas, are uncommon and typically present as delayed complications after cardiothoracic surgery. According to a comprehensive review by Piceche et al., these fistulas are more prevalent following procedures for descending thoracic aortic aneurysms (dTAA) compared to other cardiac and thoracic surgeries. The review noted an interval of 1.5 to 23 years post-dTAA before symptoms appeared. Notably, only one patient in their review had undergone endovascular stent-graft placement.^1^
Thoracic endovascular aortic repair (TEVAR), introduced in the early 1990s, has become the primary treatment for high-risk patients with thoracic aortic disease.^3^
Chiesa et al. examined the incidence of aorto-oesophageal (AEF) and aortobronchial (ABF) fistulas following TEVAR. Of 1113 patients who underwent TEVAR from 1998 to 2008, 19 (1.7%) developed AEF or ABF. Among these, 13 (68%) involved the oesophagus, one (5%) affected the left bronchial tree, and five (26%) showed concurrent broncho-oesophageal involvement.^2^
Similarly, Czerny et al. analysed data from the European Registry of Endovascular Aortic Repair Complications, which included 4680 TEVAR patients across 14 European centres. They reported a 0.56% incidence of aortobronchial or aortopulmonary fistula following TEVAR. The primary causes of fistula formation included external compression of the bronchial tree, endoleak formation, and additional aortic ischaemia.^4^
Diagnostic modalities such as CT angiography, bronchoscopy, and aortography can be used to visualize the fistula tract. However, Piceche et al. found that direct visualization of the fistula was achieved only in rare cases.^1^
Regarding treatment, Piceche et al. found that untreated ABFs invariably result in death. All eight untreated patients in their study died from massive haemoptysis.^1^ Additionally, the patient mentioned in Chiesa et al.’s review also died when left untreated.^2^
Conclusion
This case highlights the diagnostic and management challenges of ABFs, emphasizing the need for a multidisciplinary approach. Regular follow-up with appropriate imaging is crucial to detect early recurrence. Patient education on symptom recognition and prompt reporting is essential. Multidisciplinary communication and early intervention if recurrence is suspected are paramount. Comprehensive management strategies are necessary to optimize patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Picichè M , De Paulis R, Fabbri A, Chiariello L. Postoperative aortic fistulas into the airways: etiology, pathogenesis, presentation, diagnosis, and management. Ann Thorac Surg 2003;75:1998–2006.12822663 10.1016/s 0003-4975(02)04837-3 · doi ↗ · pubmed ↗
- 2Chiesa R , Melissano G, Marone EM, Marrocco-Trischitta MM, Kahlberg A. Aorto-oesophageal and aortobronchial fistulae following thoracic endovascular aortic repair: a national survey. Eur J Vasc Endovasc Surg 2010;39:273–279.20096612 10.1016/j.ejvs.2009.12.007 · doi ↗ · pubmed ↗
- 3Dake MD , Miller DC, Semba CP, Mitchell RS, Walker PJ, Liddell RP. Transluminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med 1994;331:1729–1734.7984192 10.1056/NEJM 199412293312601 · doi ↗ · pubmed ↗
- 4Czerny M , Reser D, Eggebrecht H, Janata K, Sodeck G, Etz C, et al Aorto-bronchial and aorto-pulmonary fistulation after thoracic endovascular aortic repair: an analysis from the European Registry of Endovascular Aortic Repair Complications. Eur J Cardiothorac Surg 2015;48:252–257.25414427 10.1093/ejcts/ezu 443 · doi ↗ · pubmed ↗