Causal relationships of infection with Helicobacter pylori and herpesvirus on periodontitis: A Mendelian randomization study
Erli Wu, Ming Cheng, Shouxiang Yang, Wanting Yuan, Mengyun Gu, Dandan Lu, Lei Zhang, Qingqing Wang, Xiaoyu Sun, Wei Shao

TL;DR
This study used genetic data to investigate whether infections with Helicobacter pylori and herpesvirus cause periodontitis, but found no causal link in either direction.
Contribution
The study provides new genetic evidence that H. pylori and herpesvirus infections are not causally related to periodontitis.
Findings
Genetically predicted H. pylori and herpesvirus infections showed no causal association with periodontitis.
Reverse analysis also found no causal effect of periodontitis on these infections.
Sensitivity analyses confirmed the robustness of the MR results.
Abstract
To explore the causal association between Helicobacter pylori (H. pylori) infection, herpesvirus infection and periodontitis (PD) from a genetic perspective using Mendelian randomization (MR). The PD data were derived from genome-wide association study (GWAS) from the Dental Endpoints (GLIDE) consortium, and the FinnGen Biobank provided data on H. pylori and herpesvirus infections. In addition, we examined GWAS data for subtypes of H. pylori and herpesvirus infection. Inverse variance weighting (IVW) was selected as a major analysis technique, and weighted median (WM), weighted model, simple model, and MR-Egger regression were added as supplementary methods. To verify the findings, the effects of pleiotropy and heterogeneity were assessed. Genetically predicted H. pylori infection (OR = 0.914, 95%CI = 0.693–1.205, P = 0.523), anti-H. pylori VacA (OR = 0.973, 95%CI = 0.895–1.057, P =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
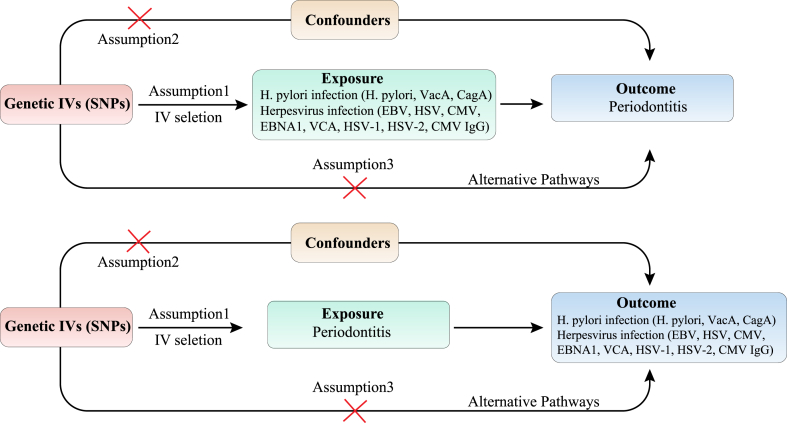 Figure 1
Figure 1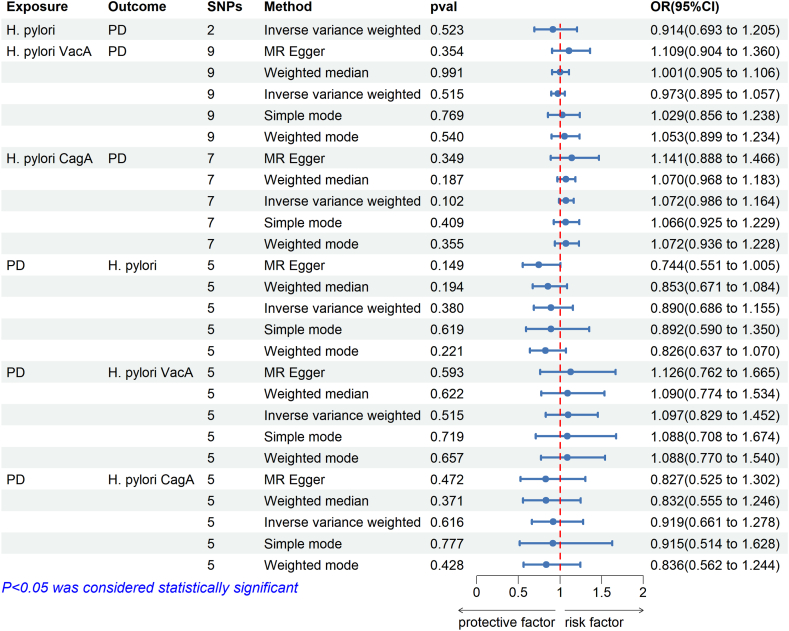 Figure 2
Figure 2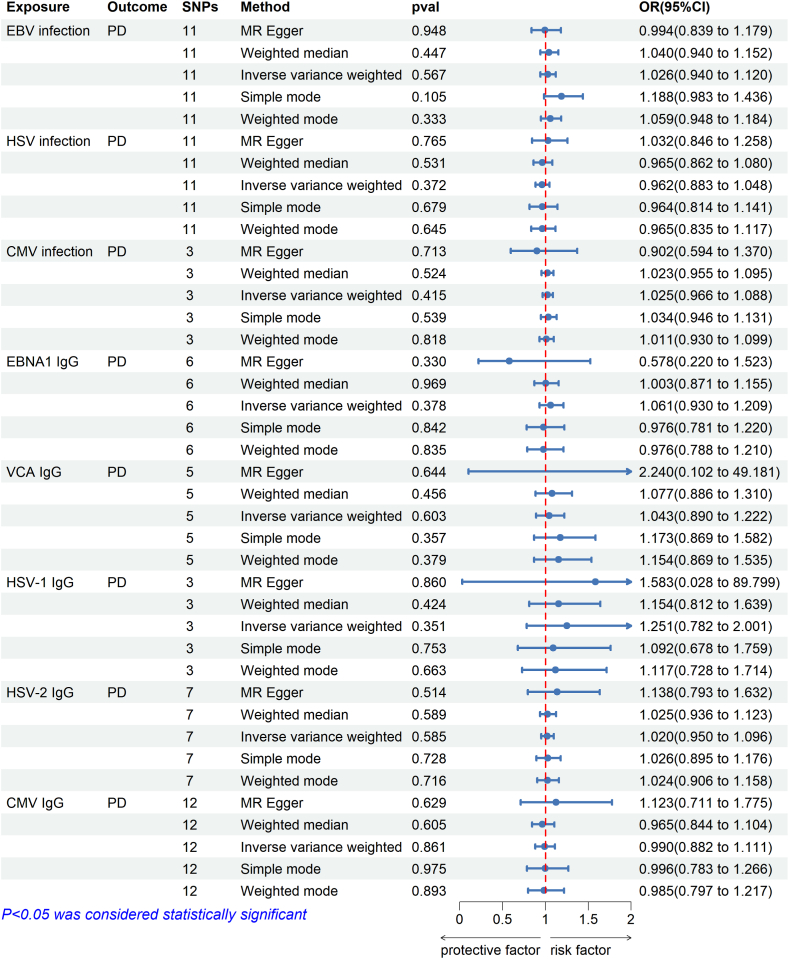 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsychedelics and Drug Studies · Music History and Culture · Comics and Graphic Narratives
Introduction
1
Periodontitis (PD) is a chronic oral disease characterized by plaque biofilm, causing deterioration of periodontal supporting tissues and the loss of teeth [1,2]. Due to its high incidence, PD has become the main cause of tooth loss in adults, which seriously affects the quality of life of patients [3]. According to epidemiological studies, mild to moderate PD affects 50 % of adults and has become the sixth greatest epidemic in human history [4].
The pathogenesis of PD is very complex, and the interaction between bacterial biofilm and the host immune system is the main factor in PD [5]. Some specific bacterial species, mainly gram-negative bacteria, such as Porphyromonas gingivalis (P. gingivalis), Fusobacterium nucleatum, Tannerella forsythia, and Treponema denticola, are closely associated with PD [6]. In addition, with the development of molecular biology, microbiology and other disciplines, studies have shown that certain viruses may affect the development of PD. These viruses may reduce the host's resistance and lead to local immune dysfunction, which is conducive to the colonization of periodontal pathogens. Furthermore, periodontal infection caused by bacteria allows viruses to infect cells and enter the gum tissue, exacerbating the damage [7].
Helicobacter pylori (H. pylori) and herpesvirus are among the most prevalent bacteria and viruses in humans, respectively, and have a high infection rate in the population. All of them can be latent in the mouth and may participate in the progression of PD by interacting with other oral microorganisms and reducing host resistance [8,9]. Specifically, H. pylori is a type of gram-negative bacterium that specifically resides in the epithelium of the human stomach and affects around 60 % of people all over the world [10]. H. pylori is intimately connected to gastritis and gastric ulcers (GC), and long-term infection with H. pylori will raise the risk of gastric malignant tumors [11]. Additionally, H. pylori is also implicated as a potential risk factor for numerous oral conditions, like PD [12]. P. gingivalis, the major pathogen of PD, was found to be altered by pre-incubation with H. pylori, which altered the virulence of P. gingivalis, including hemagglutination, biofilm development, and bacterial internalization into oral keratinocytes [13]. Additionally, there was a substantial rise in IL-6, IL-8, and INF-γ following stimulation of a human leukemia mononuclear cell line with cagA + H. pylori, indicating that H. pylori can exacerbate the course of inflammation [14]. An increasing number of studies have documented the detection of H. pylori in the supringival and subgingival plaques of PD patients, offering compelling evidence for the correlation between H. pylori and PD [[15], [16], [17]]. Some surveys have also found that infection with H. pylori raises the incidence of PD, and eradicating H. pylori may alleviate the progression of PD [9,11].
Similarly, herpesvirus is the most common virus in humans, and research has indicated that herpesvirus is a significant contributor to the etiology of PD and that co-infection of the virus with periodontal bacteria may be a major cause of PD [8]. Herpes simplex virus (HSV), cytomegalovirus (CMV) and Epstein-Barr virus (EBV) are herpesviruses closely related to PD, which can aggravate and damage periodontal tissues by infecting immune cells of periodontal patients and promoting the increase of periodontal pathogens [18]. Multiple studies have demonstrated that the detection rates of HSV, CMV, and EBV are increased in patients with PD compared to healthy controls [[19], [20], [21]]. It was also observed that in cases of PD, the presence of herpesvirus increased with the seriousness of the disease [22,23]. More recently, the use of stage I therapy in cases of chronic PD can also lead to short-term elimination of the virus at the lesion site [24].
However, these results are based on observational studies. Observational studies have several limitations including detection bias, residual and unmeasured confusion, and reverse causality [25]. In addition, there are several reports that do not observe an association between these diseases [19,26]. More significantly, finding any correlation between H. pylori and herpesvirus infections and the risk of PD has significant clinical and public health implications due to the high prevalence of H. pylori, herpesvirus infections, and PD in the population, as well as the relative ease and cost-effectiveness of treatment against H. pylori and herpesvirus infections. For these reasons, better methods are needed to assess the causal effects of H. pylori and herpesvirus infection on the pathogenesis of PD. Therefore, improved methods are required to evaluate the causal relationships between these diseases.
Mendelian randomization (MR), an epidemiology technique, uses multiple single-nucleotide polymorphisms (SNPs) as genetic instrumental variables (IVs) to evaluate causality in a proposed exposure-outcome pathway. Since SNPs are distributed at random during conception, it can prevent reverse causality and other confounding consequences [27]. In this study, we assessed the causality of H. pylori and herpesvirus infection for PD by using MR analysis. Also, a reverse MR study was also performed.
Materials and methods
2
Study design and materials
2.1
SNPs indicating genetic variation were chosen as instrumental variables (IVs) for two-sample MR analysis. IVs were required to fulfill three conditions: (1) IVs have a strong and direct relationship with exposure; (2) IVs are not subject to confounding factors; (3) IVs exclusively influence outcomes through exposure [28,29]. The causality of H. pylori and herpesvirus infection on PD was evaluated through MR analysis. Subsequently, we performed a reverse MR analysis with PD as the exposure and H. pylori and herpesvirus infection as the outcomes. Fig. 1 showed a schematic of the MR study between H. pylori infection, herpesvirus infection, and PD.Fig. 1. Flowchart of this MR analysis. Abbreviations: SNPs, single-nucleotide polymorphisms; H. pylori, Helicobacter pylori; VacA, Vacuolar cytotoxin A; CagA, Cytotoxin-associated protein A; EBV, Epstein-Barr virus; HSV, Herpes simplex virus; CMV, cytomegalovirus; EBNA1, EBV nuclear antigen-1; VCA, EBV virus capsid antigen; HSV-1, HSV type 1; HSV-2, HSV type 2.Fig. 1
Data source
2.2
The latest meta-analysis of GWAS from the Gene-Lifestyle Interaction in the Dental Endpoints (GLIDE) consortium provided summary statistics for PD. This study has the biggest sample size to date, consisting of 28,210 controls and 17,353 clinically diagnosed cases [30]. The Community Periodontal Index (CPI) or the Centers for Disease Control and Prevention/American Academy of Periodontology (CDC/AAP) case definitions were used to categorize PD cases. Alternatively, the number of deep periodontal pockets and the depth of probing were utilized to determine the PD diagnostic report of study participants [30]. The European Bioinformatics Institute database, which comprised 1058 patients and 3625 healthy individuals, provided the GWAS summary information for H. pylori infection. Samples from both databases were of European descent. In addition, we also collected GWAS data on subtypes of infection with H. pylori to explore the causation between infection with H. pylori and PD, which included anti-H. pylori VacA and anti-CagA. Aggregated GWAS statistics for anti-H. pylori VacA and anti-CagA were from the UK Biological Sample Database, which included 1571 and 985 samples, respectively. Moreover, we used the GWAS data from the FinnGen biobank analysis for herpesvirus infection. In the latest version, EBV infection (R10) included 2979 cases and 400,974 controls; HSV infection (R10) included 3723 cases and 396,378 controls; CMV (R7) included 428 cases and 301,439 controls. Besides these, we also used GWAS data on circulating antibody IgG levels associated with several herpesvirus subtypes including EBV nuclear antigen-1 (EBNA1), EBV virus capsid antigen (VCA), CMV, HSV type 1 (HSV-1) and HSV type 2 (HSV-2). The samples were collected from the Milieu Interieur cohort, which comprises 1000 healthy individuals who were tested with a 2200 IgG kit for sero-specific IgGTM against various herpevirus antigens [31]. Table 1 displayed the specifics of the GWAS data used in this study.Table 1. Details of the studies in the mendelian randomization analysis.Table 1. PhenotypeConsortiumPopulationSample sizeCasesControlsAccess LinkPDGLIDEEuropean45,56317,35328,210https://data.bris.ac.uk/data/dataset/2j2rqgzedxlq02oqbb4vmycnc2Anti-H. Pylori IgG levelsEBIEuropean468310583625https://gwas.mrcieu.ac.uk/datasets/ieu-b-4905/H. pylori VacA antibody levelsEuropean1571––https://gwas.mrcieu.ac.uk/datasets/ebi-a-GCST90006916/H. pylori CagA antibody levelsEuropean985––https://gwas.mrcieu.ac.uk/datasets/ebi-a-GCST90006911/EBV infectionFinnGen cohortEuropean403,9532979400,974https://r10.finngen.fi/HSV infectionEuropean400,1013723396,378https://r10.finngen.fi/CMV infectionEuropean301,867428301,439https://r7.finngen.fi/EBNA1 IgGMilieu Intérieur cohortEuropean100091486https://doi.org/10.5281/zenodo.1217136VCA IgGEuropean100095644HSV-1 IgGEuropean1000645355HSV-2 IgGEuropean1000208792CMV IgGEuropean1000347653Abbreviations: H. pylori, Helicobacter pylori; VacA, Vacuolar cytotoxin A; CagA, Cytotoxin-associated protein A; PD, periodontitis; GLIDE, Gene-Lifestyle Interaction in the Dental Endpoints; EBI, European Bioinformatics Institute; EBV, Epstein-Barr virus; HSV, herpes simplex; CMV, cytomegalovirus; EBNA1, Epstein-Barr virus nuclear antigen-1; VCA, EBV viral capsid antigen; HSV-1, HSV type 1; HSV-2, HSV type 2.
IV selection
2.3
Genetic IV can be acquired through GWAS aggregated data analysis or a literature search. The H. pylori infection's genetic IV was provided by a prior investigation carried out by Mayerle et al. [32]. Two SNPs, rs10004195 and rs368433, were shown to be independently and highly linked with seropositivity for H. pylori in their investigation of a European population, which comprised 2763 cases and 8175 controls, as indicated in Table S1. Consequently, these 2 SNPs were chosen for IVs linked to H. pylori infection and were employed in subsequent analyses. For other GWAS summary data, to satisfy three assumptions of MR analysis, IVs were obtained in accordance with p < 5 × 10^−6^ to obtain more SNPs. Then, we removed SNPs that have a substantial linkage imbalance (LD) by filtering them out with the aggregation software R^2^ = 0.001*,* clumping distance = 10,000 kb [33]. Additionally, each SNP's F statistic is determined using the following equation: (1) F = R^2^ × (N-2)/(1-R^2^) or (2) F = beta^2^/se^2^. R^2^ is a representation of the exposure variability for each IV interpretation [34,35]. An IV will not be included in the MR analysis if its F statistic is less than 10, which is regarded as a poor instrument. In order to confirm the second MR hypothesis, we scanned the PhenoScannerV2 database for IV and its proxy qualities and excluded SNPs that may affect the outcome due to other confounding variables [36,37]. Finally, palindrome SNPs were omitted to avoid the effect of alleles on the outcome of the causal association between the diseases [38].
MR analysis
2.4
The study was statistically analyzed using R (version 4.3.1). For MR analysis, the "TwoSampleMR” package in R was used to find any potential causative relationships between H. pylori infection, herpesvirus infection and PD [39]. Inverse variance weighting (IVW) was employed in the main study [40]. As additional techniques for MR analysis, weighted median, weighted models, simple models, and MR-Egger regression were applied [41]. The 95 % confidence interval (CI) and odds ratio (OR) serve as the main effect measures in this investigation. If OR>1, it is demonstrated that the factor can encourage the outcome to occur; if not, the reverse [42]. P < 0.05 was used as the significance criterion to detect plausible causal effects.
Sensitivity analysis
2.5
After MR analysis, the Cochran's Q test was employed to assess heterogeneity in the IVW and MR Egger regression methods. If P > 0.05, we considered that the results of the study were not affected by heterogeneity [24]. The Pleiotropy Residual Sum and Outlier (MR PRESSO) and MR-Egger methods were used to analyze the pleiotropy between SNPs as instrumental factors [43]. If P > 0.05, pleiotropy was not present in causal analysis, and its effects may be ignored. The MR-Egger regression can identify and correct pleiotropy [44]. Furthermore, the MR-PRESSO approach could identify whether horizontal pleiotropy exists based on a global test. If it is found, it offers estimates derived from this analysis that are adjusted for horizontal pleiotropy by eliminating potential outliers [45]. Additionally, a leave-one-out approach was used, systematically excluding each SNP throughout the MR analysis to identify any SNPs that potentially had an impact [46].
Results
3
Causal effect of H. pylori infection on PD
3.1
The MR analysis results were displayed in Fig. 2 rs10004195 and rs368433, two SNPs highly connected to H. pylori infection, had F-statistics of 558.639 and 289.986, respectively, which prevented weak IVs from affecting causality. MR analysis revealed that IVW (OR = 0.914, 95%CI = 0.693–1.205, P = 0.523), indicating that H. pylori infection had no effect on PD.Fig. 2. Causal estimates between H. pylori infection and PD given as odds ratios (ORs) and 95 % confidence intervals. SNPs, single-nucleotide polymorphisms; H. pylori, Helicobacter pylori; OR, Odds ratio; 95 % CI, 95 % confidence intervals; VacA, Vacuolar cytotoxin A; CagA, Cytotoxin-associated protein A; PD, periodontitis.Fig. 2
In addition, analysis was performed on the two main subtypes of H. pylori infection: H. pylori VacA antibody and H. pylori CagA antibody. 9 and 7 SNPs were eventually accepted to analyze the causal effect of VacA and CagA on PD in the MR study. In Tables S2–S3, the IVs used for MR analyses were fully described. The MR estimates showed no causal impact of VacA (OR = 0.973, 95%CI = 0.895–1.057, P = 0.515) and CagA (OR = 1.072, 95%CI = 0.986–1.164, P = 0.102) on PD. The findings from the WM and MR Egger tests were in agreement with IVW methods.
The results of the sensitivity analysis showed no heterogeneity or directional pleiotropy in VacA and CagA studies on PD, indicating that our MR results were robust (Table 2). The leave-one-out analysis showed no outliers existed, suggesting that a specific SNP did not impact the findings. The scatter plots, leave-one-out analyses, and funnel plots of the MR analyses were displayed in Figs. S1–S3.Table 2. The sensitivity analysis of MR study between H. pylori infection and PD.Table 2. ExposureOutcomeSNPsIVWMR-Egger regressionMRPRESSOQ statisticQ_pvalInterce ptP-valueRSSobsP-valueH. pyloriPD28.5190.004––––VacAPD911.5160.174−0.0370.21520.7860.175CagAPD77.0510.316−0.0210.62212.3600.348PDH. Pylori IgG58.1730.0850.0440.19221.3720.054VacA50.1730.996−0.0060.8650.4681.000CagA51.2230.8740.0280.55413.1990.256Abbreviations: MR, Mendelian randomization; SNPs, single-nucleotide polymorphisms; IVW, inverse variance-weighted method; H. pylori, Helicobacter pylori; VacA, Vacuolar cytotoxin A; CagA, Cytotoxin-associated protein A; PD, periodontitis.
Causal effect of PD on H. pylori infection
3.2
8 SNPs as IVs were identified for PD after filtering out weak IVs and LD. They are all highly correlated with exposure (F > 10). Then, by combining the outcome database and removing SNPs that were palindromic, 5 SNPs were approved for MR estimates of PD on IgG for H. pylori infection, anti-H. pylori VacA, and anti-CagA. Table S4 showed the details of the SNPs associated with PD.
We did not find an impact of PD on anti*-H. pylori* IgG levels (OR = 0.890, 95%CI = 0.686–1.155; P = 0.380), anti-H. pylori VacA (OR = 1.097, 95%CI 0.829–1.452; P = 0.515) and anti-H. pylori CagA (OR = 0.919, 95%CI = 0.661–1.278, P = 0.615). The findings from the WM and MR Egger tests were in agreement with IVW.
The sensitivity analysis confirmed the absence of horizontal pleiotropy or heterogeneity. No abnormal SNPs were observed in both the leave-one-out MR analysis and the MR-PRESSO regression methods.
Causal effect of herpesvirus infection on PD
3.3
58 SNPs were used for herpesvirus infection on PD after filtering, which all have an F statistic greater than 10 (ranging from 20.983 to 47.626). Table S5 showed the details of the SNPs associated with the herpesvirus.
Fig. 3 illustrated the effect between each herpesvirus and PD using the IVW approach. Specifically, in the FinnGen cohort, genetically predicted EBV infection (OR = 1.026, 95%CI = 0.940–1.120, P = 0.567), HSV infection (OR = 0.962, 95%CI = 0.883–1.048, P = 0.372), and CMV infection (OR = 1.025, 95%CI = 0.967–1.088, P = 0.415) were not associated with PD risk. In the Milieu Interieur cohort, we found no correlations between herpesvirus-related IgG EBNA1 (OR = 1.061, 95%CI = 0.930–1.209, P = 0.378), VCA (OR = 1.043, 95CI% = 0.890–1.222, P = 0.603), HSV-1 (OR = 1.251, 95%CI = 0.782–2.001, P = 0.351), HSV-2 (OR = 1.020, 95%CI = 0.950–1.096, P = 0.585), CMV (OR = 0.990, 95CI% = 0.882–1.111, P = 0.861) and PD risk.Fig. 3. Causal estimates between herpesvirus infection and PD given as odds ratios (ORs) and 95 % confidence intervals. SNPs, single-nucleotide polymorphisms; H. pylori, Helicobacter pylori; OR, Odds ratio; 95 % CI, 95 % confidence intervals; EBV, Epstein-Barr virus; HSV, Herpes simplex virus; CMV, cytomegalovirus; EBNA1, EBV nuclear antigen-1; VCA, EBV virus capsid antigen; HSV-1, HSV type 1; HSV-2, HSV type 2; PD, periodontitis.Fig. 3
In the sensitivity analysis, according to the Cochran's Q test, no heterogeneity was detected between the instrumental SNP effects of the herpesvirus, except for HSV-1. Therefore, the random effects model was used for the MR analysis of HSV-1. Additionally, the MR-Egger intercept and MR-PRESSO global tests revealed no indication of horizontal pleiotropy (Table 3). The leave-one analysis, forest plot, and scatter plot showed that our results are reliable and consistent with our earlier testing (Figs. S4–S6).Table 3. The sensitivity analysis of MR study between herpesvirus infection and PD.Table 3. ExposureOutcomeSNPsIVWMR-Egger regressionMRPRESSOQ statisticQ_pvalInterce ptP-valueRSSobsP-valueEBV infectionPD1116.7200.0810.0080.67823.0250.127HSV infection115.6250.846−0.0130.4626.5100.914CMV infection30.7130.7000.0540.6531.8770.797EBNA1 IgG67.8920.1620.1010.28311.4670.267VCA IgG55.2660.261−0.0830.6607.7980.395HSV-1 IgG36.6710.036−0.0240.92710.4730.154HSV-2 IgG72.6910.846−0.0220.5713.8640.873CMV IgG1217.6710.090−0.0250.58720.6710.270PDEBV infection611.2070.047−0.0200.56915.4310.263HSV infection62.1960.821−0.0080.6934.3350.877CMV infection61.9480.8560.0040.9458.0010.674EBNA1 IgG30.6260.7310.0070.9201.8480.878VCA IgG33.2680.195−0.0130.90015.6990.071HSV-1 IgG31.9610.375−0.0200.71413.0100.125HSV-2 IgG30.5430.762−0.0300.7413.4400.711CMV IgG217.6710.090−0.0250.58720.6710.270Abbreviations: MR, Mendelian randomization; SNPs, single-nucleotide polymorphisms; IVW, inverse variance-weighted method; EBV, Epstein-Barr virus; HSV, Herpes simplex virus; CMV, cytomegalovirus; EBNA1, EBV nuclear antigen-1; VCA, EBV virus capsid antigen; HSV-1, HSV type 1; HSV-2, HSV type 2; PD, periodontitis.
Causal effect of PD on herpesvirus infection and subtypes
3.4
In the reverse MR study, we also did not find an association between PD and herpesvirus infection. In particular, the p-value of PD for all herpesvirus infections and their subtypes was greater than 0.05, suggesting that there is no causal effect of PD on herpesvirus infections (Fig. S7). Table S6 documented the IVs associated with PD for herpesvirus infection.
Except for EBV infection, which had a P-value of less than 0.05 and thus used a random effects model, the heterogeneity test results were all P > 0.05, which meant no heterogeneity effect in the results of MR analysis. We performed MR PRESSO to check for horizontal pleiotropy, and the results were all P > 0.05, which indicated there was no effect of horizontal pleitropy. A leave-one-out test was also performed to test each SNP and the results indicated that it was unlikely that a single SNP affected the MR results. Therefore, the results of the MR analysis were believed to be reliable and stable.
Discussion
4
In this study, we explored the causal effect of H. pylori infection and herpesvirus infection on PD using MR methods. The findings of the MR study did not uncover any proof linking H. pylori and herpesvirus infections to PD. The results of the reverse MR study were consistent with the aforementioned results. The results of the sensitivity analysis suggested the reliability and robustness of our MR analysis results.
The oral cavity, as the entrance and initial component of the gastrointestinal system, has been generally recognized by researchers as a primary extra-gastric reservoir of H. pylori [47,48]. Therefore, H. pylori is also thought to be a possible bridge between gastrointestinal diseases and PD. A meta-analysis reported a strong association between the presence of H. pylori in the oral cavity and in the stomach [49]. Other studies have found that 83.3 % of the patients with H. pylori in the oral cavity were also positive for the bacterium in gastric samples [50]. In addition, poor oral hygiene and microaerobic conditions caused by chronic PD infections favor H. pylori colonization of the periodontal pouch, suggesting that even if H. pylori is eradicated from the stomach, dental plaque can become a sanctuary for H. pylori and have an impact on re-infection, leading to a recurrence of stomach ulcers [51,52]. A recent MR study also suggested that PD was associated with an increased risk of GC, and the pathway may be associated with H. pylori in oral [53]. Moreover, the occurrence of oral H. pylori infections is directly related to the oral hygiene and periodontal health status of an individual, and the improvement of oral hygiene and oral health may increase the inhibition rate of gastric H. pylori infection [54]. The above-mentioned studies suggest that there may be a reciprocal relationship between H. pylori-induced PD and H. pylori-induced GC.
Some observational studies have examined the links between infection with H. pylori and PD. According to research including 14 individuals with chronic PD, patients who had H. pylori had more loss of attachment and deeper probing depth than those who did not [14]. Another cross-sectional study involving 53 volunteers also discovered a relationship between the existence of PD and genotypes and rates of detection of H. pylori in subgingival plaque [55]. Riggio et al. [15] identified H. pylori in the sub-gingival plaque of adults with PD through the PCR technique. Additionally, a study involving 4955 participants between the ages of 20 and 90 who underwent periodontal exams and serum testing for H. pylori was conducted to examine a correlation between PD and infection with H. pylori, suggesting a strong connection between PD and a higher probability of infection with H. pylori in comparison to good periodontal health (OR = 1.271, 95 % CI = 1.177–1.372) [12]. Furthermore, a case-control study showed that adults with poorer oral hygiene exhibited greater H. pylori levels detected in stomachs and dental plaque [56]. Moreover, a meta-analysis involving 2727 participants from Asia revealed a connection between oral H. pylori infection and PD (OR = 2.53; 95%CI = 1.86–3.44, P < 0.05) [47]. Another meta-analysis including eight studies suggested that the possibility of H. pylori infection was 2.47 times higher in individuals with PD (OR = 2.47; 95%CI = 2.01–3.03; P = 0.001) [57]. In addition, two meta-analyses reported that combined periodontal treatment can reduce gastric H. pylori rates [58,59]. Nevertheless, certain research findings showed no association between H. pylori infection and PD. A case-control study involving 134 participants showed no correlation between infection with H. pylori and patients with poor oral hygiene and PD [26]. Another case-control study involving 100 participants revealed no significant correlation between H. pylori presence in gingival crevicular fluid and PD status (P = 0.200) [60]. Moreover, a meta-analysis including four observational studies indicated no links between H. pylori and PD [61]. Furthermore, a study involving 959 healthy Japanese adults found that H. pylori infection was positively correlated with tooth loss in males, but negatively correlated with the prevalence of PD in females [62].
Herpesvirus infection is another disease with a high prevalence in the population, which may influence the development of PD by reducing the resistance of periodontal tissues and decreasing host resistance to periodontal pathogens [63]. A study by Contreras et al. [64] using nested polymerase chain reaction in 15 human samples indicated an increased detection rate of CMV and EBV-1 in PD lesions than that in healthy periodontal sites. According to a case-control study involving 20 healthy participants, 40 gingivitis patients, and 40 patients with chronic PD, the levels of HSV-1 and EBV detection in chronic PD patients were considerably greater than those in the healthy controls (P < 0.001). Furthermore, a positive correlation was seen between the incidence of EBV in patients suffering from chronic PD and a rise in gingival index, probing depth, and loss of clinical attachment (P < 0.05) [65]. A meta-analysis showed a significant correlation between EBV, CMV and PD [66]. Moreover, Kubar et al. [67] discovered that invasive PD lesions had a greater incidence of CMV and EBV DNA copies in the gum tissue and periodontal pocket than did chronic PD lesions, indicating a possible correlation between the herpesvirus count and the severity of PD. Puletic et al. [68] also collected subgingival samples from 39 periodontal abscesses, 33 necrotizing ulcerative PD, 27 chronic PD and 30 healthy controls, conducted PCR analysis for microbial detection, and found higher detection rates of EBV and CMV in severe PD patients than those in healthy subjects and patients with moderate PD. Nevertheless, some studies have shown no relationship between the herpesvirus and the prevalence of PD. Nibali et al. [19] performed PCR analysis to detect CMV and EBV in 140 ethnically mixed (predominantly Caucasian) subjects including 16 affected by limited invasive PD, 64 affected by generalized aggressive PD, 20 affected by chronic PD, and 40 healthy controls. The sample size of this study was much larger than the other studies, and the results of this study found that CMV DNA was undetectable in all plaque samples and only a small percentage of PD patients and healthy controls carried EBV. Dawson et al. [69] found a rare rate of both CMV and EBV in the subgingival region of patients with chronic PD by conducting a PCR test with 65 chronic PD subjects. Another controlled trial involving 65 patients with aggressive PD and 65 healthy controls discovered that there was no significant difference between the patient and control groups in terms of serum IgG against HSV-1 (76.1 % versus 73.9 %), EBV (98.5 % versus 96.9 %), CMV (47.7 % versus 46.2 %), or IgM levels against HSV-1 (6.2 % versus 1.5 %), EBV (0 % versus 0 %), or CMV (0 % versus 1.5 %) [70].
The discrepancies in the relationship between herpesvirus infection, H. pylori infection, and PD have numerous plausible causes. Firstly, in these observational epidemiological studies, there is no prospective, randomized, or blind approach. Biases related to reverse causality, selection bias, and inappropriate confounding control can all affect the differences in results. For herpesvirus, the majority of research that find a positive association with PD use sample sizes of less than thirty, which restricts the generalizability of the findings [70]. Secondly, different studies used different methodologies to diagnose H. pylori infection and herpesvirus infection. The World Gastroenterology Organization (WGO) has endorsed urine breath testing as the gold standard for non-invasive methods of detecting H. pylori [71]. Nevertheless, the diagnostic standards for H. pylori infection vary throughout research since some measure infection with H. pylori with blood, anti-H. pylori IgG or DNA sequences of H. pylori. For herpesviruses, the majority of prior assays are nested PCRs. Despite the fact that this approach is more sensitive than PCR, cross-contamination could lead to false positive results [72]. Thirdly, changes in age, sex, region, ethnicity, dietary habits, and socioeconomic status, as well as the titer of H. pylori and herpesvirus IgG, and the type and level of H. pylori and herpesvirus antibodies, all contributed to differences in results [[73], [74], [75]]. For instance, the prevalence of H. pylori is typically greater than 50 % in communities in Southern and Eastern Europe, South America, and Asia, but roughly one-third of people in Northern and North American populations are still infected [76]. Germany has a high seropositivity rate for HSV-1, ranging from 85.2 % (west) to 88.5 % (east). Furthermore, in Germany, the HSV-1 seroprevalence rate for youth is over 60 %, the rate for individuals between the ages of 35 and 44 is over 80 %, and the rate for the elderly is around 100 % [75]. A survey of CMV prevalence in the United States showed that age (36 % in childhood, 91 % in people aged 80) and race (51 % for non-Hispanics, 76 % for non-Hispanic blacks, and 82 % for Mexican Americans) had a significant impact [77]. The prevalence of EBV in the 30–40 year age group in Western and Central Europe is close to 90 %, while the positive rate in the Central African population is close to 100 %, and the seroprevalence in the United States depends on socioeconomic status [78]. Finally, the characteristic incubation period of herpesvirus can also lead to differences in the detection rate of herpesvirus [79,80].
MR analysis can generate reasonably accurate causal assessments by employing genetic IVs, thus circumventing the impact of these confounding factors [27,81]. Our study has several benefits. Firstly, this is the first research to examine the bidirectional causation between infection with H. pylori, herpesvirus and PD using the MR method. This approach can minimize the effects of confounding variables and reverse causality. Secondly, we used multiple GAWS data on subtypes of H. pylori and herpesvirus infections to further strengthen the robustness of the conclusions we obtained. Nevertheless, there are some restrictions on our investigation. Initially, individuals with European ancestry are the only subjects of our investigation. It cannot be demonstrated that this is applicable to other racial populations, despite the fact that it would lessen the bias brought about by population stratification. Furthermore, as previously stated, there are racial and geographic differences in the prevalence of H. pylori and herpesvirus in patients with PD; therefore, the census population's racial and geographic distributions must be expanded. Secondly, IVs chose a 5e-06 p-value threshold, which might somewhat influence the final estimate due to instrumental bias. Thirdly, due to the limited sample size of H. pylori and herpesvirus infection-associated GWAS, higher sample sizes will need to be studied in future studies to support the MR analysis. Finally, it is unknown whether study subjects with GWAS data on H. pylori, herpesvirus, and PD have used antibiotics now or in the past year, which may affect the readability of our results. The use of antibiotics may omit the detection of patients with H. pylori infection and patients with PD. Furthermore, using antibiotics may cause resistance to arise, which may result in genetic loci changing. For instance, mutations in the 23S rRNA, rdxA, frxA, fdxB, gyrA and gyrB loci allow H. pylori to avoid the associated antibiotic activity by preventing the synthesis of bacterial proteins, preventing the intracellular reductive activation of metronidazole (MTZ), and preventing the transcription and replication of bacterial DNA, respectively [82,83].
Conclusions
5
Taken together, our MR analysis failed to find a causal effect of H. pylori and herpesvirus infection on PD or vice versa. This implies that eradicating or preventing H. pylori and herpesvirus may not be beneficial for PD. Nevertheless, due to restrictions related to geography and ethnicity as well as the modest size of the GWAS sample size data, the results we obtained should be interpreted cautiously.
Ethics statement
The data of this study were obtained from public databases, having obtained informed consent from all participating studies in accordance with the protocols approved by their institute's ethics committee. No separate ethical approval is required for this study.
Funding
This work was supported by the 10.13039/501100001809National Natural Science Foundation of China (82071770); Research Level Improvement Project of 10.13039/501100002947Anhui Medical University (2021xkjT001); 10.13039/501100003995Anhui Provincial Natural Science Foundation (2008085QH371); Scientific Research of BSKY in 10.13039/501100002947Anhui Medical University (XJ201601); Research and practical innovation projects of 10.13039/501100002947AHMU (YJS20230039); Basic and Clinical Cooperative Research and Promotion Program of 10.13039/501100002947Anhui Medical University (2021xkjt039); 10.13039/501100003995Natural Science Foundation of Anhui Province (2208085QH245) and the 10.13039/501100001809National Natural Science Foundation of China (82201127).
Data availability statement
The GWAS data related to PD were sourced from the GLIDE consortium at https://data.bris.ac.uk/data/dataset/2j2rqgzedxlq02oqbb4vmycnc2. The summary-level data for H. pylori infection, VacA and CagA were obtained from the EBI consortium, available at https://www.ebi.ac.uk/gwas/home/. The FinnGen website provided GWAS data on EBV, CMV and HSV infections. The GWAS data on antibody IgG of EBNA1, VCA, CMV, HSV-1 and HSV-2 were sourced from the Milieu Intérieur cohort at https://doi.org/10.5281/zenodo.1217136.
CRediT authorship contribution statement
Erli Wu: Writing – original draft. Ming Cheng: Project administration. Shouxiang Yang: Data curation. Wanting Yuan: Data curation. Mengyun Gu: Software. Dandan Lu: Methodology. Lei Zhang: Investigation. Qingqing Wang: Funding acquisition. Xiaoyu Sun: Formal analysis. Wei Shao: Writing – review & editing.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Genco R.J.Sanz M.Clinical and public health implications of periodontal and systemic diseases: an overview Periodontol 8312000. 202071310.1111/prd.1234432385880 · doi ↗ · pubmed ↗
- 2Kinane D.F.Stathopoulou P.G.Papapanou P.N.Periodontal diseases Nat. Rev. Dis. Prim.320171703810.1038/nrdp.2017.3828805207 · doi ↗ · pubmed ↗
- 3Ma C.Periodontitis and stroke: a Mendelian randomization study Brain Behav 1322023 e 288810.1002/brb 3.2888 PMC 992783236621868 · doi ↗ · pubmed ↗
- 4Marouf N.Association between periodontitis and severity of COVID-19 infection: a case-control study J. Clin. Periodontol.484202148349110.1111/jcpe.1343533527378 PMC 8014679 · doi ↗ · pubmed ↗
- 5Darveau R.P.Periodontitis: a polymicrobial disruption of host homeostasis Nat. Rev. Microbiol.87201048149010.1038/nrmicro 233720514045 · doi ↗ · pubmed ↗
- 6Hajishengallis G.Periodontitis: from microbial immune subversion to systemic inflammation Nat. Rev. Immunol.1512015304410.1038/nri 378525534621 PMC 4276050 · doi ↗ · pubmed ↗
- 7Teles F.Viruses, periodontitis, and comorbidities Periodontol 8912000. 202219020610.1111/prd.1243535244970 · doi ↗ · pubmed ↗
- 8Chen C.Feng P.Slots J.Herpesvirus-bacteria synergistic interaction in periodontitis Periodontol 8212000. 2020426410.1111/prd.12311 PMC 738244631850623 · doi ↗ · pubmed ↗