Splenic Artery Pseudoaneurysm Management With Cyanoacrylate Glue: A Case Report
Sudhanshu Tonpe, Himandri Warbhe, Pankaj Banode, Shubham Waghulkar, Shubham Dugad, Manasa Suryadevara, Swaroop Reddy Guggella

TL;DR
A 40-year-old woman with a splenic artery pseudoaneurysm was successfully treated with cyanoacrylate glue embolization, preventing life-threatening bleeding.
Contribution
This case report highlights the successful use of cyanoacrylate glue for managing a splenic artery pseudoaneurysm.
Findings
Endovascular cyanoacrylate glue embolization resolved the pseudoaneurysm.
The treatment prevented catastrophic hemorrhagic shock in the patient.
Abstract
We present the case of a 40-year-old female who presented with abdominal pain, hematochezia, and melena for the past week and was diagnosed with a pseudoaneurysm emanating from the mid-splenic artery. The patient was managed with endovascular cyanoacrylate glue embolization, resulting in the complete resolution of an impending catastrophic hemorrhagic shock.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
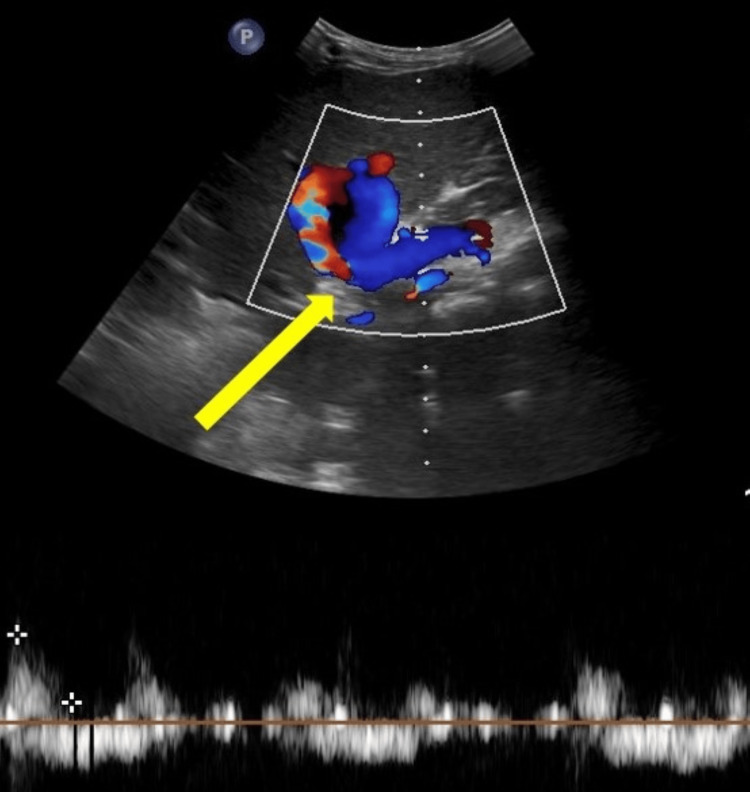 Figure 1
Figure 1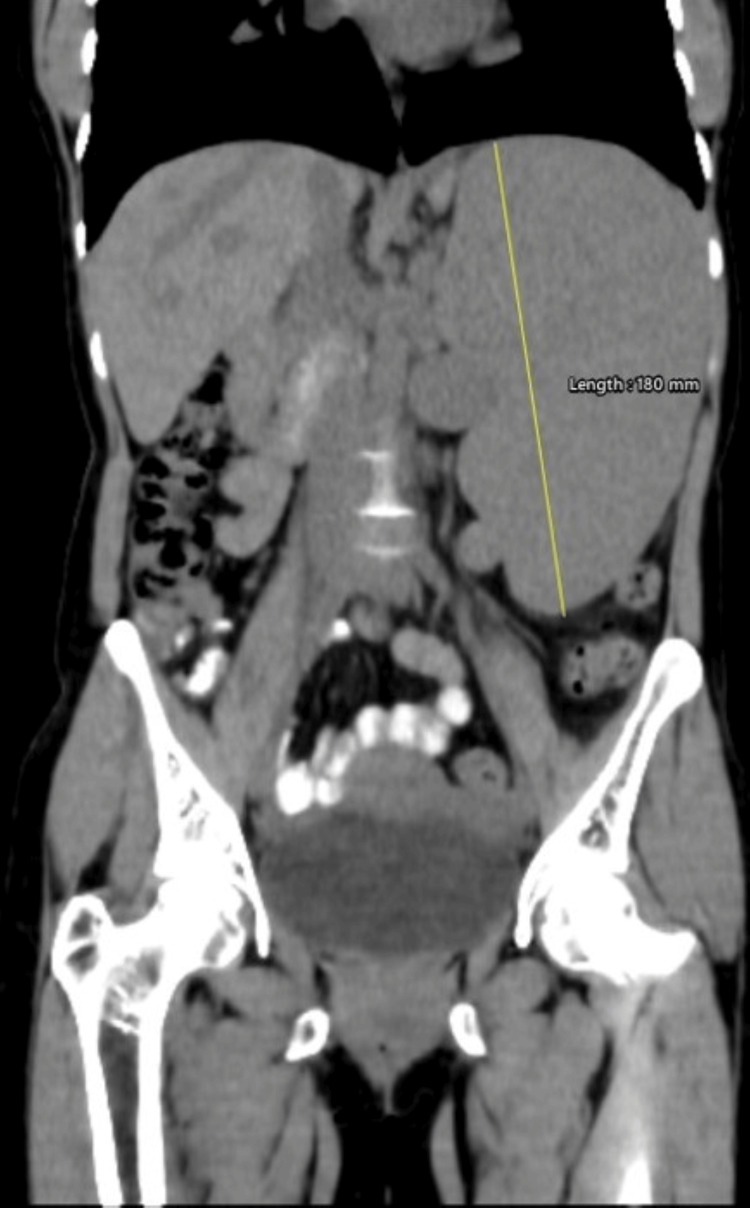 Figure 2
Figure 2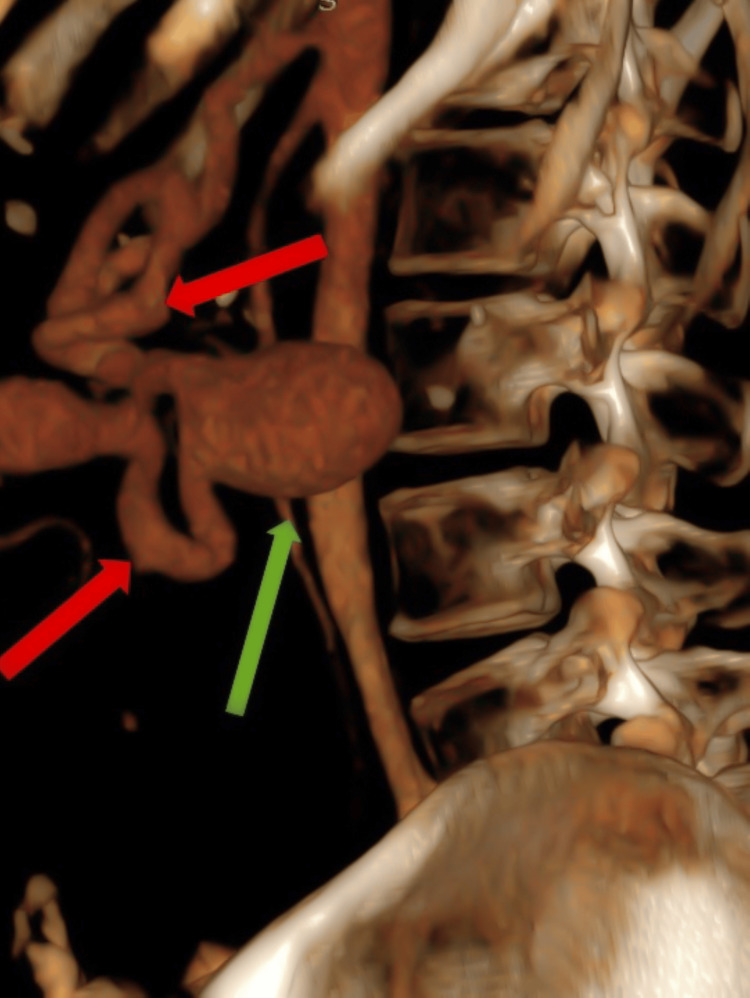 Figure 3
Figure 3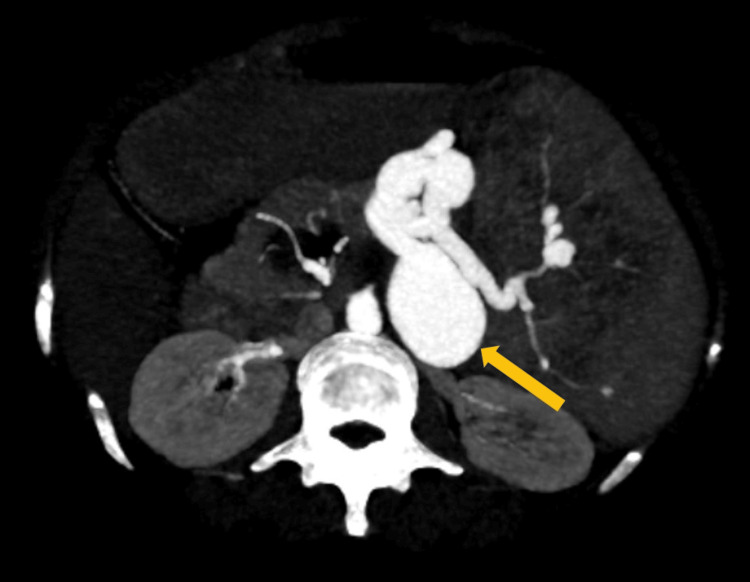 Figure 4
Figure 4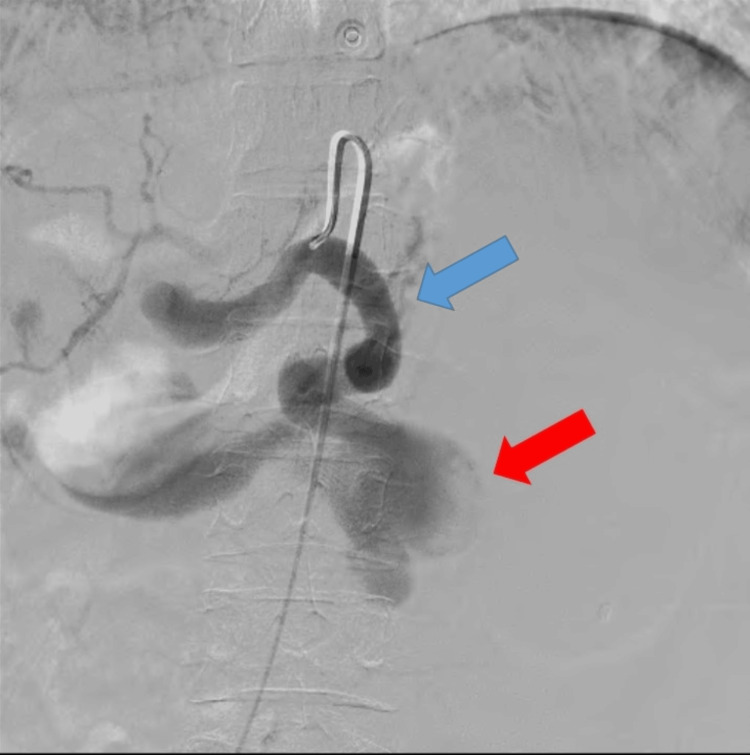 Figure 5
Figure 5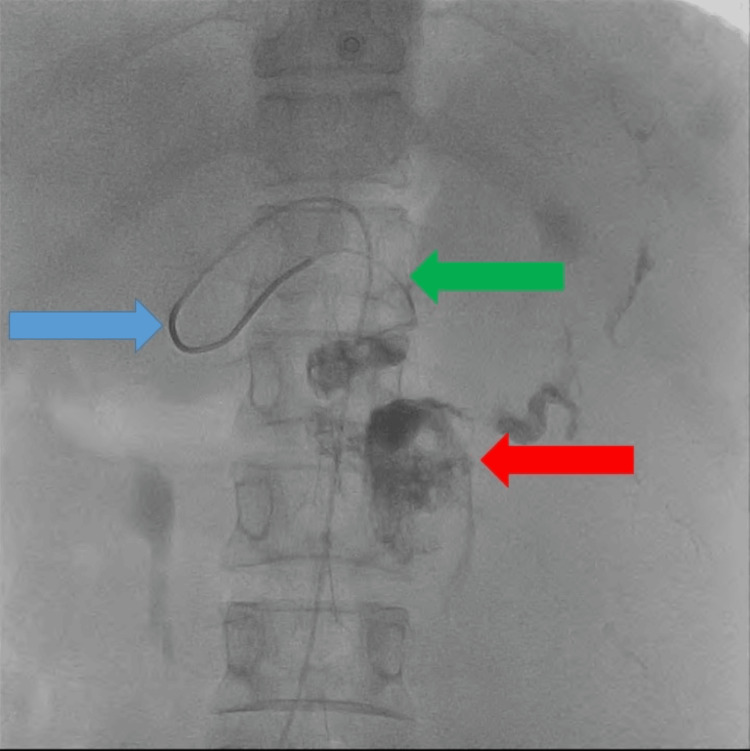 Figure 6
Figure 6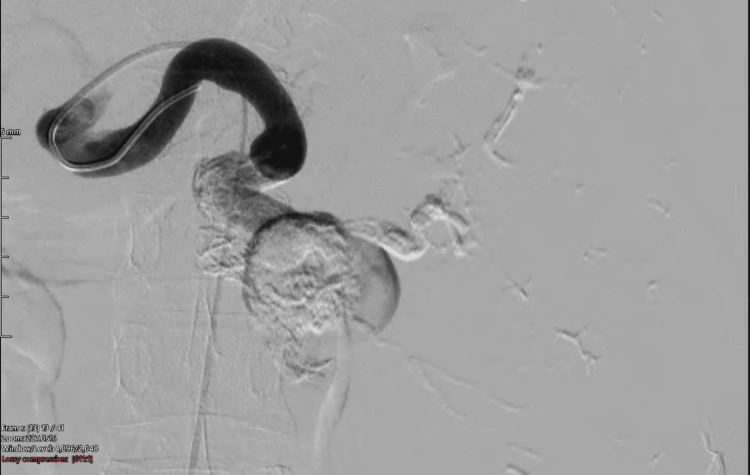 Figure 7
Figure 7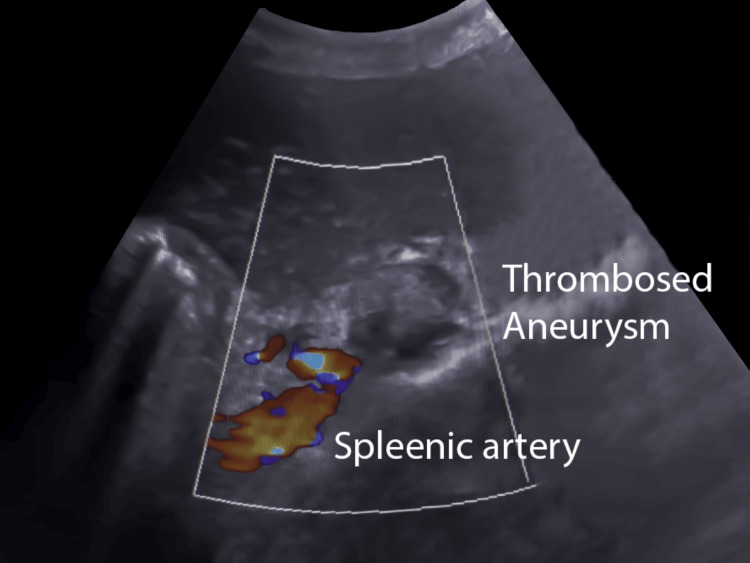 Figure 8
Figure 8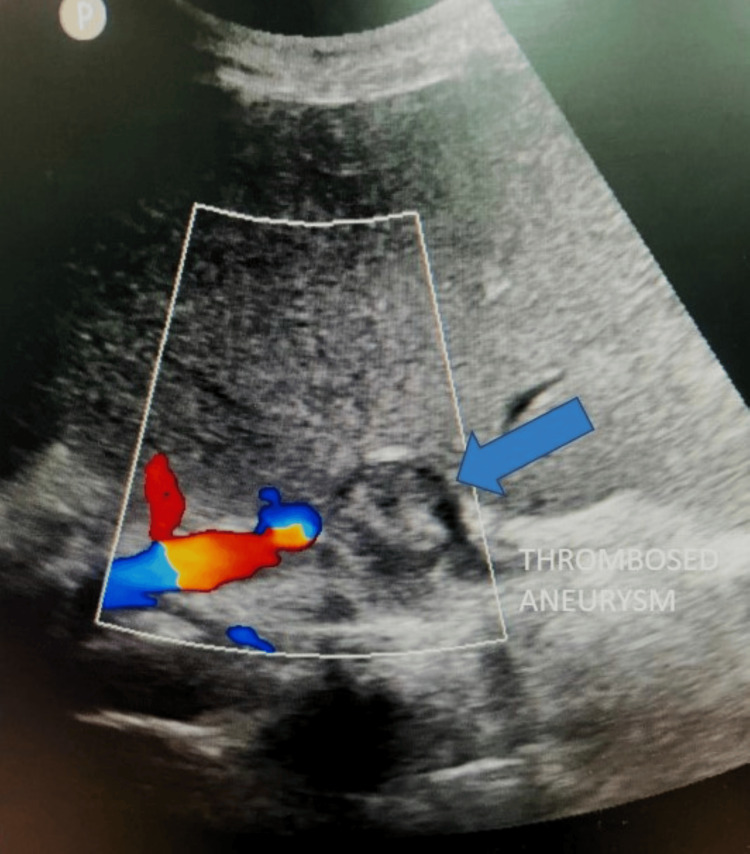 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Vascular Anomalies and Treatments · Renal and Vascular Pathologies
Introduction
Splenic artery pseudoaneurysms after aortoiliac aneurysms are the second most common abdominal aneurysms, constituting around 60% of all aneurysms [1,2]. Overall, 7% of individuals diagnosed with splenomegaly or portal hypertension exhibit a splenic artery aneurysm, while around 10% of those with a splenic artery aneurysm manifest symptoms of portal hypertension [3]. Conventional management comprises surgical simple ligation or resection of the aneurysm. Nevertheless, in recent years, endovascular techniques have been performed in growing numbers. Prior research focused on addressing endovascular therapies for splenic artery aneurysms has examined thrombin, coil embolization, gel foam detachable balloons, or a combination of these approaches [4,5]. Surgical resection of splenic artery aneurysm results in morbidity of roughly 1%-2% and mortality of 10% [6]. Here, we present the case of a patient managed with endovascular instillation of cyanoacrylate glue within the pseudoaneurysm sac.
Case presentation
A 40-year-old female was admitted to the hospital with chief complaints of hematochezia, abdominal pain, and melena for the past week. On examination, the patient had splenomegaly and tenderness in the epigastric region. The patient was vitally stable. She had reduced blood hemoglobin levels of 5.5 g/dL on lab investigation. The patient underwent a diagnostic ultrasound, which demonstrated splenomegaly and a pseudoaneurysm in the splenic artery (Figure 1).
Ultrasound of the spleen demonstrating the yin yang sign (yellow arrow) on color Doppler in the splenic artery, suggestive of a pseudoaneurysm.
An upper gastrointestinal endoscopy was performed on the subsequent day, and the patient had no significant ulcerations or bleeding from the upper gastrointestinal tract. The patient underwent a contrast-enhanced CT, which confirmed splenomegaly and pseudoaneurysm ultrasound findings along the splenic artery. The spleen measured 180 mm in the craniocaudal extent (Figure 2). The splenic artery pseudoaneurysm measured 43 × 32 mm (Figures 3, 4).
Coronal reformat of the non-contrast abdomen demonstrating splenomegaly.
Three-dimensional reformat of the abdomen at the level of the spleen shows an aneurysmal outpouching (green arrow) in the mid-splenic artery (red arrows).
Contrast-enhanced CT in the maximum intensity projection demonstrating an outpouching in the mid-splenic artery (orange arrow).
After a multidisciplinary meeting with the referring physician, radiologist, and interventional radiologist, the decision was made to pursue endovascular management using cyanoacrylate after vaccination with the Haemophilus influenza type b vaccine, pneumococcal vaccine, and meningococcal vaccine.
An angiography via the right femoral route using a 5 Fr cobra catheter was performed. The celiac artery was selectively cannulated, demonstrating an aneurysmal outpouching emanating from the middle portion of the splenic artery (Figure 5).
Angiography of the celiac trunk demonstrating an aneurysmal outpouching (red arrow) emanating from the mid portion of the splenic artery (blue arrow).
A 2.3 Fr microcatheter was coaxially introduced in the aneurysmal sac, and the pseudoaneurysm was embolized with 3 mL of 33% N-butyl cyanoacrylate glue mixed in lipiodol (Figure 6).
Fluoroscopic image demonstrating glue cast within the aneurysmal sac (red arrow). The microcatheter (green arrow) was introduced co-axially from the diagnostic catheter (blue arrow) into the aneurysm.
This concentration of glue and volume was based on the operator’s prior experience. The glue injection was performed using a 5 mL lewer lock syringe and controlled hand injection. Before the introduction of the glue within the microcatheter, the microcatheter system was meticulously prepared by flushing the catheter with roughly 5 mL of 5% dextrose, a non-ionic solution, to arrest impetuous contact of the cyanoacrylate glue concoction with ionic saline and blood and thus prevent untimely polymerization of glue enclosed in the microcatheter. After the aneurysm was completely filled with glue, the microcatheter was removed with a jerk from the diagnostic catheter. This was done to prevent the microcatheter from adhering to the glue cast inside the pseudoaneurysm. The cobra catheter was flushed with 10 mL of normal saline solution at least five times to prevent residual glue and thrombi from entering the bloodstream and causing non-target embolization. The post-embolization angiography demonstrated complete exclusion of the aneurysm (Figure 7).
Angiography of the splenic artery demonstrating complete exclusion of the aneurysm with glue cast in the aneurysmal sac.
In the intensive critical care unit, the patient was observed for 24 hours. The patient experienced abdominal pain and fever, which was managed conservatively with intravenous non-steroidal anti-inflammatory drugs. The patient was asymptomatic and discharged on the second day. Follow-up sonography on the second day of the procedure showed complete obliteration of the aneurysm, and there were no signs of splenic infarctions (Figure 8).
Ultrasound with color Doppler on the second day of the procedure showing complete thrombosis of the aneurysm.
The abdominal pain, hematochezia, and melena resolved within a day, and the patient was on follow-up. On her six-month follow-up, the patient’s hemoglobin level was 9 g/dL. The color Doppler of the aneurysm showed no vascularity. The spleen was heterogeneous, suggesting partial infarction and mild reduction in size compared to the preoperative ultrasound (Figure 9).
Ultrasound with color Doppler on the sixth-month follow-up showing complete thrombosis of the aneurysm with a reduction in the size of the aneurysm (blue arrow).
Discussion
Dotter and Goldman first described endovascular glue embolization with isobutyl 2-cyanoacrylate in treating upper gastrointestinal bleeding, pelvic hemorrhage, and selective renal artery occlusion [7,8]. Conventional management comprises surgical simple ligation or resection of the aneurysm. Endovascular management of splenic artery pseudoaneurysm with the use of stainless steel coils was first reported by Uflacker and Diehl [9]. Other procedures that have gained acceptance include embolization with micro-coils, laparoscopic surgery, and stent-graft technique [4,5,10,11]. In this case report, we discuss using cyanoacrylate glue to embolize splenic pseudoaneurysms. As the patient was unfit for surgery and the potential benefit of treating the entire diseased splenic artery and the expertise in handling cyanoacrylate glue by the interventional radiologist, the multidisciplinary team decided to proceed with endovascular management of this aneurysm. Coils and plugs were not used in our case as the objective was the exclusion of the pseudoaneurysm and not splenic infarction.
Cyanoacrylate glue rapidly polymerizes on contact with ionic solutions such as blood and saline, requiring the operator to have specialized training. The polymerization rate is adjusted with a change in the concentration of the ratio of cyanoacrylate and lipodol. The potential complication of an erroneous mixture may result in non-target proximal vascular or distal embolization. Non-target embolization can also occur with wrong injection rates. The other potential complications include abscess, rupture, septicemia, and pneumonia. This can be reduced with effective pain control, strict aseptic precautions, and careful post-embolization follow-up. Cyanoacrylate glue embolization can also treat hemobilia, visceral arteriovenous malformations, and neuro arteriovenous malformations [12]. Although most interventional radiologists are well-versed in using detachable balloons, coils, and particles such as polyvinyl alcohol and gelatin sponges, few have experience with liquid adhesives such as cyanoacrylate glue.
Conclusions
Cyanoacrylate glue embolization by the endovascular technique should be the management methodology of choice in the treatment of splenic artery aneurysms and is a viable alternative to surgery and detachable balloons, coils, and particles such as polyvinyl alcohol and gelatin sponges due to its potential benefit of treating the entire diseased splenic artery without resulting in splenic infarctions. All interventional radiologists should be well versed in the potential applications of and handling cyanoacrylate glue. The follow-up imaging and clinical improvement demonstrate the benefits of glue embolization in the case of an unruptured splenic artery aneurysm.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Splanchnic artery aneurysms Arch Surg Stanley JC Thompson NW Fry WJ 6896971011970548929310.1001/archsurg.1970.01340300045009 · doi ↗ · pubmed ↗
- 2Splenic artery aneurysm in the 1990 s Ann Vasc Surg Dave SP Reis ED Hossain A Taub PJ Kerstein MD Hollier LH 2232291420001079695310.1007/s 100169910039 · doi ↗ · pubmed ↗
- 3Common splanchnic artery aneurysms: splenic, hepatic, and celiac Ann Vasc Surg Shanley CJ Shah NL Messina LM 315322101996879300310.1007/BF 02001900 · doi ↗ · pubmed ↗
- 4Treatment of multiple aneurysms of the splenic artery after liver transplantation by percutaneous embolization and laparoscopic splenectomy Transplantation De Roover A Sudan D 9569587220011157146610.1097/00007890-200109150-00036 · doi ↗ · pubmed ↗
- 5Endovascular management of splenic artery aneurysms and pseudoaneurysms Cardiovasc Intervent Radiol Mc Dermott VG Shlansky-Goldberg R Cope C 179184171994795457010.1007/BF 00571531 · doi ↗ · pubmed ↗
- 6Splenic artery aneurysms World J Surg Trastek VF Pairolero PC Bernatz PE 37838391985401335210.1007/BF 01655271 · doi ↗ · pubmed ↗
- 7[Embolization of AVM's of thoracic spinal cord with histoacryl glue]Neurol Neurochir Pol Radek A Maciejczak A Zajgner J 333345301996 https://pubmed.ncbi.nlm.nih.gov/8756259/8756259 · pubmed ↗
- 8Endovascular glue embolisation of intercostal arteriovenous fistula: a non-surgical treatment option J Postgrad Med Siddhartha W Parmar H Shrivastav M Limaye U 213214462000 https://pubmed.ncbi.nlm.nih.gov/11298475/11298475 · pubmed ↗