Diagnosis of Kallmann Syndrome in a Young Adult Male
Kushal Bothara, Purnachandra Lamghare, Eshan Chetan Durgi, Karishma Krishnani

TL;DR
A young man with anosmia and delayed sexual development was diagnosed with Kallmann syndrome using MRI and ultrasound.
Contribution
This case highlights the importance of MRI in confirming Kallmann syndrome through the detection of absent olfactory bulbs.
Findings
MRI revealed absent olfactory bulbs and hypoplastic olfactory sulci.
Ultrasound showed atrophic testes consistent with Kallmann syndrome.
The anterior pituitary was normal on MRI, supporting the diagnosis.
Abstract
Kallmann syndrome is an anosmic variety of GnRH (gonadotropin-releasing hormone) deficiency. A young adult male with anosmia since childhood presented with features of failed sexual maturation and underwent an ultrasound of the genital system and an MRI (magnetic resonance imaging) of the brain. MRI revealed absent olfactory bulbs in bilateral olfactory grooves with hypoplastic olfactory sulci on both sides. Ultrasound showed atrophic testes, while the anterior pituitary appeared normal on MRI. The clinical, hormonal, and imaging findings were characteristic of Kallmann syndrome. MRI serves as a crucial tool in its diagnosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1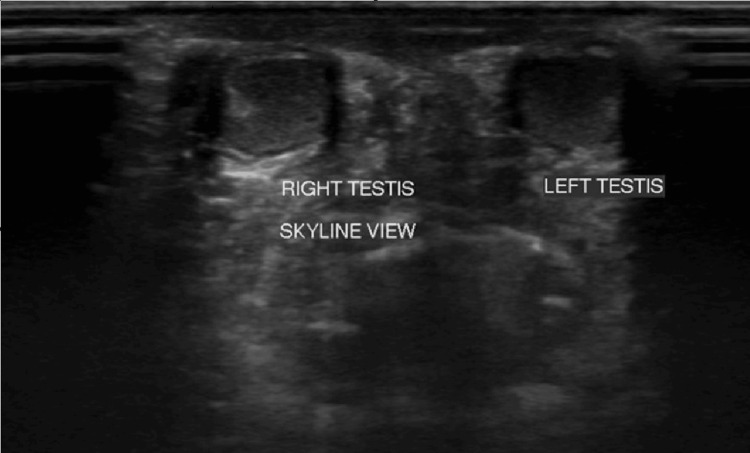 Figure 2
Figure 2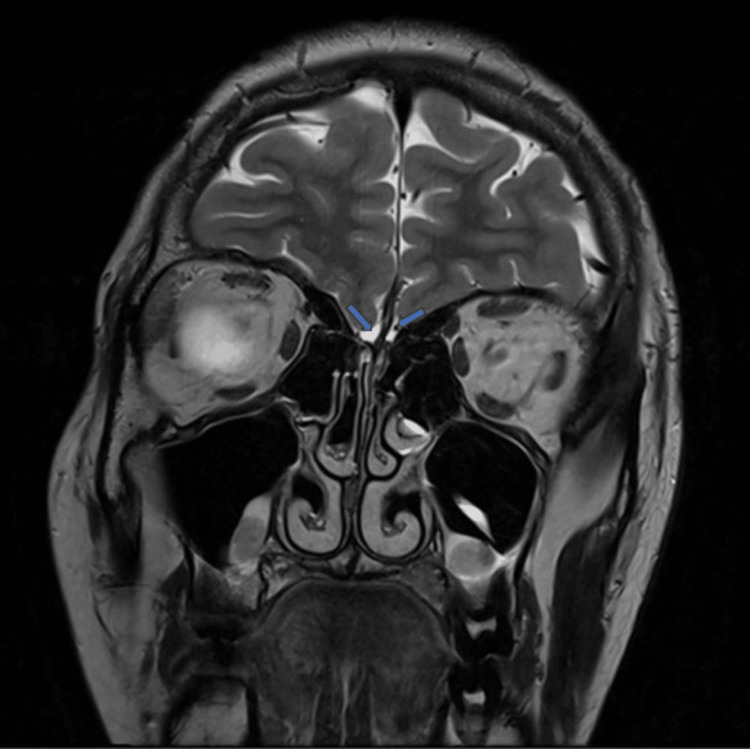 Figure 3
Figure 3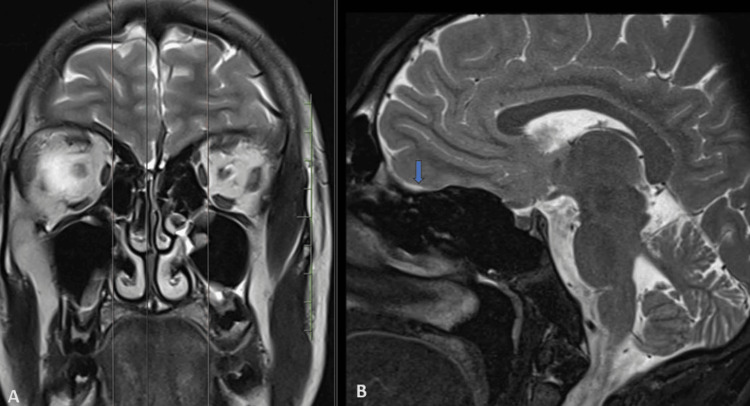 Figure 4
Figure 4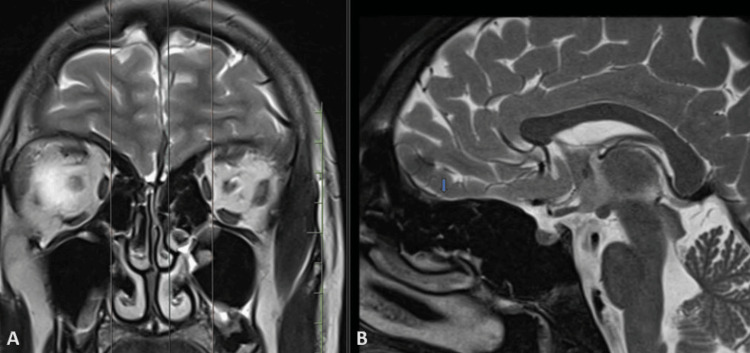 Figure 5
Figure 5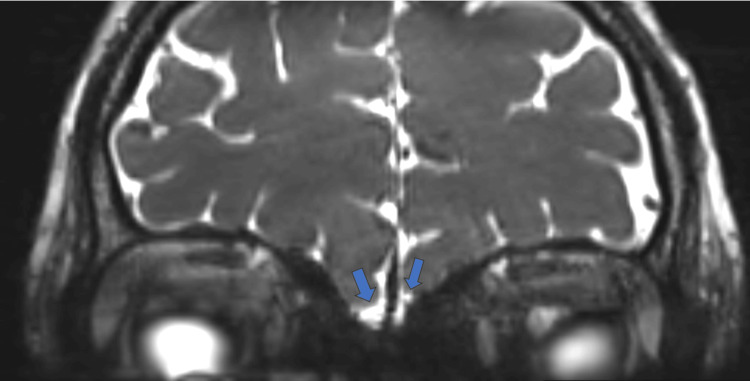 Figure 6
Figure 6| Test | Observed value | Reference range |
| FSH | 0.46 mIU/ml | 1.40–15.40 mIU/ml |
| LH | 0.10 mIU/ml | 0.56–12.07 mIU/ml |
| Testosterone level | 9.76 ng/dl | 300–950 ng/dl |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHypothalamic control of reproductive hormones · Ovarian function and disorders · Genetic and Clinical Aspects of Sex Determination and Chromosomal Abnormalities
Introduction
Kallmann syndrome is an anosmic variety of (gonadotropin-releasing hormone) GnRH deficiency [1]. It usually results from mutations involving one or more genes involved in olfactory bulb morphogenesis and the subsequent migration of GnRH neurons from their site of origin to their final location. It is an X-linked disorder, more common in males [2], resulting in GnRH deficiency. Diagnosis is based on a combination of clinical findings, hormonal evaluation, and imaging findings.
Case presentation
A 20-year-old male presented with complaints of failed sexual maturation and anosmia since childhood. He also reported decreased hearing in his left ear. No other associated medical issues were noted, and there was no history of similar complaints in his family. The patient has two siblings - a brother and a sister - with normal sexual maturity. Upon arrival at our hospital, the patient underwent an MRI of the brain, an ultrasound of the abdomen and pelvis, and hormonal assays.
Clinical examination initially revealed hormonal abnormalities, including absent secondary sexual characteristics, micropenis, a high-pitched voice, and decreased pubic, axillary, and facial hair (Figure 1).
The clinical image demonstrating micro-penis.
On ultrasonography, normal functioning bilateral kidneys were observed, with a renal calculus noted in the right kidney. In inguino-scrotal ultrasonography, both testes appeared smaller in size, with the right testis measuring approximately 0.32 cc and the left testis measuring approximately 0.27 cc. Normal testis volume typically ranges from 12 to 30 cc. Therefore, in this case, the findings suggested testicular atrophy. Importantly, both testes were observed within the scrotal sac, ruling out cryptorchidism (Figure 2).
Ultrasound image showing skyline view showing both the atrophic testes.
The patient underwent an MRI, which revealed the absence of olfactory bulbs in bilateral olfactory grooves and bilateral hypoplastic olfactory sulci (Figures 3-6).
Coronal T2-weighted MRI shows absent olfactory bulbs in bilateral olfactory grooves with hypoplastic olfactory sulci on both sides (blue arrows).
T2-weighted MRI in coronal section (A) with sagittal section (B) at corresponding level show absent olfactory bulb in right olfactory groove with hypoplastic olfactory sulcus (blue arrow).
Coronal T2-weighted MRI in coronal (A) section with sagittal section (B) at corresponding level show absent olfactory bulb in left olfactory groove with hypoplastic olfactory sulcus (blue arrow).
CISS (constructive interference in steady state) MRI sequence showing absent olfactory bulbs (blue arrows).
With these examination findings, the patient underwent further hormonal assays. Table 1 displays the results of the hormonal assay, indicating reduced levels of follicle-stimulating hormone (FSH), luteinizing hormone (LH), and testosterone compared to the reference ranges.
Based on the above findings, the patient was diagnosed with Kallmann syndrome. Hormonal replacement therapy was initiated, along with the supplementation of vitamin D and bisphosphonates for lifelong management. Surgical intervention was not required. Interval follow-ups with hormonal assays were recommended for monitoring.
Discussion
Congenital GnRH deficiency can be anosmic or normosmic [3]. Kallmann syndrome is an anosmic variety of GnRH deficiency [1]. It usually results from mutations involving one or more genes involved in olfactory bulb morphogenesis and the subsequent migration of GnRH neurons from their site of origin (in the olfactory placode) into their final location (the pre-optic region of the hypothalamus) [1].
This leads to a deficiency of GnRH, with a resultant deficiency of LH and FSH. LH and FSH are hormones that stimulate the testes, and a reduction in their secretion results in secondary hypogonadism. Hence, this leads to a setting where there is a deficiency of LH, FSH and testosterone.
Kallmann syndrome is known to be associated with mutations in KAL1, genes involved in fibroblast growth factor (FGF) signaling, NELF, genes involved in PROK signaling, WDR11, SEMA3, HS6ST1, CHD7, and FEZF1 [3].
Kallmann syndrome usually involves hypogonadotropic hypogonadism alongside a total lack of the ability to smell (anosmia) [4]. In the present case, the patient has complained of anosmia since childhood. When anosmia is not present, it is commonly known as idiopathic hypogonadotropic hypogonadism (IHH).
Zaghouani et al. [2], in their study of five patients with Kallmann syndrome, reported that all patients had absent olfactory bulbs, with three of them showing absent olfactory sulci and two of them having hypoplastic olfactory sulci. Our case also had absent olfactory bulbs with bilateral hypoplastic olfactory sulci (Figure 3).
Koenigkam-Santos et al. [5] reported that patients with Kallmann syndrome frequently had findings of olfactory bulbs and sulcus aplasia. Specifically, findings of bulb aplasia on MRI in the clinical setting of aplasia were highlighted, which aligns with our own observations in this case. Sometimes, a hypoplastic anterior pituitary may also be seen; however, in the present case, the anterior pituitary was normal.
MRI is the investigation of choice for evaluating olfactory bulb aplasia. The widespread use of MRI in modern medicine has significantly enhanced the radiological assessment of olfactory disorders. The groundbreaking studies by Yousem et al. [6] showcased MRI's capability to provide precise volumetric measurements of the olfactory bulb across different pathological conditions. It allows for detailed imaging of the olfactory bulb and tract, making it highly effective at detecting even subtle damage to the central projection areas involved in the sense of smell.
For the best visualization of the olfactory bulbs, a coronal scan with a large matrix size and minimized intersection gap is advised. This imaging plane is particularly suited for comprehensive anatomical assessment of the olfactory tract, detection of parenchymal lesions, and accurate volumetric measurement of the olfactory bulbs [7]. Axial MRI images allow for the visualization of the olfactory sulci in the frontal lobes; however, they are not ideal for assessing the olfactory bulbs or tracts, which are more clearly seen in coronal views [8].
Kallmann syndrome is known to be associated with renal anomalies, cleft lip/palate, tooth anomalies, pigmentation, cranio-facial anomalies, oculomotor/visuospatial defects, and gut malformations [3]. In the present case, there was no evidence of any cranial or extracranial anomalies.
Kallmann syndrome is usually suspected based on clinical features (delayed puberty) and confirmed using hormonal and imaging findings, such as decreased levels of GnRH, LH, FSH, and testosterone and absence or hypoplasia of the olfactory bulb and sulci.
Conclusions
Kallmann syndrome is initially suspected based on clinical features such as delayed puberty and is confirmed using hormonal assays and radiological investigations (MRI). Ultrasound is crucial for ruling out associated anomalies, which include renal anomalies and cryptorchidism, and detecting testicular atrophy, as observed in the present case. MRI plays a pivotal role in assessing the olfactory bulbs and ruling out acquired causes of hypogonadism, such as sellar masses or infiltrative diseases of the hypothalamus or pituitary gland. Therefore, MRI plays a significant role in both diagnosing and managing rare genetic disorders like Kallmann syndrome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kallman syndrome versus idiopathic hypogonadotropic hypogonadism at MR imaging Radiology Vogl TJ Stemmler J Heye B 53571911994813459710.1148/radiology.191.1.8134597 · doi ↗ · pubmed ↗
- 2Kallmann syndrome: MRI findings Indian J Endocrinol Metab Zaghouani H Slim I Zina NB Mallat N Tajouri H Kraiem C 0517201310.4103/2230-8210.119536 PMC 383028324251137 · doi ↗ · pubmed ↗
- 3Disorders of sex development Harrison’s Principles of Internal Medicine Achermann JC Jameson J 27762777 New York Mc Graw-Hill Education 2018 https://accessmedicine.mhmedical.com/book.aspx?bookid=3095&is Missing Chapter=true
- 4Kallmann syndrome Eur J Hum Genet DodéC Hardelin JP 1391461720091898507010.1038/ejhg.2008.206PMC 2986064 · doi ↗ · pubmed ↗
- 5Quantitative magnetic resonance imaging evaluation of the olfactory system in Kallmann syndrome: correlation with a clinical smell test Neuroendocrinology Koenigkam-Santos M Santos AC Versiani BR Diniz PR Junior JE de Castro M 2092179420112160664210.1159/000328437 · doi ↗ · pubmed ↗
- 6Kallmann syndrome: MR evaluation of olfactory system AJNR Yousem DM Turner WJ Li C Snyder PJ Doty RL 839843141993 https://www.ajnr.org/content/14/4/8398352154 PMC 8333839 · pubmed ↗
- 7Kallmann syndrome: MR findings AJNR Knorr JR Ragland RL Brown RS Gelber N 845851141993 https://www.ajnr.org/content/14/4/845.short 8352155 PMC 8333846 · pubmed ↗
- 8Neuroradiology of Kallmann's syndrome Acta Med Port de m Freitas P Carvalho S Ribeiro F Marnoto D Martins F 123126142001 https://europepmc.org/article/med/1132196711321967 · pubmed ↗