Effect of topical Zingiber cassumunar on painful diabetic neuropathy: a double-blind randomized-controlled trial
Nachapol Jatuten, Phuangthong Piyakunmala, Jiratha Budkaew, Bandit Chumworathayi, Fifteen Aprila Fajrin, Bandit Chumworathayi

TL;DR
A study found that a balm made from Zingiber cassumunar (Plai) reduced pain in people with diabetic neuropathy more effectively than a placebo.
Contribution
This is the first double-blind RCT to demonstrate the efficacy of topical Zingiber cassumunar in reducing pain in diabetic neuropathy.
Findings
Plai balm reduced mean pain scores significantly more than placebo at week two and week four.
75% of the Plai group had at least 50% pain reduction compared to 20% in the placebo group.
No adverse events were observed in either group.
Abstract
Background: Plai or Zingiber cassumunar Roxb. was registered into the Thai Traditional Medicine list since 2011. However, there is limited evidence regarding Plai as a treatment in painful diabetic neuropathy (PDN). Therefore, this study aimed to evaluate the efficacy of topical Zingiber cassumunar. Methods: A RCT was conducted in patients with PDN during February to March 2019. All participants received oral gabapentin 300 mg before bed as a standard regimen. The intervention group (n=16) received Plai balm 15%w/w 0.5 gram to apply on their feet three times a day and the control group (n=15) received placebo balm to similarly apply. Pain score at baseline, 2 nd and 4 th weeks were assessed and compared. Patients’ quality of life, and adverse events, were collected. Mean pain scores before and after treatment in each group and between groups were also analyzed. Results: At the end of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
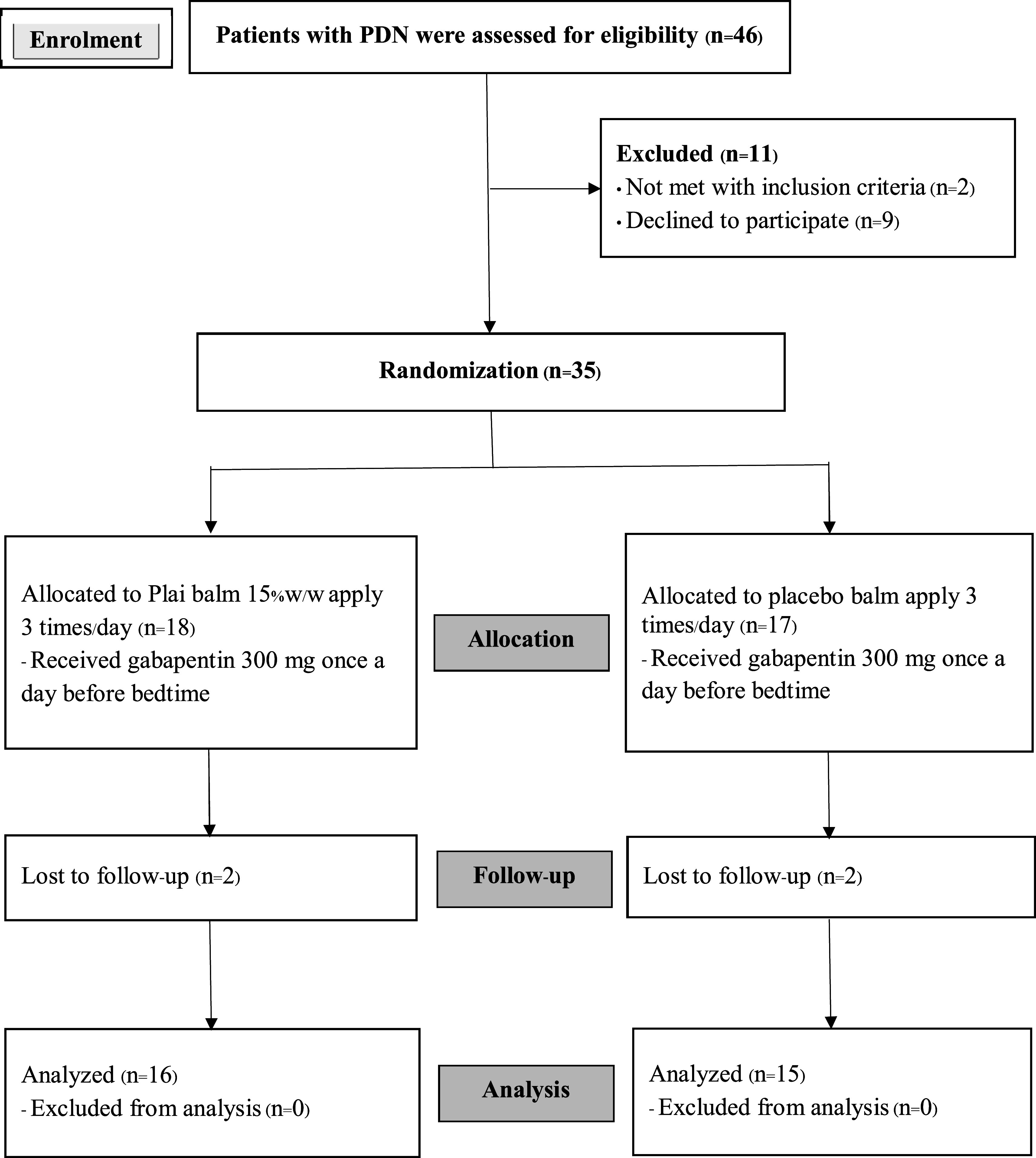 Figure 1
Figure 1| Patients’ characteristics | Plai (n=16) | Placebo (n=15) | P-value | ||
|---|---|---|---|---|---|
| Number | Percent | Number | Percent | ||
|
| 0.064 | ||||
| Lower than 50 | 2 | 12.50 | 4 | 26.67 | |
| 51 or more | 14 | 87.50 | 11 | 73.33 | |
| Mean (±SD) | 55.56 | (±5.43) | 52.87 | (±5.57) | |
| Median (min:max) | 58 | (39:59) | 54 | (39:59) | |
|
| 0.561 | ||||
| Male | 7 | 43.75 | 6 | 40.00 | |
| Female | 9 | 56.25 | 9 | 60.00 | |
|
| 0.611 | ||||
| Lower than 5 | 6 | 37.50 | 4 | 26.67 | |
| 6 or more | 10 | 62.50 | 11 | 73.33 | |
| Mean (±SD) | 7.50 | (±3.29) | 8.07 | (±2.81) | |
| Median (min:max) | 6.50 | (3:12) | 8.00 | (4:12) | |
|
| 0.662 | ||||
| Lower than 1 | 8 | 50.0 | 8 | 53.33 | |
| 2 or more | 8 | 50.0 | 7 | 46.67 | |
| Mean (±SD) | 1.88 | (±1.31) | 1.67 | (±1.05) | |
| Median (min:max) | 1.5 | (1:6) | 8.00 | (1:5) | |
|
| 0.561 | ||||
| Yes | 9 | 56.25 | 9 | 60.00 | |
| No | 7 | 43.75 | 6 | 40.00 | |
|
| 0.534 | ||||
| Mean (±SD) | 11.09 | (±2.14) | 10.59 | (±2.22) | |
| Median (min:max) | 10.9 | (8.3:16.6) | 8.00 | (7:15.1) | |
|
| 0.280 | ||||
| Mean (±SD) | 6.81 | (±1.47) | 6.33 | (±1.59) | |
| Median (min:max) | 6.5 | (5:10) | 6 | (5:9) | |
|
| 0.525 | ||||
| Yes | 2 | 12.50 | 1 | 6.67 | |
| No | 14 | 87.50 | 14 | 93.33 | |
|
| 0.475 | ||||
| Yes | 1 | 6.25 | 2 | 13.33 | |
| No | 15 | 93.75 | 13 | 86.67 | |
| Pain characteristics | Plai (n=16) | Placebo (n=15) | ||
|---|---|---|---|---|
| Frequency | Intensity | Frequency | Intensity | |
| (Percent) | (Mean±SD) | (Percent) | (Mean±SD) | |
| 1. Throbbing | 6 (37.5) | 1.44±0.55 | 11 (73.33) | 1.45±0.52 |
| 2. Shooting | 12 (75) | 1.92±0.79 | 12 (80.0) | 1.33±0.49 |
| 3. Stabbing | 10 (62.5) | 1.70±0.67 | 4 (26.67) | 1.75±0.5 |
| 4. Sharp | 12 (75) | 2±0.60 | 11 (73.33) | 1.36±0.50 |
| 5. Cramping | 4 (25) | 2±0.81 | 5 (33.33) | 2±0.71 |
| 6. Gnawing | 6 (37.5) | 1.83±0.98 | 6 (40.0) | 1±0 |
| 7. Burning | 7 (43.75) | 1.86±0.38 | 11 (73.33) | 1.45±0.68 |
| 8. Aching | 7 (43.75) | 1.43± 0.53 | 4 (26.67) | 1.45±0.53 |
| 9. Heavy | 5 (31.25) | 1.6±0.55 | 4 (26.67) | 2±0.81 |
| 10. Tender | 3 (18.75) | 1.67±0.58 | 7 (46.67) | 2.75±0.5 |
| 11. Splitting | 2 (12.50) | 1.5±0.7 | 2 (13.33) | 2.5±0.71 |
| 12. Exhausting | 10 (62.5) | 1.7±0.67 | 6 (40.0) | 1.83±0.75 |
| 13. Fearful | 6 (37.5) | 1.83±0.75 | 3 (20.0) | 2±1 |
| 14. Sickening | 15 (93.75) | 1.73±0.59 | 14 (93.33) | 1.57±0.85 |
| 15. Punishing-Cruel | 13 (81.25) | 1.54±0.66 | 12 (80.0) | 1.5±0.79 |
| Pain mappings | Plai (n=16) | Placebo (n=15) | ||
|---|---|---|---|---|
| Number | Percent | Number | Percent | |
| Posterior ankle pain | 12 | 75.00 | 12 | 80.00 |
| Lateral ankle pain | 12 | 75.00 | 12 | 80.00 |
| Medial ankle pain | 10 | 62.50 | 10 | 66.67 |
| Anterior ankle pain | 10 | 62.50 | 10 | 66.67 |
| Dorsal forefoot pain | 16 | 100.00 | 15 | 100.00 |
| Dorsal great toe pain | 16 | 100.00 | 15 | 100.00 |
| Dorsal lesser toe pain | 16 | 100.00 | 15 | 100.00 |
| Metatarsal head pain | 13 | 81.25 | 15 | 100.00 |
| Plantar great toe pain | 16 | 100.00 | 15 | 100.00 |
| Plantar lesser toe pain | 12 | 75.00 | 14 | 93.33 |
| Plantar midfoot pain | 16 | 100.00 | 15 | 100.00 |
| Heel pain | 16 | 100.00 | 15 | 100.00 |
| Groups | Baseline Mean (SD) | Week 2 Mean (SD) | Week 4 Mean (SD) | Week 2 | Week 4 | ||
|---|---|---|---|---|---|---|---|
| Mean change
| P-value | Mean change
| P-value | ||||
|
| 6.81 (1.47) | 3.81 (1.04) | 3.38 (1.02) | -3.00 (-3.58 to -2.41) | <0.001 | -3.44 (-3.87 to -3.00) | <0.001 |
|
| 6.33 (1.59) | 4.8 (1.57) | 4.4 (1.40) | -1.53 (-2.08 to -0.98) | <0.001 | -1.93 (-2.46 to -1.40) | <0.001 |
| NRS differences | Week 2 | Week 4 | ||||
|---|---|---|---|---|---|---|
| Plai (n=16) | Placebo (n=15) | P-value | Plai (n=16) | Placebo (n=15) | P-value | |
|
| -1.47 (-1.96 to -1.30) | 0.001 | -1.51 (-1.92 to -0.13) | 0.027 | ||
| Pain reduction amount | Groups | P-value | |
|---|---|---|---|
| Plai, n (%) | Placebo, n (%) | ||
|
| 12 (75.00) | 3 (20.00) | 0.004 |
| <
| 4 (25.00) | 12 (80.00) | |
| WHOQOL-BREF domain |
| SD | Mean difference | 95%CI | P-value |
|---|---|---|---|---|---|
|
| |||||
| Plai | 14.12 | 0.60 | -1.74 | -3.49 to 0.01 | 0.0504 |
| Placebo | 15.87 | 0.60 | |||
|
| |||||
| Plai | 20.56 | 0.96 | -0.30 | -3.21 to 2.60 | 0.832 |
| Placebo | 20.86 | 1.05 | |||
|
| |||||
| Plai | 10.875 | 0.24 | -0.32 | -0.99 to 0.34 | 0.329 |
| Placebo | 11.2 | 0.22 | |||
|
| |||||
| Plai | 26.25 | 0.61 | 0.52 | -1.25 to 2.28 | 0.555 |
| Placebo | 25.73 | 0.61 | |||
|
| |||||
| Plai | 71.81 | 1.48 | -1.85 | -5.98 to 2.28 | 0.366 |
| Placebo | 73.67 | 1.37 | |||
- —Khon Kaen Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPain Mechanisms and Treatments · Ginger and Zingiberaceae research · Pharmacological Effects of Natural Compounds
Introduction
Diabetic polyneuropathy is one of the complications of diabetes mellitus. There are many signs and symptoms, such as painful diabetic neuropathy (PDN), orthostatic hypotension, cardiac autonomic neuropathy, foot injuries, and wounds. ^ 1 ^ The incidence of diabetic patients who have developed neuropathy, is approximately 20%. In addition, 50-70% of them must undergo surgery for non-traumatic amputation. ^ 2 ^
PDN is the damage of nerves, that causes pain in the limbs. Patients will suffer from aching and feeling like shooting and stabbing pain. These symptoms will occur at the limbs during nighttime, and usually affect daily life activities, sleeping patterns and work, as a result, patient quality of life will be decreased. ^ 3 ^ ^,^ ^ 4 ^
Presently, non-steroidal analgesic medicines or opioids have been widely used for symptoms relieving. However, opioids are not only ineffective but have many side effects when treating PDN. Consequently, patients’ quality of life also decreases because of drug’s dosage-administration complexities, and long onset of action. ^ 5 ^ ^–^ ^ 8 ^ Capsaicin cream is effectively used for pain relief in PDN, but after a week, it might cause severe burn effect and finally require opioids for pain relief. ^ 9 ^
Plai or Zingiber cassumunar Roxb. is registered on the Thai Traditional Medicine list since 2011, ^ 10 ^ and categorized as a topical anti-inflammatory agent. The important extracted components from Zingiber cassumunar are (E)-4-(3, 4–dimethoxyphenyl) but-3-en-1-ol (compound D), (E)-1-(3, 4-dimethoxyphenyl) but-1, 3-diene (DMPBD) and zerumbone. ^ 11 ^ It has also been used for anti-inflammation, ^ 12 ^ ^–^ ^ 15 ^ pain relief, ^ 16 ^ ^–^ ^ 19 ^ and local anesthesia. ^ 20 ^ ^–^ ^ 23 ^
Although there were two successful studies of mixed multi-herbal preparation using Zingiber cassumunar Roxb. as its main component in treating diabetic foot ulcers, ^ 24 ^ ^,^ ^ 25 ^ there still has been no study regarding the use of Plai as a treatment in PDN. Therefore, this study aimed to evaluate the efficacy of a topical Zingiber cassumunar preparation by comparing with placebo on PDN.
Methods
Patients
This study was conducted at Selaphum Hospital, Selaphum District, Roi Et, Thailand. Participants were patients diagnosed with PDN. Neuropathic Pain Diagnostic Questionnaire (Thai version of DN4) was used for pain assessment, ^ 26 ^ and monofilament test was used as a sensory screening tool in these patients. ^ 8 ^ Written informed consent was obtained from all patients.
Recruitment
Patients aged 20-60 years who had been diagnosed with diabetic mellitus for at least 1 year, tested for HbA1c within six months, suffering from pain intensity on a scale as moderate or more [Numerical Rating Scale (NRS), pain score ≥ 4], and with defined positive monofilament test result, were included. Patients who had been diagnosed with diabetic mellitus less than one year, with other caused neuropathy, clinically significant cardiovascular, foot ulcer and/or infection, pregnancy and lactation, and allergy to Plai, were excluded.
Study design and oversight
This double-blind randomized-controlled trial was conducted within four weeks, from the 1 ^st^ of February to the 1 ^st^ of March 2019. All the authors were involved in the design and performance of the study, which was conducted according to the Declaration of Helsinki. The Khon Kaen Hospital Institute Review Board (KKHIRB) in Human Research (the oversighting IRB for Selaphum Hospital) approved the study protocol on 19 ^th^ December 2018 (KE61099). This trial was retrospectively registered with the Thai Clinical Trial Registry (TCTR20200221001) on 19 ^th^ February 2020, because “registration before recruitment” was missed, but authors finally registered it within one year after completion. Registration before recruitment is not a prerequisite for KKHIRB or Selaphum Hospital’s study. The study protocol did not differ from the registered one.
Study treatment and procedures
Pain assessment was commenced at week 0 and indicated by using The World Health Organization Quality of Life (WHOQOL-BREF–THAI) ^ 27 ^ with NRS, pain characteristic, and pain mapping to follow-up side effect of Plai and its adverse events as baseline. Consequently, patients returned to clinic at the following week one, two, and four, to monitor and assess the accuracy of practice on frequency, and dosage of balms’ use. The patients’ quality of life in week 4 were observed and recorded.
Block-of-four randomization was applied to this study, concealment was done by telephone calls to research assistants. Participants were divided into two groups. All participants received oral gabapentin of 300 mg, one tablet a day before bedtime as a standard regimen. The intervention group (n=16) received Plai balm 15% w/w 0.5 gram to apply on their feet three times a day and the control group (n=15) received the placebo balm to apply similarly.
Endpoints
The mean differences of pain scores in NRS at week two and four between the two groups were the first endpoint. The other endpoint was the comparison of patients’ numbers/percentages who have at least 50% pain reduction at week two and four between the groups. Additionally, The World Health Organization Quality of Life (WHOQOL- BREF–THAI) scores changes at week four were compared between the groups.
Statistical analysis
The preliminary study suggests that the number of participants should be 24-36 people. Consequently, this study recruited 35 participants, which were divided in to two groups. Generalized estimating equation (GEE) was used to analyze the mean differences of pain scores at week two and four. Fisher’s exact test was used to analyze the differences in patients’ numbers/percentages who had at least 50% pain reduction at week two and four between the groups. Independent t-test was used to analyze the differences of The World Health Organization Quality of Life (WHOQOL-BREF–THAI) scores changes at week four between the groups. Mann-Whitney U-test was used to compare skew continuous data.
Results
Study patients
There were 826 diabetic mellitus type 2 patients treated at Selaphum Hospital during the study period. Although 88 of them had developed PDN, only 46 patients were able to participate according to the age criteria. Eleven of them were later excluded by other exclusion criteria. As a result, 35 of them were randomly assigned to each group. The intervention group had 18 participants receiving Plai balm, and the control group had 17 participants receiving placebo balm. Two participants in each group were later excluded due to follow-up loss ( Figure 1).
CONSORT flow diagram.
The patients’ characteristics, pain characteristics, and pain mapping of PDN at baseline, were similar among the two groups ( Tables 1, 1.1, and 1.2).
Primary outcomes
The mean changes of pain scores in each group were significantly decreased. The mean changes of pain score in the Plai group decreased by -3.00 (95%CI: -3.58 to -2.41, p-value <0.001) at week two, and by -3.44 (95%CI: -3.87 to -3.00, p-value <0.001) at week four. The mean changes of pain score in the placebo group also decreased by -1.53 (-95%CI: 2.08 to -0.98, p-value <0.001) at week two, and by -1.93 (95%CI: -2.46 to -1.40, p-value <0.001) at week four ( Table 2).
Using GEE analyses by controlling confounding factors (age, sex, quality of life score), showed that the Plai group had statistically significant less pain at week two by -1.47 (95%CI: -1.96 to -1.30, p-value <0.001) when compared to the placebo group. At week four, the Plai group’s pain score was still decreasing and statistically significant less than the placebo group by -1.51 (95%CI: -1.92 to -0.13, p-value <0.027) ( Table 2.1).
Secondary outcomes
Numbers/percentages of patients who had at least 50% pain reduction of pain by NRS scores at week four were found significantly more in the Plai group when compared to the placebo group [12/16 (75%) vs 3/15 (20%), p-value = 0.004] ( Table 3).
The overall integration of WHOQOL- BREF–THAI 4 components was used. Physical domain, psychological domain, social relationships, and environmental domain analyzed patients’ quality of life scores at week four. Overall and each domain’s patients’ quality of life scores were no different between the two groups ( Table 4).
Adverse events
No adverse events such as edema, erythema, papules, pruritus, and burning sensation, were found in this study.
Discussion
This double-blind randomized-controlled trial was conducted in PDN patients who had pain by NRS scores of four or more within four weeks, from the 1 ^st^ February to the 1 ^st^ March 2019 at Selaphum Hospital, Selaphum District, Roi Et, Thailand. Majority of participants were elderly female patients who had been diagnosed with poor controlled type 2 diabetic mellitus for years. Those patients met the criteria of having PDN, which obviously presented similar pain characteristics and pain mapping between the groups.
Based on this study’s method, all participants received oral gabapentin 300 mg, 1 tablet daily before bed as a standard regimen. The use of Plai balm 15% w/w 0.5 gram significantly showed pain reduction on PDN. The pain scores by NRS were decreased more in the Plai group compared to the placebo group [by mean differences of -1.47 (95%CI: -1.96 to -1.30, p-value <0.001) at week two, and by mean difference of -1.51 (95%CI: -1.92 to -0.13, p-value = 0.027) at week four]. These results derived from the effects of Plai balm on PDN.
Until now (December 2022), there has been no other trial that studied the efficacy of Plai on reducing pain in PDN. However, previous studies had shown that Plai being main component in mixed herbal preparations, is safe ^ 24 ^ and effective ^ 25 ^ in treating diabetic foot ulcers. Moreover, Plai has local anesthetic ^ 20 ^ ^–^ ^ 23 ^ and neuroprotective ^ 28 ^ effects, in addition to its effects on anti-inflammation ^ 12 ^ ^–^ ^ 15 ^ and pain relief. ^ 16 ^ ^–^ ^ 19 ^ These mechanisms in combination, might be the cause of pain reduction. Nevertheless, this study has been the first one to show the effect on PDN. Whether a neuroprotective effect also occurs in the peripheral nerves, is needed to be investigated.
In this study, not only Plai was found to be effective in pain reduction, but also safe with no adverse event reported, neither redness, swelling, burning or rash. These were similar to a systematic review done in 2017 by Chongmelaxme et al. ^ 15 ^ Even in two more recent studies, with very similar application but more mixed herbs, adverse events were still not found. ^ 24 ^ ^,^ ^ 25 ^ However, quality of life scores were not significantly different between groups at week 4, even though the quality-of-life scores were improved in each groups. This could be explained by the standard treatment both groups had received: 300 mg gabapentin, once a day. This might be also the main reason for similar changes in the quality-of-life scores.
Strengths of this study were 1) This has been the first RCT comparing treatment efficacy of Plai to placebo, 2) Pain reduction was found significantly different between the groups, and 3) Pain and quality of life scores were measured, reported, and analyzed using their standard methods. Weaknesses of this study might be that; 1) It has low sample size, 2) Some patients were lost from each group, and 3) Cost-effectiveness was not collected and analyzed. Future research with similar objectives may be conducted with larger sample sizes and more diverse settings.
Conclusion
In conclusion, Zingiber cassumunar balm (Plai) was efficacious and safe for reducing pain in patients with painful diabetic neuropathy (PDN). However, quality of life scores changes in the Plai group were not significantly different from the placebo group.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tesfaye S Selvarajah D : The Eurodiab study: what has this taught us about diabetic peripheral neuropathy? Curr. Diab. Rep. 2009;9:432–434. 10.1007/s 11892-009-0070-1 19954687 · doi ↗ · pubmed ↗
- 2Hadden RDM Thomas PK Hughes RAC : Diseases of the peripheral nerves. Warrell DA Cox TM Firth JD , editors. Oxford Textbook of Medicine. 5 ed. Oxford: Oxford Textbooks;2010.
- 3Centre for Clinical Practice at NICE (UK): Neuropathic Pain: The Pharmacological Management of Neuropathic Pain in Adults in Non-specialist Settings. London: National Institute for Health and Care Excellence, (UK);2013.25577930 · pubmed ↗
- 4Jensen MP Chodroff MJ Dworkin RH : The impact of neuropathic pain on health-related quality of life: review and implications. Neurology. 2007;68:1178–1182. 10.1212/01.wnl.0000259085.61898.9e 17420400 · doi ↗ · pubmed ↗
- 5Schmader KE : Epidemiology and impact on quality of life of postherpetic neuralgia and painful diabetic neuropathy. Clin. J. Pain. 2002;18:350–354. 10.1097/00002508-200211000-00002 12441828 · doi ↗ · pubmed ↗
- 6O'Connor AB : Neuropathic pain: quality-of-life impact, costs and cost effectiveness of therapy. Pharmaco Economics. 2009;27(2):95–112. 10.2165/00019053-200927020-00002 19254044 · doi ↗ · pubmed ↗
- 7Attal N Cruccu G Baron R : EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur. J. Neurol. 2010;17:1113–e 88. 10.1111/j.1468-1331.2010.02999.x 20402746 · doi ↗ · pubmed ↗
- 8Hartemann A Attal N Bouhassira D : Working Group on the Diabetic Foot from the French-speaking Society of Diabetology. Painful diabetic neuropathy: diagnosis and management. Diabetes Metab. 2011;37(5):377–388. 10.1016/j.diabet.2011.06.003 21820345 · doi ↗ · pubmed ↗