Heart failure, recurrent vascular events and death in patients with ischemic stroke—results of the MonDAFIS study
Serdar Tütüncü, Manuel C. Olma, Claudia Kunze, Joanna Dietzel, Johannes Schurig, Michael Rosenkranz, Robert Stingele, Matthias Maschke, Peter U. Heuschmann, Paulus Kirchhof, Ulrich Laufs, Darius G. Nabavi, Joachim Röther, Götz Thomalla, Roland Veltkamp, Matthias Endres

TL;DR
This study finds that heart failure increases the risk of heart attacks and death in patients with ischemic stroke, but not the risk of recurring strokes or bleeding.
Contribution
The study provides new evidence on the specific risks associated with heart failure in ischemic stroke patients from a large, multicenter trial.
Findings
Heart failure increases the risk of myocardial infarction and all-cause death in stroke patients.
The risk of recurrent stroke or major bleeding is not significantly higher in heart failure patients.
Adjustments for age, stroke severity, and cardiovascular risk factors were made in the analysis.
Abstract
Heart failure (HF) is associated with poor outcome after stroke, but data from large prospective trials are sparse. We assessed the impact of HF on clinical endpoints in patients hospitalized with acute ischemic stroke or transient ischemic attack (TIA) enrolled in the prospective, multicenter Systematic Monitoring for Detection of Atrial Fibrillation in Patients with Acute Ischemic Stroke (MonDAFIS) trial. HF was defined as left ventricular ejection fraction (LVEF) < 55% or a history of HF on admission. The composite of recurrent stroke, major bleeding, myocardial infarction, and all-cause death, and its components during the subsequent 24 months were assessed. We used estimated hazard ratios in confounder-adjusted models. Overall, 410/2562 (16.0%) stroke patients fulfilled the HF criteria (i.e. 381 [14.9%] with LVEF < 55% and 29 [1.9%] based on medical history). Patients with HF had…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
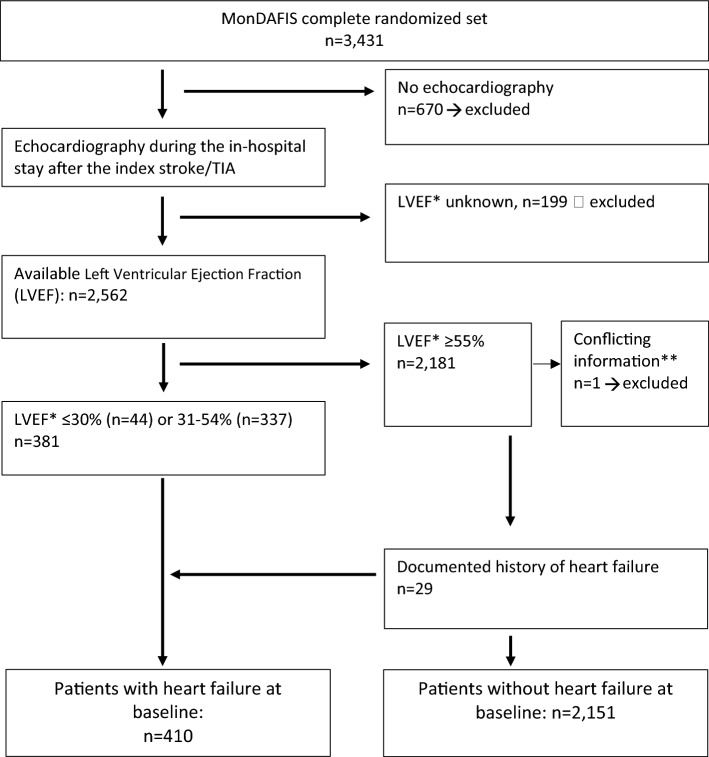 Figure 1
Figure 1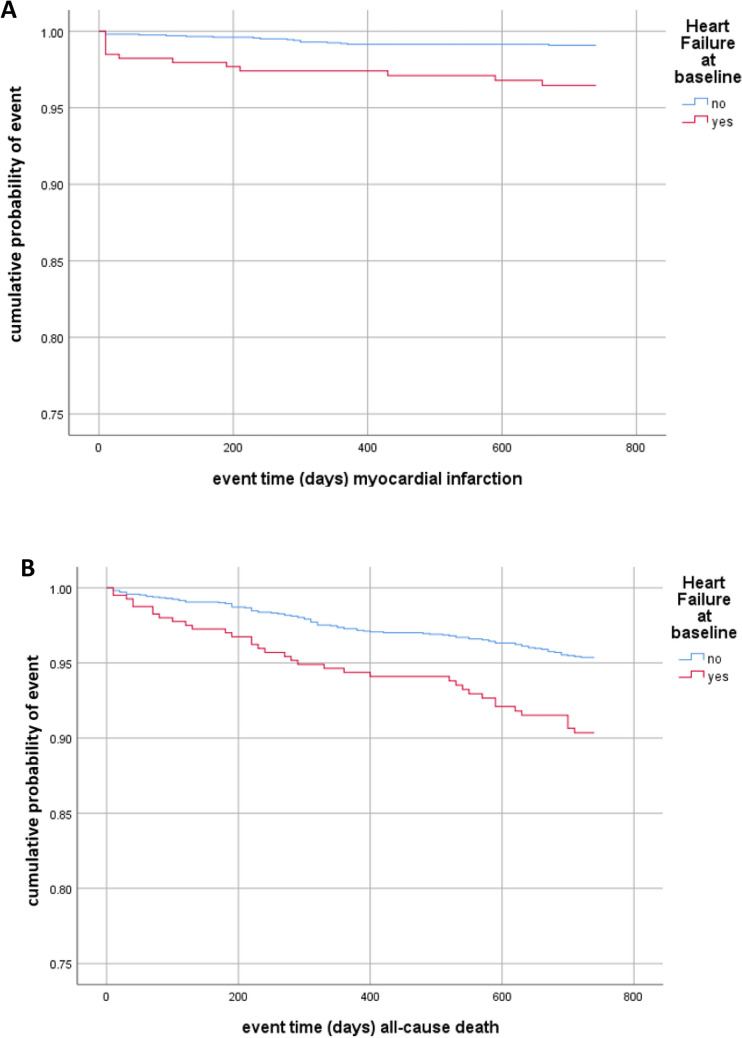 Figure 2
Figure 2- —http://dx.doi.org/10.13039/100014851Bayer Animal Health
- —Charité - Universitätsmedizin Berlin (3093)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Acute Ischemic Stroke Management · Heart Failure Treatment and Management
Introduction
The prevalence of both stroke and heart failure (HF) is high in the elderly, and there is a long list of common cardiovascular risk factors, including hypertension, diabetes, sleep apnea, kidney dysfunction, or atrial fibrillation (AF). HF is regarded as an independent risk factor for ischemic stroke, and about 9% of all ischemic strokes are assumed to be related to HF [1]. Furthermore, there is an association between HF with unfavorable clinical outcome and mortality after stroke [2–6]. In addition, a reduced ejection fraction in patients with ischemic stroke and atrial fibrillation is associated with mortality [7]. In contrast, it is less clear whether HF is also associated with recurrent vascular events following an ischemic stroke. Data on recurrent ischemic stroke in stroke patients with HF are conflicting: a systemic review and meta-analysis of seven prospective trials with differing follow-up times demonstrated a significant association of HF with recurrent ischemic stroke in 9173 ischemic stroke patients [8]. However, a retrospective insurance data-based analysis showed no significant association of recurrent stroke and HF in 370,527 ischemic stroke patients [9]. While there are several publications focusing on myocardial infarction following ischemic stroke [10, 11], data on the association of myocardial infarction with HF in ischemic stroke patients are scarce [12]. In addition, studies examining the occurrence of major bleeding in association with heart failure in ischemic stroke patients are missing.
In this post-hoc analysis of the prospective multicenter MonDAFIS study, we analyzed the impact of HF at baseline on the composite of recurrent stroke, major bleeding, myocardial infarction, and all-cause death within 24 months after hospitalization for acute ischemic stroke or transient ischemic attack (TIA) [13, 14]. Furthermore, we investigated the association of each vascular endpoint separately with HF and rates of oral anticoagulation after 24 months in patients with or without HF at baseline.
Methods
Study cohort
MonDAFIS was an investigator-initiated randomized trial sponsored by the Charité—Universitätsmedizin Berlin, Berlin, Germany, and supported by an unrestricted research grant from Bayer Vital GmbH, Leverkusen, Germany to the Charité. The study rationale and design [12] as well as the primary and secondary endpoints [14] were published previously. The MonDAFIS study received primary approval from the Ethics Committee of the Charité—Universitätsmedizin Berlin, Germany. All 39 participating study centers provided approval from their respective ethics committees. All study patients gave written informed consent. The MonDAFIS trial complies with the Declaration of Helsinki. Patients were recruited from December, 2014 to September, 2017. A critical event committee adjudicated all serious adverse events (including recurrent stroke, myocardial infarction, major bleeding, and all-cause death). The members met at the study coordinating center and were blinded to trial randomization.
Study population
Men or women ≥ 18 years of age were eligible for study enrollment if they had an ischemic stroke according to WHO criteria [15]. If the newly occurring neurological deficits were transient in nature (consistent with a TIA), an additional inclusion criterion required either a neurologist to have observed and documented the acute neurological deficits or evidence of a corresponding acute ischemic lesion on imaging. Patients were excluded due to withdrawal of informed consent and data deletion or lack of any data. Detailed information regarding further in- and exclusion criteria as well as the trial intervention was published previously [14].
In the vast majority of MonDAFIS patients, left ventricular ejection fraction (LVEF) was determined by echocardiography at baseline as part of routine diagnostic procedures. The LVEF was captured in the eCRF as a categorized variable (LVEF ≥ 55% (“normal”), LVEF 31–54% (“slightly reduced”), LVEF ≤ 30% (“reduced”)). The rationale for this definition was based on the ESC guidelines for measuring LVEF that was valid at the time of study conception. In addition, heart failure (HF) was considered as pre-existing at baseline if it was reported by the patient or evident from existing medical reports (history of HF). In the present analysis, patients with a documented LVEF < 55% and/or a history of HF at baseline were considered HF patients. Patients without echocardiography during the index-stroke/TIA related hospital stay were excluded from the present analysis.
Outcomes
In line with the pre-defined secondary endpoint of the MonDAFIS study, we assessed the composite of recurrent stroke, myocardial infarction, major bleed, and all-cause death within 2 years after the index stroke in defined subgroups. Furthermore, the individual components of the composite endpoint were analyzed separately. The rate of oral anticoagulation within 24 months after the index event was assessed in patients with and without HF at baseline.
Statistical methods
This is an explorative analysis of the MonDAFIS study data set using predefined outcomes. Baseline characteristics are reported as frequencies and percentages for categorical variables or median and limits of the interquartile range (IQR; [25th and 75th percentile]) for metric variables. For the outcomes of interest, we conducted event-free survival analyses comparing cumulative hazards between patient groups. Event-free survival time, as well as survival, was measured in person-days until one of the events of the combined endpoint or death occurred, the study ended, or the participant was lost to follow-up. These dropouts are censored at the time of last contact. We used Kaplan–Meier curves and the log-rank test to compare crude cumulative hazard distributions. Cox Proportional Hazard models (crude and adjusted for age and cardivascular risk factors as arterial hypertension, diabetes mellitus, hyperlipoproteinemia, coronary heart disease, detection of atrial fibrillation and group randomization as well as stroke severity measured by the NIHSS score at baseline given as model 1 and model 2 with further adjustment for intravenous thrombolysis and endovascular thrombectomy in addition) were used to estimate hazard ratios (HR) for each vascular endpoint, the composite endpoint for all-cause death risk within 2 years after ischemic stroke or TIA. In a further sensitivity analysis, we added the status of antithrombotic therapy (antiplatelets or oral anticoagulation) at discharge after the index stroke in to the above-mentioned models. Cox Proportional Hazard assumption was checked. For the endpoint ‘oral anticoagulation 24 months after index event’ a multiple binary logistic regression analysis (adjusted for AF and detection of left atrial and/or ventricular thrombus) was conducted and adjusted odds ratios, as well as respective confidence intervals (CI) are reported. Data preparation was done using the software IBM SPSS Statistics 24.
Results
Of 3,431 patients included in MonDAFIS, LVEF was available in 2562 (75%) patients (mean age 67 [57–76] years, 39.5% female, median NIHSS score on admission 2 points [1–4]). Figure 1 shows the derivation of the study population. Patients without documented LVEF were older, more often had a TIA as index event and a stroke or TIA before the index event (Table 1 Online Supplement).Fig. 1. Derivation of the study population. *LVEF left ventricular ejection fraction, **Data of one MonDAFIS patient were excluded from analysis due to conflicting information regarding first diagnosis of heart failure during in-hospital stay
Overall, 381/2562 (14.9%) patients had a LVEF < 55% and 75/2562 patients had a documented past medical history of HF (of which 29 had a LVEF ≥ 55%). Therefore, a total of 410/2562 (16.0%) patients fulfilled at least one of the pre-defined HF criteria (Fig. 1). Baseline characteristics and results of multiple binary logistic regression of patients with vs without HF are shown in Table 1.Table 1. Baseline characteristics of MonDAFIS study patients with or without heart failure at baselineUnivariate analysisp-valueMultivariate analysisHeart failure, n = 410No heart failure, n = 2151OR (95% CI)p-valueAge, years, median [IQR]69 [60–77]66 [56–76] < 0.0011.01 (0.99–1.02)0.078Age categories, years, n (%)0.001-- < 65149 (36.3)991 (46.1)-- 65–74121 (29.5)566 (26.3)-- 75–84116 (28.3)521 (24.2)-- > 8424 (5.9)73 (3.4)--Female sex, n (%)119 (29.0)866 (40.3) < 0.0010.79 (0.61–1.03)0.081Body weight, kg, mean (SD) [IQR]81 [70–95]80 [70–90]0.0091.01 (1.00–1.02)0.052Index stroke, * n (%)0.020TIA99 (24.1)640 (29.8)1S troke311 (75.9)1507 (70.2)1.11 (0.86–1.44)0.422NIHSS score on admission, median [IQR]3 [1–5]2 [1–4]0.0131.05 (1.02–1.09)0.002In-hospital treatment, n (%) Intravenous thrombolysis91 (22.2)500 (23.2)0.644-- Endovascular treatment15 (3.7)56 (2.6)0.233-- Hemicraniectomy1 (0.2)1 (0.0)0.190-- Carotid surgery or stenting9 (2.2)33 (1.5)0.334--Cardiovascular risk factors, n (%) Diabetes mellitus150 (36.6)508 (23.6) < 0.0011.33 (1.04–1.70)0.026 Hypertension346 (84.4)1,615 (75.2) < 0.0011.14 (0.83–1.57)0.408 Hypercholesterolemia237 (57.8)1,125 (52.4)0.0431.06 (0.84–1.33)0.634 Coronary heart disease116 (28.3)191 (8.9) < 0.0013.12 (2.36–4.13) < 0.001 Peripheral arterial disease34 (8.3)60 (2.8) < 0.0012.04 (1.28–3.25)0.003 Prior ischemic stroke or TIA68 (16.6)326 (15.2)0.469-- Smoker211 (51.7)1017 (47.6)0.129-- Randomization to the intervention group, n (%)200 (48.8)1072 (49.8)0.695--^**^OR and 95% CI for continues variables were expressed per point (BMI, NIHSS) or per each year of age
Patients with HF more often had diabetes mellitus [OR 1.33; 95% CI 1.04–1.70; P = 0.026], coronary artery disease [OR 3.12; 95% CI 2.36–4.13; P < 0.001], and peripheral arterial disease [OR 2.03; 95% CI 1.27–3.24; P = 0.003] than non-HF patients. Moreover, patients with HF had a higher stroke severity on admission than patients without HF [assessed by the NIHSS score; OR per point 1.05; 95% CI 1.02–1.09; P = 0.002).
Association of heart failure with clinical outcomes
Within two years after index stroke or TIA, the predefined composite endpoint occurred in 480/2561 (14.0%) of patients, including recurrent stroke in 301 (8.8%) patients, myocardial infarction in 43 (1.3%) patients, major bleeding in 32 (0.9%) patients and all-cause death in 175 (5.1%) patients. Recurrent ischemic stroke or TIA occurred in 283/2561 (8.3%) patients, while 18/2561 (0.7%) patients had a hemorrhagic stroke within 2 years.
After adjusting for cardiovascular risk factors, stroke severity and randomization (model 1), HF was associated with myocardial infarction [HR 2.21; 95% CI 1.02–4.79; P = 0.046], and all-cause death [HR 1.67; 95% CI 1.12–2.49, P = 0.013] within 2 years after the index event. The event rates at different time frames for myocardial infarction and all-cause death are shown in Tables 2 and 3 Online Supplement. On the contrary, neither the composite endpoint [HR 1.28; 95% CI 0.99–1.66] nor recurrent ischemic stroke or TIA [HR 1.07; 95% CI: 0.74–1.55] nor major bleeding [HR 1.93; 95% CI 0.73–5.06] (Fig. 2 and Table 2) was significantly increased in stroke patients with HF. Additional adjustment for intravenous thrombolysis and endovascular thrombectomy (model 2) yielded similar results (Table 2). Also, excluding patients with a documented medical history of HF but normal LVEF (≥ 55%) at baseline yielded similar results (Table 4 Online Supplement). Adding the status of 'no-antithrombotic’ treatment at hospital discharge after the index stroke into both models of the cox regression analysis did not change the significant impact of heart failure in the occurrence of myocardial infarction or all-cause death.Table 2. Adjusted survival analyses, Cox regression, hazard ratios for the composite endpoint (recurrent stroke, myocardial infarction, major bleeding, all-cause death) and its components as well as recurrent ischemic stroke/TIA within 24 months after the index stroke/TIA for patients with heart failure (n = 410) compared to those without heart failure at baselineCrudeAdjusted, Model 1^a^Adjusted, Model 2^a^HR (95% CI)PHR (95% CI)PHR (95% CI)PComposite endpoint^b^1.54 (1.20–1.98)0.0011.28 (0.99–1.66)0.0651.29 (0.99–1.67)0.060All-cause death2.15 (1.46–3.16) < 0.0011.67 (1.12–2.49)0.0131.65 (1.10–2.47)0.015Recurrent stroke^c^1.21 (0.86–1.69)0.2741.08 (0.76–1.54)0.6681.09 (0.77–1.56)0.620Recurrent ischemic stroke or TIA1.16 (0.81–1.65)0.4251.07 (0.74–1.55)0.7371.08 (0.75–1.57)0.680Recurrent ischemic stroke1.24 (0.83–1.85)0.2991.08 (0.71–1.66)0.7191.09 (0.71–1.67)0.683Recurrent TIA0.91 (0.43–1.93)0.8060.98 (0.46–2.11)0.9550.99 (0.46–2.14)0.986Myocardial infarction3.96 (1.94–8.08) < 0.0012.21 (1.02–4.79)0.0462. 18 (1.01–4.76)0.050Major bleed1.93 (0.76–4.89)0.1681.93 (0.73–5.06)0.1841.89 (0.72–4.99)0.196^a^Adjusted Model 1: for age, stroke severity (NIHSS score on admission), diabetes mellitus, arterial hypertension, hyperlipoproteinemia, coronary heart disease, detection of atrial fibrillation in-hospital, randomization; Adjusted Model 2: all variables of Adjusted Model 1 and additionally intravenous thrombolysis and endovascular thrombectomy^b^Recurrent stroke, MI, major bleed, all cause death c) Ischemic Stroke, Transient Ischemic Attack, Intracerebral Hemorrhage, Subarachnoid HemorrhageFig. 2Time to event analysis. Occurrence of myocardial infarction (A) or all-cause death (B) within 24 months according to heart failure status at baseline
Secondary stroke prevention in patients with heart failure
Information on oral anticoagulation at 24 months was available in 2072/2561 (80.9%) patients and, similarly, on antiplatelet treatment in 2075/2561 (81.0%) patients. Overall, 312/2,072 (15.1%) patients were on anticoagulation and 1,645/2,075 (79.4%) patients on antiplatelets at 24 months. In patients with HF at baseline, information on oral anticoagulation at 24 months was available in 304/410 (74.2%) patients. There was a statistically significant difference in the rate oral anticoagulation in HF patients vs. non-HF patients (63/304 [20.7%] vs. 249/1768 [14.1%], respectively, P = 0.004). AF was diagnosed in 46/63 (73.0%) of those with oral anticoagulants and HF. The rate of oral anticoagulation was 15.7% in HF patients vs 11.8% in non-HF patients at 6 months after the index stroke/TIA (p = 0.046) and 16.6% vs 12.9% after 12 months (P = 0.072) (Table 5 online supplement).
After multivariate adjustment (including newly detected AF within 24 months and left ventricular or left atrial thrombus at baseline), there was no significant association between HF status at baseline and oral anticoagulation after 24 months [OR 0.89; 95% CI 0.51–1.56; P = 0.689].
Discussion
The prospective multicenter MonDAFIS study shows that ischemic stroke or TIA patients with comorbid HF had a significantly higher rate of myocardial infarction and all-cause mortality within 24 months than non-HF patients. One strength of our post hoc analysis is the large number of clinical endpoints assessed by an independent endpoint committee and standardized follow-up for 24 months. Our data confirm that stroke/TIA patients with comorbid HF are not only more likely to have cardiovascular risk factors (such as diabetes, coronary heart disease, peripheral arterial disease) but also to have more severe strokes than stroke patients without HF [2]. Our finding of a statistically higher rate of myocardial infarction over 24 months after stroke/TIA in the presence of HF is consistent with the results of a large multicenter registry in the UK based on NHS primary care data of 9,840 patients [12]. The detected higher mortality rate in ischemic stroke patients with comorbid HF is also in line with previous studies [6, 9]. Of note, the rate of recurrent stroke as well as recurrent ischemic stroke or TIA was not associated with HF in our study, which was also found in a retrospective analysis of a large registry but is not consistent with a meta-analysis of prospective studies [8, 9]. The follow-up period of 2 years was may be too short to observe any potential association between HF and ischemic stroke—the authors of the WARCEF trial reported a higher rate of ischemic strokes during a follow-up period that was approximately 1.5 years longer. One study reported a significant association of recurrent intracerebral hemorrhage in patients with HF compared to non-HF patients [9]. In MonDAFIS, the HF status at baseline was not associated with the rate of major bleeding after stroke, even though 21% of HF patients received oral anticoagulation at 24 months. In fact, OAC status was not statistically different between HF vs. non-HF patients after adjusting for AF and presence of cardiac thrombi.
There are some limitations that should be mentioned. First, the MonDAFIS study was not designed to investigate the impact of HF on recurrent vascular events or death. Second, as echocardiography was conducted according to routine clinical practice respective data were available for only 75% of the total study population. Third, we had no systematic information on biomarkers, like natriuretic peptides. Fourth, we had no further information on HF status after hospital discharge after the index-stroke/TIA. Fifth, our results cannot be applied to all stroke patients, as patients had to provide informed consent to participate in the MonDAFIS study. Finally, we are not able to specify the cause of death. Due to formal data protection laws we did not have access to death certificates and autopsy is not regularly performed even if patients die in hospital.
Conclusion
Patients with acute ischemic stroke or TIA with comorbid HF have a higher prevalence of cardiovascular risk factors, suffered more severe (index) strokes and have a higher risk for myocardial infarctions or all-cause death within 24 months after the index stroke. Special attention should be paid to the prevention of myocardial infarction in this patient population and cardiac follow-up should be recommended in stroke patients with HF.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 26 KB)