Presence of Teen Clubs and its Association with Clinic Attendance among Adolescents Living with HIV in Tanzania: A Retrospective Cohort Study
Ephrasia Hugho, Theopista Masenga, Jenny Renju, Ola Johanpour, Gretchen Antelman, Sajida Kimambo, Frederick Haraka, Sia E. Msuya

TL;DR
Teen clubs at HIV clinics in Tanzania are linked to better clinic attendance among adolescents living with HIV.
Contribution
This study empirically demonstrates the positive impact of teen clubs on adolescent HIV clinic attendance in Tanzania.
Findings
Adolescents with access to teen clubs had a 16% higher likelihood of good clinic attendance.
Adolescents aged 15–19 were less likely to have good clinic attendance compared to younger adolescents.
Being on ART for more than two years was also associated with improved clinic attendance.
Abstract
Adolescent's living with Human Immunodeficiency Virus (HIV) are widely reported to have poor adherence to antiretroviral therapy (ART) due to stigma and fear of discrimination. A “Teen club” is an adolescent centered intervention designed to reduce social stigma and improve adherence and retention in HIV care. In this study we determined how the availability of teen clubs within routine HIV care and treatment facilities affects adolescents' clinic attendance. We conducted a retrospective cohort study using secondary data from routine clinic records on adolescents (10–19 years) who started ART between 2010 and 2016, and had documented clinic visits between March 2017 and September 2017 at HIV care and treatment clinics (CTC) in northern and central Tanzania. Good clinic attendance was defined as attending at least four monthly clinic visits during the 7-month follow-up period. A Poisson…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
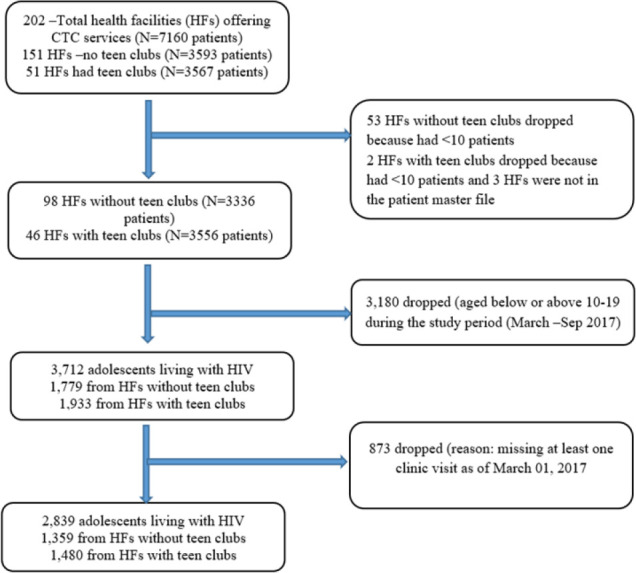 FIGURE 1
FIGURE 1| Variable | Total | Health facility status | P Value | ||||
|---|---|---|---|---|---|---|---|
| No Teen club (n=1359) | Teen club (n=1480) | ||||||
| n | % | n | % | n | % | ||
| Sex | |||||||
| Male | 1265 | 44.6 | 600 | 44.1 | 655 | 44.9 | .675 |
| Female | 1574 | 55.4 | 756 | 55.9 | 825 | 55.1 | |
| Age at ART initiation | |||||||
| <10 years | 1230 | 43.3 | 574 | 42.2 | 656 | 44.3 | .185 |
| 10–14 | 1366 | 48.1 | 656 | 48.3 | 710 | 48.0 | |
| 15–19 | 243 | 8.6 | 129 | 9.5 | 114 | 7.7 | |
| Age during the study | |||||||
| <15 | 1935 | 68.2 | 915 | 67.3 | 1020 | 68.9 | .364 |
| 15–19 | 904 | 31.8 | 444 | 32.7 | 460 | 31.9 | |
| Baseline WHO Stage | |||||||
| 1 | 519 | 18.3 | 253 | 18.6 | 266 | 18.3 | .072 |
| 2 | 946 | 33.3 | 477 | 35.1 | 469 | 33.3 | |
| 3 | 1131 | 39.8 | 516 | 38.0 | 615 | 39.8 | |
| 4 | 240 | 8.6 | 110 | 8.1 | 130 | 8.6 | |
| Missing | 3 | 0.1 | 3 | 0.2 | 0 | 0 | |
| Reported ARV Adherence | |||||||
| Good | 2424 | 85.4 | 1154 | 84.9 | 1270 | 85.4 | .138 |
| Poor | 126 | 4.4 | 71 | 5.2 | 55 | 4.4 | |
| Missing | 289 | 10.2 | 134 | 9.9 | 155 | 10.2 | |
| Health facility level | |||||||
| Dispensary | 274 | 9.7 | 212 | 15.6 | 62 | 4.2 | <.001 |
| Health center | 932 | 32.8 | 508 | 37.4 | 424 | 28.6 | |
| Hospital | 1633 | 57.5 | 639 | 47.0 | 994 | 67.2 | |
| Region | |||||||
| Arusha | 647 | 22.8 | 110 | 8.1 | 537 | 36.3 | <.001 |
| Dodoma | 613 | 21.6 | 454 | 33.4 | 159 | 10.7 | |
| Kilimanjaro | 864 | 30.4 | 476 | 35.0 | 388 | 26.2 | |
| Tabora | 715 | 25.2 | 319 | 23.5 | 396 | 26.8 | |
| Outcomes | Total | No teen club (n=1359 | Teen club (n=1480) | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Good clinic attendance | 2075 | 73.1 | 918 | 67.6 | 1157 | 78.2 |
| Retained | 2611 | 92.0 | 1226 | 90.2 | 1385 | 93.6 |
| LTFU | 212 | 7.5 | 129 | 9.5 | 83 | 5.6 |
| Stopped ART | 4 | 0.1 | 2 | 0.2 | 2 | 0.1 |
| Died | 13 | 0.4 | 2 | 0.2 | 10 | 0.7 |
| Variable | Univariate analysis | Multivariable analysis | ||||
|---|---|---|---|---|---|---|
| n | n (%) | cRR (95% CI) | P-value | aRR (95% CI) | P value | |
| Health facility status | ||||||
| No teen club | 1359 | 918 (67.6) | 1.00 | 1.00 | ||
| Teen club | 1480 | 1157 (78.2) | 1.16(1.10 – 1.21) | <.001 | 1.15 (1.09 – 1.20) | <.001 |
| Sex | ||||||
| Male | 1265 | 938 (74.2) 1.00 | 1.00 | |||
| Female | 1574 | 1137 (72.2) | 0.97 (0.93 – 1.01) | .251 | 0.94 (0.93 – 1.02) | .364 |
| Age | ||||||
| <15 | 1935 | 1450 (74.9) | 1.00 | 1.00 | ||
| 15–19 | 904 | 625 (69.1) | 0.92 (0.88 – 0.97) | .002 | 0.93 (0.88 – 0.98) | .003 |
| Baseline WHO Stage | ||||||
| 1 | 519 | 399 (76.9) | 1.00 | 1.00 | ||
| 2 | 946 | 661 (69.9) | 0.91 (0.85 – 0.97) | .003 | 0.90 (0.84 – 0.96) | .001 |
| 3 | 1131 | 830 (73.4) | 0.95 (0.90 – 1.01) | .121 | 0.93 (0.88 – 0.98) | .014 |
| 4 | 240 | 182 (75.8) | 0.99 (0.91 – 1.07) | .754 | 0.96 (0.88 – 1.04) | .315 |
| Unknown | 3 | 3 (100) | 1.30(1.24 – 1.36) | <.001 | 1.58(1.46 – 1.72) | <.001 |
| Duration on ART | ||||||
| <1 year | 138 | 90 (65.2) | 1.00 | 1.00 | ||
| 1–2 years | 494 | 322 (65.2) | 0.99 (0.87 – 1.15) | .994 | 1.00 (0.86 – 1.15) | .952 |
| More than 2 years | 2207 | 1663 (75.4) | 1.16(1.02 – 1.30) | .023 | 1.15 (1.02 – 1.30) | .025 |
| Health facility level | ||||||
| Dispensary | 274 | 196 (71.5) | 1.00 | – | – | – |
| Health center | 932 | 675 (72.4) | 1.01 (0.93 – 1.10) | .774 | – | – |
| Hospital | 1633 | 1204 (73.1) | 1.03 (0.95 – 1.12) | .459 | – | – |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · Adolescent and Pediatric Healthcare · Homelessness and Social Issues
INTRODUCTION
In 2016 in Tanzania, antiretroviral therapy (ART) coverage was 48% among children (0–14 years) and 63% among adults.^1^ Despite the rapid scale up of ART, adolescents living with HIV (ALHIV) face challenges in accessing and remaining engaged with HIV care and treatment.^2,3^ Poor adherence to scheduled visits has been associated with virological failure and drug resistance.^4^ Age,^5–7^ stigma and fear of discrimination; poverty and inadequate economic resources; education and HIV/ART literacy^8–9^ are individual factors that affect care retention and health outcomes. Various inter-relational factors are also influential, such as social participation, support structures, culture and religion.^3,10^ Finally, structural barriers to accessing the health facility include distance or transportation costs; operating hours, permissions to leave school, and waiting times.^7^
In Malawi, teen clubs met at a designated time and on the same day adolescents were also able to receive all their HIV related care.^11^ In Uganda, Family Clinic Days (FCD), whereby children, adolescents and their family members are given priority care, achieved 75–100% attendance.^12^ Similarly, Kenya improved clinic attendance through their Youth and Adolescent Friendly Services program in 2013.^13^
In 2016, the Ministry of Health in collaboration with Elizabeth Glaser AIDS Foundation (EGPAF) implemented the 53 Teen clubs in northern and central Tanzania to provide psychosocial support to ALHIV and are led by adolescent peer ambassadors who have extensive knowledge on HIV and stigma. The psychosocial support clubs are intended to help adolescents deal with emotional challenges they face from traumatic experiences such as not having access to basic necessities of life. Through this, teen clubs provide adolescents with a safe and supportive space to discuss sexual and reproductive health issues with their peers. By creating a sense of community and shared experience, teen clubs can reduce stigma and discrimination around health issues and provide adolescents with a supportive network of peers who may encourage them to seek out clinical services. They provide avenue for the people to come together, interact and learn skills that will enable them to make informed decisions when they face challenges in life. The EGPAF teen club model has education sessions which provide correct information on sexual and reproductive health, peer psychosocial support, positive change in mind and attitude towards prevention of Sexually Transmitted Infections (STIs) through provision of adolescent friendly services and improving adherence and retention to care among HIV positive adolescents. It also imparts adolescents with life skills for managing both physical and social developmental changes occurring at their age.
Teen club activities were scheduled on Saturdays, and in order to become a member of the club, individuals must meet the following criteria: aged between 10 and 19 years, be aware of their HIV status, and be receiving HIV care services at the specific site. In this study, we compared HIV clinic attendance amongst adolescents receiving HIV care in health facilities with teen clubs to those in facilities without teen clubs.
METHODS
Study Design and Setting
We conducted a retrospective cohort study to assess the association between teen club presence and clinic attendance in a population of ALHIV attending ART care from March to September 2017. The study was conducted in 144 health facilities that offer CTC services. The facilities included in the analysis were located in four regions: Arusha (42 health facilities), Dodoma (36 health facilities), Kilimanjaro (44 health facilities), and Tabora (77 health facilities). As of March 2016, teen clubs were running in 51 health facilities; 16 in Arusha region, 13 in Kilimanjaro region, 3 in Dodoma region and 19 in Tabora region.
Eligibility Criteria
This study included all ALHIV aged 10–19 years who started ART between 2010 and 2016, who were registered and accessing ART care in the selected health facilities and had at least one documented clinic visit between 1^st^ March and 30^th^ September, 2017. All CTC sites with at least 10 ALHIV registered in ART care were eligible for the study.
Sample Size and Sampling
This was a secondary analysis of the available CTC data. All eligible adolescents from 144 CTC sites were included in the study. A total of 2839 participants were obtained for analysis. The Power of the study was calculated by using formula for power calculation for two proportions (power two proportions p1 p2, n1( ) n2( ). With 1359 adolescents in the unexposed group (from health facilities without teen clubs) and 1480 in exposed group (from health facilities with teen clubs), the analysis had 100% power to detect 10% difference in the proportion of adolescents who had optimal clinic attendance in the two groups at 5% significant level. Figure 1 shows the sites and participant selection process.
Sites and Participants Selection Process
Data Source and Study Variables
Data were extracted from routine HIV care and treatment patient records. The primary exposure was availability of the teen club at the health facility. Other variables included sex of the patient, age during the study period, age at ART initiation, reported ARV adherence, duration on ART (time since the initiation of ARVs), World Health Organization (WHO) HIV clinical stage and health facility level (dispensary, health center or hospital).
Good clinic attendance was the primary outcome, defined as having attended at least four visits during the study period, where according to the Tanzanian standard of care for ALHIV, monthly clinic visits were recommended.^13^ The teen clubs were offered monthly and provided clinical services and ART refills. Other outcomes observed at the end of the study follow-up were loss to follow-up (LTFU) defined as not having attended the clinic by the end of the study follow-up period for >90 days ^14^, death or stopping ART, and retention (not LTFU, died or stopped ART).
Data Analysis
Data analysis was performed using STATA version 15. Descriptive statistics (measures of central tendency, frequencies, and percent) were used to summarize continuous and categorical variables. In both the univariate and multivariable analyses, we used modified Poisson regression with robust error variances^19^ to obtain risk ratios (RR) and precise confidence intervals for the association between exposure variables and good clinic attendance. A complete case analysis was performed and only variables with a P value of less than 0.2 in the univariate analysis were included in the multivariable model. Statistical inference for significant association was made at 95% confidence interval and Wald test P value <0.05. The best model fit was the one with the smallest Akaike Information Criterion (AIC) value.
Ethical Considerations
Ethical approval for this secondary analysis was obtained from the Research and Ethics Committee of the Kilimanjaro Christian Medical University College-Tumaini University Makumira (No. 2032). This study was also conducted under the protocol Reaching 90-90-90 evaluation of patient and program characteristics associated with identification of adults and children living with HIV, ART initiation and retention in Tanzania, describing secondary analyses objectives for analyzing the National HIV Care and Treatment data from facilities supported by the EGPAF; approved by the National Research Ethics Committee under the National Institute for Medical Research (NIMR/HQ/R.8a/Vol IX/2185).
RESULTS
Characteristics of Study Participants
A total of 2839 adolescents from 144 health facilities were included in our analyses. The mean (SD) age of the participants was 14.4(2.3) years. The majority (91.4%) of the participants started ART at the age of ≤15 years and 77.7% had been using ART for more than 2 years.
Clinician reported ARV adherence was charted as “good” at every visit for 85.4% of the participants. Participant characteristics were significantly different in terms of health facility level, duration on ART and region of residence when comparing teen club sites versus no teen club sites (Table 1).
Good Clinic Attendance and its Associated Factors
Overall good clinical attendance was 73.1%. A significantly higher proportion (78.2%) of ALHIV who attended facilities with teen clubs completed the good number of clinic visits during the study period compared to adolescents attending clinics without teen clubs (67.6%; P value < .001). Other outcomes observed during the study period include retention care (92%) and loss to follow up (7.5%) Table 2.
In the adjusted analysis, good clinic attendance was independently associated with having a teen club at the health facility, age and duration on ART (Table 3). We observed a 15% higher odds of achieving good clinic attendance among adolescents attending facilities with a teen club compared to those without a teen club (adjusted RR: aRR=1.15, 95% CI:1.09–1.20). Compared to adolescents aged <15 years, those aged 15–19 years were 7% less likely to have good clinic attendance (aRR=0.93, 95% CI: 0.88–0.98). Adolescents who had been on ART for more than 2 years had 15% good clinic attendance compared to those on ART for less than two years (aRR=1.15, 95% C1.02–1.30).
DISCUSSION
The findings of this study suggest that the availability of teen clubs within the health facility could improve adolescents' monthly attendance at the ART clinic. Interestingly, adolescent retention into ART care was good for both study groups (with and without teen clubs). Further, younger ALHIV had a higher odds of having a good clinic attendance during the study period.
Over three-quarters of adolescents receiving ART at health facilities with teen clubs had good clinic attendance.
Teen clubs provide adolescents with time to share life experience with their peers^16^ thus providing strong peer support. Also, adolescents attending facilities with teen clubs might have been motivated to attend due to the availability of sexual and reproductive health education sessions, or to benefit from the integration of psychosocial/peer support and HIV clinical services provided during the teen club meetings.^17^ The teen clubs are offered on a Saturday, they do not interfere with school hours^7^ and may provide a more private environment for adolescents.^18^ Further, good clinical attendance might have been influenced by awareness and acceptance of their disease status (disclosure) which is criterion for joining the teen clubs perhaps increasing the adolescents' understanding of the importance of being on long time ART.^5^ Similar findings were reported in Malawi and Uganda where adolescent support groups were found to reduce rates of loss to follow up and improve clinic attendance.^10–11^
Older adolescents (15–19 years old) were found to be less likely to have good clinic attendance compared to younger adolescents. Poor clinic attendance at this age might be due to other family and school responsibilities.^7^ Also older adolescents may be negotiating sexual relations and facing challenges disclosing their status,^5^ which could lead them to discontinue their care. A fear of needing to transition to adult care has also been shown to repel older ALHIV from attending clinics.^6^ Similar findings were observed in Uganda and Malawi where it was reported that older adolescents had higher risk of not remaining in care.^10, 19^ There is a need for providers and teen club facilitators to implement age-appropriate strategies to support adherence to clinic appointments, recognizing the increasing need for autonomy and self-management among older adolescents, in order to maintain access to HIV care.
Adolescents who were on ART for more than two years were found to have good clinic attendance compared to those on ART for less than two years. Good clinic attendance leading to better retention in care among patients on ART for long time has also been reported in the United States.^9^ Perhaps those on ART for a longer period are knowledgeable about medication adherence and they believe that medication enables them to live longer.^8^ Having no problems in taking medications (little or no side effects) also plays an important role in retaining patients in clinics hence maintaining their practice of attending clinic for medication refill.^7^
Limitations
Teen clubs were not evenly distributed across the study areas since the priority for teen club establishment was given to the high level health facilities with high volume of patients.
Participants receiving ART care in health facilities without teen clubs differed in some characteristics from those in teen club site thus might have affected our results. Further, this study was not able to assess other factors such as distance to health facility or other aspects of quality of care, including adolescent awareness and attendance of the clubs.
CONCLUSION
The findings of this study indicate that adolescents enrolled into teen clubs are more likely to have good clinic attendance during the study period, supporting growing evidence that teen clubs can support adolescents to achieve good clinic attendance. There is a need for newly enrolled adolescents in HIV care and treatment to join the support group and assess whether frequency and consistency of adolescent participation in the teen club relates to improved health outcomes. Qualitative research should be conducted to explore adolescents' perception of teen club and other ART outcomes as well as other enablers of clinic attendance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. United Republic of Tanzania: HIV Country Profile: 2016. WHO/HIV/2017.59. www.who.int/hiv/data/Country_profile_United_Rep_of_Tanzania.pdf?ua=1. Published 2017. Accessed April 4, 2018.
- 2Mburu G, Ram M, Oxenham D, Haamujompa C, Iorpenda K, Ferguson L. Responding to adolescents living with HIV in Zambia: A social–ecological approach. Child Youth Serv Rev. 2014;45:9–17. doi:10.1016/j.childyouth.2014.03.033 · doi ↗
- 3Williams S, Renju J, Ghilardi L, Wringe A. Scaling a waterfall : a meta-ethnography of adolescent progression through the stages of HIV care in sub-Saharan Africa. J Int AIDS Soc. 2017;20(1):1–17. doi:10.7448/IAS.20.1.21922 PMC 564031228953326 · doi ↗ · pubmed ↗
- 4Bastard M, Pinoges L, Balkan S, Szumilin E, Ferreyra C, Pujades-Rodriguez M. Timeliness of Clinic Attendance Is a Good Predictor of Virological Response and Resistance to Antiretroviral Drugs in HIV-Infected Patients. P Lo S One. 2012;7(11). doi:10.1371/journal.pone.0049091 PMC 349230923145079 · doi ↗ · pubmed ↗
- 5Lowenthal ED, Jibril HB, Sechele ML, Mathuba K, Tshume O, Anabwani GM. Disclosure of HIV status to HIV-infected children in a large African treatment center: Lessons learned in Botswana. Child Youth Serv Rev. 2014;45:143–149. doi:10.1016/j.childyouth.2014.03.031 · doi ↗
- 6Lee S, Hazra R. Achieving 90-90-90 in paediatric HIV: Adolescence as the touchstone for transition success. J Int AIDS Soc. 2015;18(Suppl 6):5–9. doi:10.7448/IAS.18.7.20257 PMC 467084326639113 · doi ↗ · pubmed ↗
- 7Maskew M, Fox MP, Evans D, et al. Insights into Adherence among a Cohort of Adolescents Aged 12–20 Years in South Africa: Reported Barriers to Antiretroviral Treatment. AIDS Res Treat. 2016;2016. doi:10.1155/2016/4161738 PMC 510270227867661 · doi ↗ · pubmed ↗
- 8Roura M, Busza J, Wringe A, Mbata D, Urassa M, Zaba B. Barriers to Sustaining Antiretroviral Treatment in Kisesa, Tanzania: A Follow-Up Study to Understand Attrition from the Antiretroviral Program. AIDS Patient Care STDS. 2009; 23(3):203–210. doi:10.1089/apc.2008.012919866538 PMC 2776987 · doi ↗ · pubmed ↗