Lactating Adenoma Arising From Ovarian Mature Teratoma: An Unusual Presentation of a Young Pregnant Woman
Sharmilla Thirugnanasambandan, Kalaivani Amitkumar, Muthu Sudalaimuthu

TL;DR
A rare case of lactating adenoma in a pregnant woman's ovarian teratoma is reported, highlighting unusual dual findings and confirmed with immunohistochemistry.
Contribution
The novelty lies in the first reported case with both choroidal plexus and lactating adenoma in an ovarian teratoma, confirmed using IHC markers.
Findings
Lactating adenoma arising from ovarian mature teratoma confirmed via immunohistochemical markers.
Dual rare findings of choroidal plexus and mammary tissue hyperplasia in a benign ovarian teratoma.
Estrogen and progesterone receptor positivity in luminal and ductal cells confirmed mammary tissue.
Abstract
Mature teratoma is a benign germ cell tumor, histologically comprising components from mesoderm, ectoderm, and endoderm layer tissue. Here, we report a rare case of lactating adenoma arising from mature teratoma of the ovary in a pregnant female. To the best of our knowledge, only four cases of lactating adenoma arising from ovarian teratoma have been reported in the literature so far. This case is the fifth case reported worldwide, and the first case report with dual rare findings - choroidal plexus and lactating adenoma of mammary tissue in benign mature cystic teratoma. This is the second case report which uses immunohistochemical (IHC) markers to confirm the diagnosis. Grossly, the cystic structure was measuring 10x7x5cm. The cut surface revealed mixed solid and cystic areas filled with pultaceous material admixed with hair. Microscopy showed an ovarian cyst lined by stratified…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1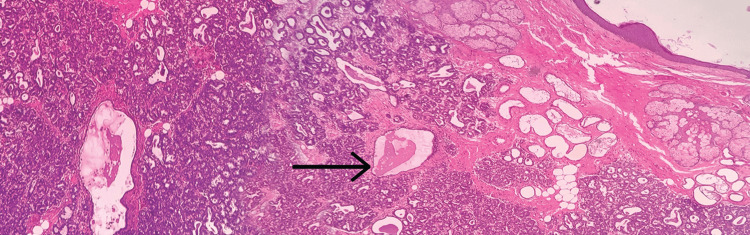 Figure 2
Figure 2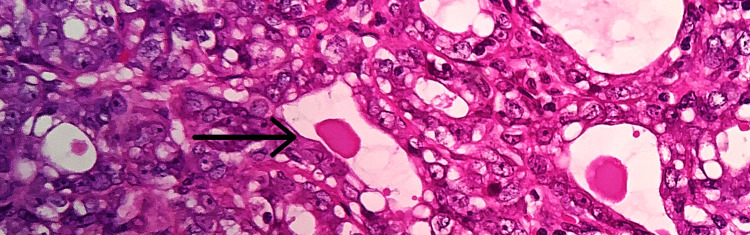 Figure 3
Figure 3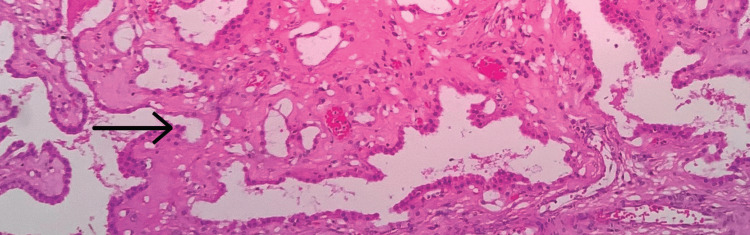 Figure 4
Figure 4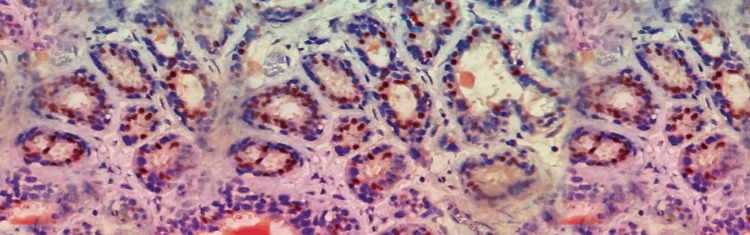 Figure 5
Figure 5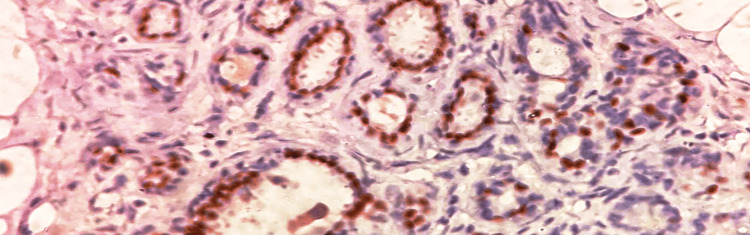 Figure 6
Figure 6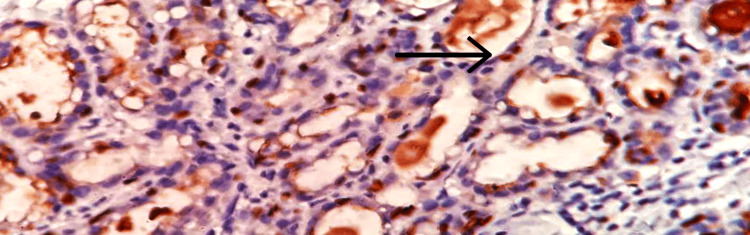 Figure 7
Figure 7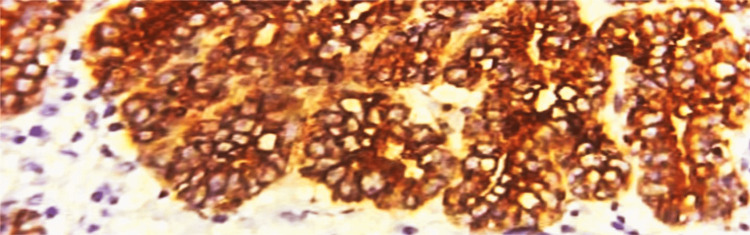 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian cancer diagnosis and treatment · Testicular diseases and treatments · Intraperitoneal and Appendiceal Malignancies
Introduction
Mature teratoma is an ovarian germ cell tumor consisting of mature tissues originating from two or three germ cell layers (ectoderm, endoderm, mesoderm). This is the most prevalent ovarian germ cell tumor, especially in young females in the reproductive age group. It accounts for 69% of germ cell tumors and 95% of teratomas [1]. The ectodermal derivative includes skin, sebaceous glands, hair follicles, and neural tissue, mainly glial tissues. Mesoderm derivatives such as bone, teeth, cartilage and smooth muscles, and endodermal structures such as gastrointestinal, respiratory, or bronchial epithelium, thyroid and salivary glands can be found. Despite being a benign tumor, older individuals rarely experience malignant transformation, which most of the time manifests as squamous cell carcinoma [2] or thyroid carcinoma [3]. We present the histological and immunohistochemical (IHC) findings of a sporadic case of lactating adenoma in a mature ovarian teratoma.
Case presentation
A 35-year-old female primigravida at 39 weeks of gestational age presented for the first time to the hospital with decreased fetal movements. The patient was admitted, vitals were checked and within normal limits, and then cardiotocography monitoring was started, and fetal distress was detected. The patient was immediately taken for an emergency lower-segment caesarian section. Intraoperatively, the right-sided complex ovarian cyst was noted on the table and removed. No antenatal scan was done before. Grossly, the cystic structure measured 10x7x5 cm (Figure 1). The cut surface revealed mixed solid and cystic areas filled with pultaceous material admixed with hair. Microscopy shows an ovarian cyst wall lined by stratified squamous epithelium with underlying sebaceous glands, apocrine acini, fatty tissue, smooth muscle, and glial tissues (Figure 2). Also noted is mammary tissue composed of hyperplastic acini with central dilated ducts filled with eosinophilic secretions arranged in multiple lobules (Figure 3). The hyperplastic acini are lined by one to two layers of low columnar epithelium with round nuclei and inconspicuous nucleoli (Figure 3). Secretory vacuoles and luminal secretions were also noted. We also noted glial tissue with choroidal plexus (Figure 4) in a few sections. Immunohistochemistry with estrogen receptor (ER) (Figure 5) and progesterone receptor (PR) (Figure 6) showed luminal and ductal nuclear positivity. Strong expression of IHC markers such as p63 (Figure 7) and pan-cytokeratin (pan-CK) (Figure 8) was noted in the myoepithelial cells and luminal cells, respectively. Hence, we confirmed the diagnosis as mature cystic teratoma with lactating mammary adenoma. Post-operatively, the patient was asymptomatic and on regular follow-up. No recurrence has been reported till now.
The gross image of ovarian cyst with cut surface showing pultaceous material with tufts of hair (arrow mark).
Microscopic examinationCyst wall lined by stratified squamous epithelium and pilosebaceous units. Mammary tissue with central dilated duct filled with secretions (arrow mark), 10x view (hematoxylin and eosin (H&E) stain).
Microscopic examinationHyperplastic acini lined by cuboidal epithelium with round nuclei (arrow mark), 40x view (hematoxylin and eosin (H&E) stain).
Microscopic examinationGlial tissues with choroidal plexus (arrow mark), 40x view (hematoxylin and eosin (H&E) stain).
Immunohistochemical examination of ERThe immunohistochemical marker estrogen receptor (ER) shows strong nuclear positivity in luminal cells of ducts in mammary tissue (40x view).
Immunohistochemical examination of PRThe immunohistochemical marker progesterone receptor (PR) shows strong nuclear positivity in the luminal epithelial cells of ducts in mammary tissue (40x view).
Immunohistochemical examination of p63The immunohistochemical marker p63 shows positivity in the outer basal/myoepithelial cells (arrow mark) of the mammary tissue (40x view).
Immunohistochemical examination of pan-CKThe immunohistochemical marker pan-cytokeratin (pan-CK) demonstrates diffuse strong positivity in the outer myoepithelial cells of the ducts in mammary tissue (40x view).
Discussion
To the best of our knowledge, only four cases of lactating adenoma arising from ovarian teratoma have been reported in the literature so far [4-7]. This is the fifth case reported worldwide and the first case report with two rare findings: choroidal plexus and lactating adenoma of mammary tissue in benign mature cystic teratoma. This is the second case report, which uses IHC markers to confirm the diagnosis. The majority of teratomas contain tiny foci of the intestinal or colonic epithelium [8]. Tsubura et al. reported a similar case in a 30-year-old Japanese lady who is primigravida and delivered at 37 weeks of gestational age [4]. Ulirsch et al. reported a case of teratoma with neurogenic crest and lactating breast tissue in a young gravid female [5]. Although ovarian teratoma frequently involves breast tissue, it is rare for secondary neoplasms, such as lactational adenoma, to form from it. This can make diagnosis harder, especially since teratoma can affect a lot of different tissues. Kato et al. described a case of lactating adenoma-like breast tissue that looked like a benign, mature ovarian teratoma [7]. They found that the glandular epithelium expressed the IHC marker GATA-3.
In this case, the grossly well-circumscribed nature of the lesion and its correlation with a history of current or recent pregnancy will be helpful clues. IHC markers for breast tissue, such as ER and PR, both epithelial markers, exhibit strong nuclear positivity [9,10]. Additionally, p63 and pan-CK, specific myoepithelial markers associated with lactating adenoma, also show positive results [10]. This confirms the diagnosis of a lactating adenoma arising in a mature teratoma.
In similar studies, Moghaddam et al. and Venizelos et al. reported sebaceous carcinoma arising in mature teratoma [2] and [11]. In a young woman, Uzum et al. reported thyroid carcinoma arising from mature teratomas [3]. Tang et al. reported mucinous cystadenoma in mature ovarian teratoma [12]. Hackethal et al. and Dos Santos et al. reported squamous cell carcinoma in mature cystic teratomas [13-15]. Harms et al. say that conventional somatic malignancies like carcinoma, sarcoma, and leukemia can also arise from teratoma [16]. The neoplastic transformation process accounts for only 1-2% of mature dermoid cyst cases [17]. Around 2-3% of teratomas presenting in the pediatric age group have shown malignant transformation [18]. According to Trabzonlu et al., any ovarian teratoma in postmenopausal women should raise suspicions of malignancy [19]. Though secondary neoplasm arising in mature teratoma is a rare manifestation, it is of utmost importance for therapeutic and prognostic purposes. Surgical excision is the preferred treatment; incomplete removal of the cyst poses a higher risk of relapse [20].
According to Blackwell et al., neural components are present in just 37% of mature teratomas, while the choroidal plexus is only present in 2% of instances. Therefore, the observation of choroidal plexus in a mature teratoma, as in this case, is unusual [21].
Conclusions
It is sporadic for lactational adenoma to develop in teratoma. Thorough grossing and careful histopathological examination, with the aid of IHC markers and knowledge of the spectrum of lesions that might develop in a teratoma, can lead to a correct diagnosis. Secondary neoplasms arising from teratoma, although rare, should be kept in mind while examining all cases of teratoma.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ectopic pituitary with pregnancy changes in a benign cystic teratoma of the ovary Pathology Mow C Edwards A Hayman JA 431433311999 https://doi.org/10.1080/0031302991048821064302110.1080/003130299104882 · doi ↗ · pubmed ↗
- 2A case of sebaceous carcinoma arising in a benign cystic teratoma of the ovary and review of the literature Scott Med J Moghaddam Y Lindsay R Tolhurst J Millan D Siddiqui N 02258201310.1177/003693301348266523728765 · doi ↗ · pubmed ↗
- 3Management and follow-up results of an incidental thyroid carcinoma in a young woman with ovarian teratoma Gynecol Endocrinol Uzum AK Iyibozkurt C Canbaz B 7247262920132377278710.3109/09513590.2013.798277 · doi ↗ · pubmed ↗
- 4Lactating mammary tissue in a mature cystic teratoma of the ovary [Article in Japanese]Gan No Rinsho Tsubura A Okada H Izuno Y Shoji T Kusunose N Morii S 532536361990 https://pubmed.ncbi.nlm.nih.gov/2181165/2181165 · pubmed ↗
- 5An unusual teratoma of the ovary: neurogenic cyst with lactating breast tissue Obstet Gynecol Ulirsch RC Goldman RL 400402601982 https://pubmed.ncbi.nlm.nih.gov/6889713/6889713 · pubmed ↗
- 6Lactating breast tissue in benign cystic teratoma Am J Obstet Gynecol Oi RH Dobbs M 729731130197863709010.1016/0002-9378(78)90342-3 · doi ↗ · pubmed ↗
- 7Genetic zygosity of mature ovarian teratomas, struma ovarii, and ovarian carcinoids Virchows Arch Kato N Sakamoto K Murakami K Iwasaki Y Kamataki A Kurose A 17718247320182945531710.1007/s 00428-018-2319-z · doi ↗ · pubmed ↗
- 8Pituitary teratoma: a case series of three cases Cureus Tena Suck ML Ortiz Plata A Moreno Jimenez S Tirado García LA 515202310.7759/cureus.38729 PMC 1024692637292527 · doi ↗ · pubmed ↗