A rare etiology of infantile dyspnea: Oropharyngeal teratoma
Chiboub Dorra, Romdhane Nadia, Jouini Selima, Cherif Maya, Chedly Achraf, Mbarek Chiraz

TL;DR
This paper presents a rare case of an infant with oropharyngeal teratoma, a congenital tumor causing breathing and feeding issues, emphasizing the importance of early diagnosis and surgical treatment.
Contribution
The paper contributes a clinical case report highlighting the management of a rare oropharyngeal teratoma in an infant.
Findings
Oropharyngeal teratomas are rare congenital tumors that can cause upper airway and digestive obstruction.
Early diagnosis using CT and MRI is crucial for effective management.
Surgical treatment is the only effective therapy for these tumors.
Abstract
Oropharyngeal teratoma is a rare congenital tumor that grows slowly and can be suspected prenatally. It entails the obstruction of upper airway and upper digestive tract. Clinical examination is always completed by imaging particularly the MRI. We present a case of an eight- month -old infant who presented an oropharyngeal mass which caused intermittent dyspnea and feeding difficulties. The treatment is only surgical and histopathological examination confirms the diagnosis. Early diagnosis is key to successful management of oropharyngeal teratomas. •Oropharyngeal teratomas are rare congenital tumors.•Diagnosis is based on CT and MRI.•Early management is essential.•Treatment is surgical. Oropharyngeal teratomas are rare congenital tumors. Diagnosis is based on CT and MRI. Early management is essential. Treatment is surgical.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
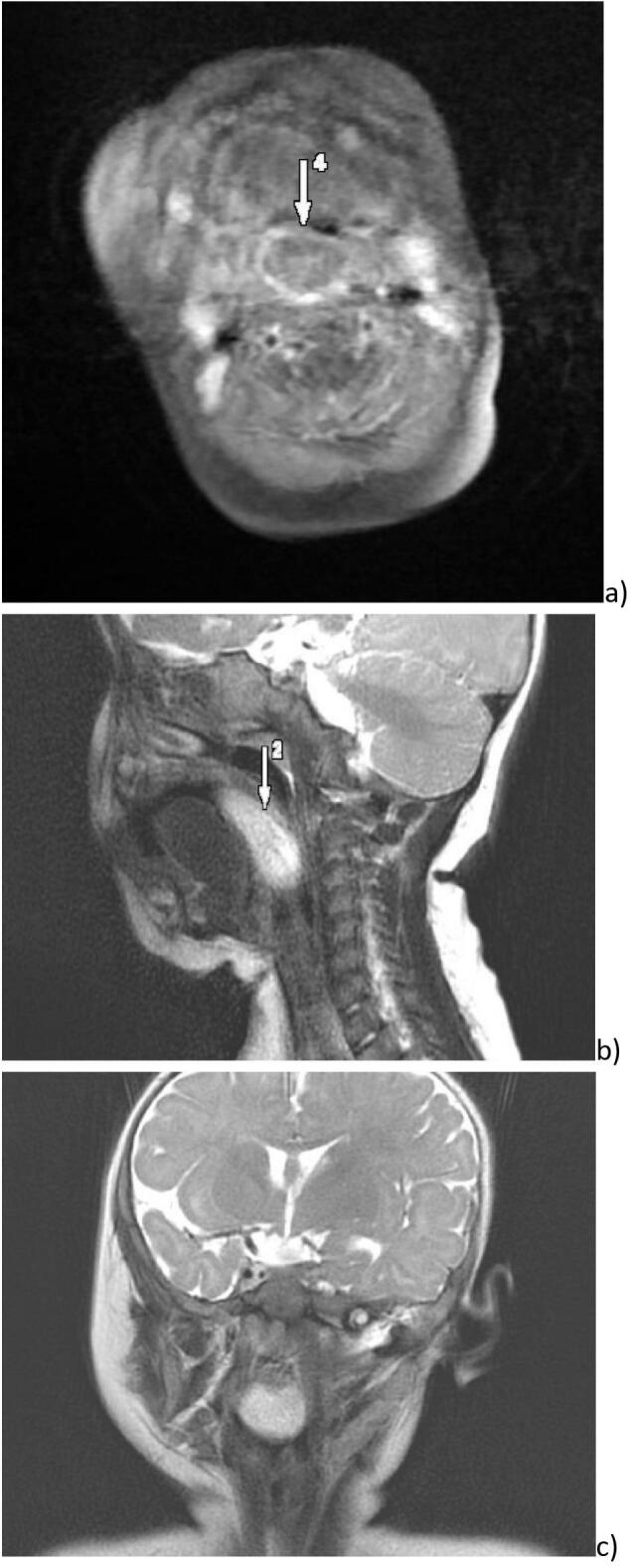 Figure 1
Figure 1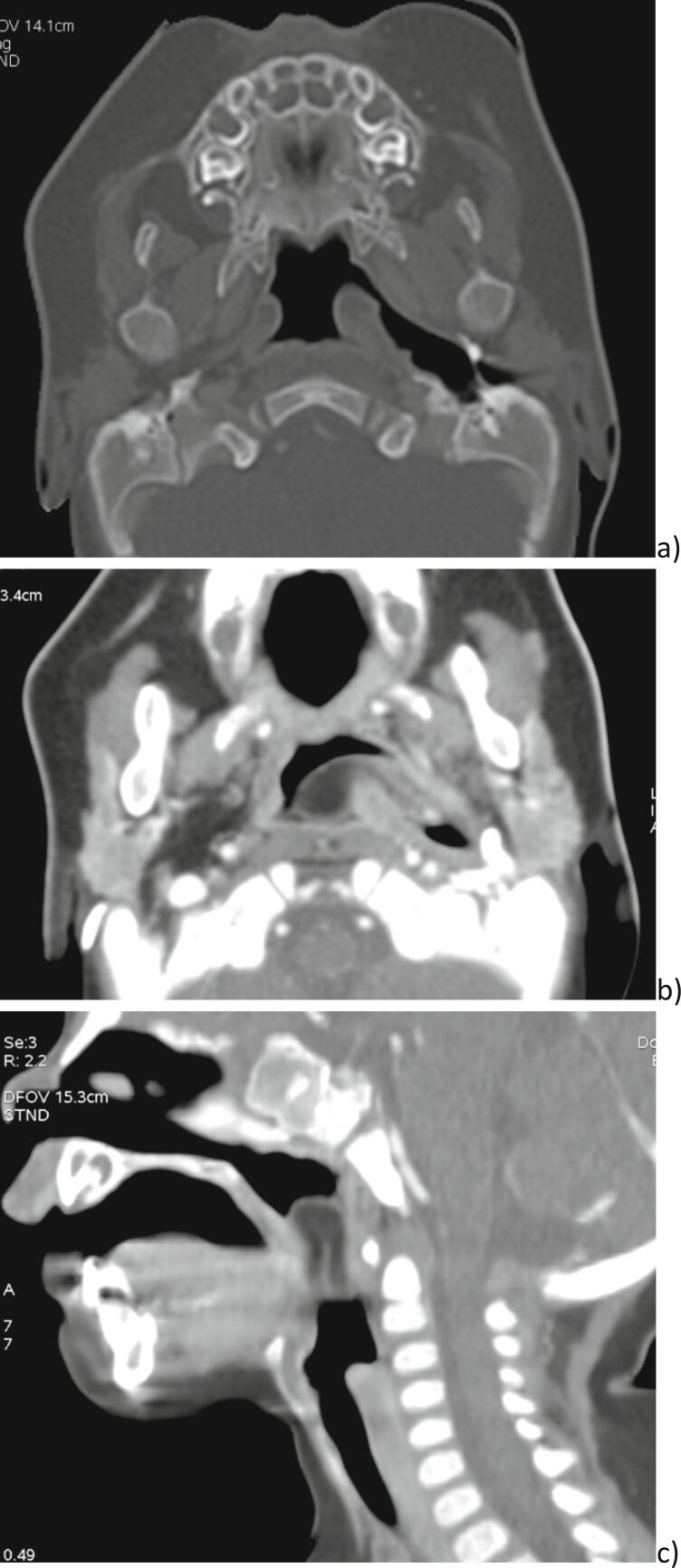 Figure 2
Figure 2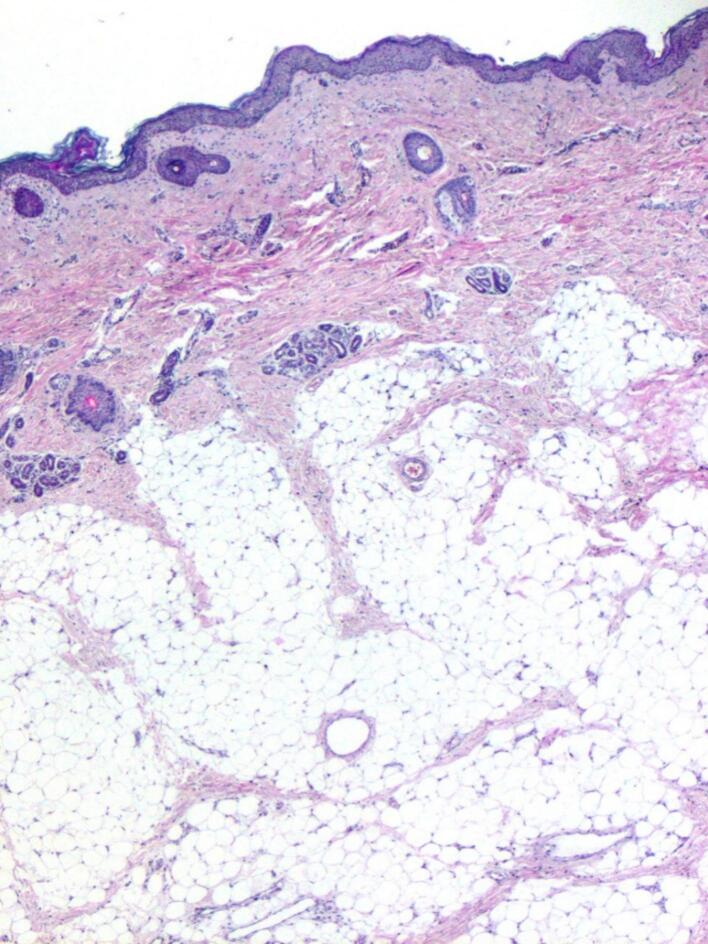 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTeratomas and Epidermoid Cysts · Tumors and Oncological Cases · Tracheal and airway disorders
Introduction
1
Teratoma is the most common infant neuronal congenital tumor, it represents 25 % of all benign and malignant tumors [1]. It usually develops in the sacrococcygeal region and only 6 to 10 % are located in the head and neck region, with a male female ratio from 1:6 to 1:3 [[1], [2], [3]]. It contains differentiated tissues foreign to the region in which it develops. The risk for head and neck localization is a partial or complete obliteration of the upper airway. The diagnosis can be made during the prenatal period thanks to recent advances in prenatal magnetic resonance imaging (MRI) [4] that allows to plan the surgical management of the newborn depending on the characteristics of the lesion. The work has been reported in line with the SCARE criteria [5].
Presentation of case
2
We report a case of an eight-month-old female infant who presented to our ENT emergencies with intermittent respiratory distress and difficulties to be fed. The symptoms were evolving for 2 months while she started to lose weight. On the first examination, there was no respiratory distress, there wasn't any cervical node, and systemic examination was normal. The oropharyngeal and endoscopic examination showed a voluminous protruding mass over the tongue, coming from the left pharyngeal wall. Otoscopy did not show any abnormalities. A Magnetic resonance imaging (MRI) was performed and showed an oropharyngeal tissular mass, measuring 51 ∗ 26 ∗ 14 mm (Fig. 1). It seemed to come from the base of the tongue. The mass was lobed, homogeneous, with a high intensity signal in T1 and T2 sequencies. The injection of gadolinium showed that it was vascularized.Fig. 1. Preoperative MRI in different sections a) axial, b) sagittal and c) coronal showing a well limited tissular lesion in hypersignal in the TWO sequences, this mass is filling the oropharynx.Fig. 1
We completed the examination with a Computed Tomography (CT-scan) that objectified a well-defined mass in the left parapharyngeal space measuring 30 ∗ 17 ∗ 8 mm. The lesion had a fat tissular CT density. The site of attachment was the left Eustachian tube. The mass was oblong, lying on the tongue. It spread in the hypopharyngeal space pushing in front the epiglottis and arriving in contact with the left arytenoid (Fig. 2). Tympanometry was normal.Fig. 2. Preoperative tomodensitometry aspect showing: a) a dilation of the left eutachian tube but without bone damage, b) a protrusing tissular mass well limited pediculated in the left eustachian tube where it is inserted, c) the tissular lesion filling the aerodigestive tract.Fig. 2
The treatment was strictly surgical with Rose's position, under complete anesthesia. Intraoperatively, we found a pale white pedunculated mass, measuring 3.5 cm, originating from the left lateral parapharyngeal wall. We completely resected the tumor along with its site of insertion through a transoral approach. A subsequent primary closure of the palatal defect was made.
The intervention proceeded without any complications.
Histopathological examination showed tissues derived from epidermal and mesodermal germ layers. The epidermal component comprised a squamous epithelium with pilosebaceous units covering the surface of the polypoid formation. The mesodermal derivate were predominantly adipose tissue, muscle, and cartilage. There was no evidence of immature neural elements. Overall, it was suggestive of a mature oropharyngeal teratoma (Fig. 3).Fig. 3. Histological aspect post operatively showing a polypoid mass covered by squamous epithelium with pilosebaceous units. Under this epithelium there was mainly adipose tissue (HE, ×100).Fig. 3
No complications such as infection or bleeding were reported following surgery. The infant was well breastfed, and her weight-loss curve improved. The MRI performed 6 months after surgery was normal and the patient didn't show signs of recurrence after a 4-year follow-up.
Discussion
3
Teratoma contains at least 2 of the three germinal layers that are ectoderm, mesoderm and endoderm. There are three types of teratoma: benign (contain mature tissues), mixed (immature tissue) and malignant. The last one represents a small quota [4]. However, even if they are benign, teratomas a can have serious repercussions and be life threatening such as in our case if the tumor had grown bigger. Oropharyngeal teratoma (also named epignathus) can present several symptoms depending on the size and the location, from all degrees of dyspnea, to feeding difficulties or just a mass discovered by the parents [4,6,7]. In our case, the patient didn't feed properly. In front of the potential gravity of the symptoms, prenatal diagnosis is essential. Therefore, fetal ultrasound combined with fetal MRI is important. The lesions are usually seen with the ultrasound in the late second and third semester of gestation [8,9]. The diagnosis is suspected in front of an elevated rate of alpha-fetoprotein, associated with a facial mass and polyhydramnios [9,10]. The prenatal MRI evaluates invasion of the brain, fetal airways, and precises the limits of the mass and its contact with the trachea and the umbilical cord [3,9,11]. All those elements allow to plan a tracheostomy (perinatal tracheostomy), or an EXIT (ex utero intrapartum treatment). CT-scan is not usually performed. This exam allows to eliminate bone involvement [3].
There is three surgical management possible for congenital teratomas: in utero procedure can be used for giant teratomas, on placenta support during EXIT intervention or postnatal.
EXIT is indicated when the lesion completely obstructs the airway tract, and during the procedure the neonate can be intubated or if it's not possible a tracheostomy is performed. Then EXIT intervention provides a safe control of the airway by removing the tumor, during placental support. This approach requires a multidisciplinary team involving ENT surgeon, pediatric surgeon, obstetrics, anesthesia and neonatology [12,13].
The prognosis of oropharyngeal teratoma is poor because of the airways obstruction [14]. It depends on the volume of the lesion and the involvement of essential structures.
Conclusion
4
Epignathi are not a common tumor. It should be diagnosed as early as possible. The treatment is strictly surgical. Earlier the lesion is highlighted more adapted will be the surgical management and complications as respiratory distress avoided.
Consent
Written informed consent was obtained from the patient's parents/legal guardian for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
This study is exempt from ethical approval at our institution (Habib Thameur Hospital, Tunis, Tunisia).
Funding
No fundings.
Author contribution
Dorra Chiboub: Writing - supervision.
Nadia Romdhane: Supervision.
Selima Jouini: Writing - Original draft.
Maya Cherif: Writing -Data collection.
Achraf Chedly: Supervision.
Chiraz Mbarek: Supervision.
Guarantor
Selima Jouini.
Conflict of interest statement
No conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moore S.W.SatgéD.Sasco A.J.Zimmermann A.Plaschkes J.The epidemiology of neonatal tumours Pediatr. Surg. Int.197Sep 1 20035095191452356810.1007/s 00383-003-1048-8 · doi ↗ · pubmed ↗
- 2Forrester M.B.Merz R.D.Descriptive epidemiology of teratoma in infants, Hawaii, 1986-2001 Paediatr. Perinat. Epidemiol.201Jan 200654581642034110.1111/j.1365-3016.2006.00678.x · doi ↗ · pubmed ↗
- 3Morof D.Levine D.Grable I.Barnewolt C.Estroff J.Fishman S.Oropharyngeal teratoma: prenatal diagnosis and assessment using sonography, MRI, and CT with management by ex utero intrapartum treatment procedure Am. J. Roentgenol.1832 Aug 20044934961526904610.2214/ajr.183.2.1830493 · doi ↗ · pubmed ↗
- 4Brodsky J.R.Irace A.L.Didas A.Watters K.Estroff J.A.Barnewolt C.E.Teratoma of the neonatal head and neck: a 41-year experience Int. J. Pediatr. Otorhinolaryngol.97Jun 201766712848325410.1016/j.ijporl.2017.02.011 · doi ↗ · pubmed ↗
- 5Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int. J. Surg. Lond. Engl.1095 May 1 20231136114010.1097/JS 9.0000000000000373 PMC 1038940137013953 · doi ↗ · pubmed ↗
- 6Zhu P.Li X.Y.Management of oropharyngeal teratoma: two case reports and a literature review J. Int. Med. Res.492Feb 202103000605219968710.1177/0300060521996873 PMC 791788533641494 · doi ↗ · pubmed ↗
- 7Kolekar S.S.Chincholi T.Nangare N.Patankar R.Oral teratoma Int. J. Appl. Basic Med. Res.61201654562695852410.4103/2229-516X.174015 PMC 4765276 · doi ↗ · pubmed ↗
- 8Cureus | Fetal oropharyngeal teratoma: prenatal diagnosis and imaging characteristics [Internet]. [cited 2022 Feb 4]. Available from: https://www.cureus.com/articles/43520-fetal-oropharyngeal-teratoma-prenatal-diagnosis-and-imaging-characteristics.10.7759/cureus.11329 PMC 771947733304667 · doi ↗ · pubmed ↗