Optical coherence tomography catheter-induced vasospasm of the left anterior descending artery: A case report
Fawaz Mohammed, Zaina Ali Khan, Muna Mohammed, Evan D. Gleaves, Cody Schwartz, Sajjad Haider, Sameer Saleem, Akhtar Amin, Jacqueline Dawson Dowe, Mohammed Abdul-Waheed, Muhammad Shoaib Akbar, Mohammed Kazimuddin, Rahil Rafeedheen

TL;DR
This case report describes a rare complication where an OCT catheter caused vasospasm in the left anterior descending artery, which was resolved with nitroglycerine.
Contribution
The novelty is the rare documentation of OCT catheter-induced vasospasm in the left anterior descending artery.
Findings
OCT catheter can induce vasospasm in the left anterior descending artery.
Nitroglycerine administration resolved the vasospasm in this case.
Abstract
Optical coherence tomography (OCT) helps identify coronary artery disease of different etiologies. Vasospasm from OCT catheter is a rarely reported complication that is more commonly seen in the right coronary artery. We report a case of OCT-catheter induced vasospasm of the left anterior descending artery that resolved with administration of nitroglycerine. Interventionalists need to weary of the occurrence of catheter-related coronary artery spasm to avoid stenting when not necessary.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
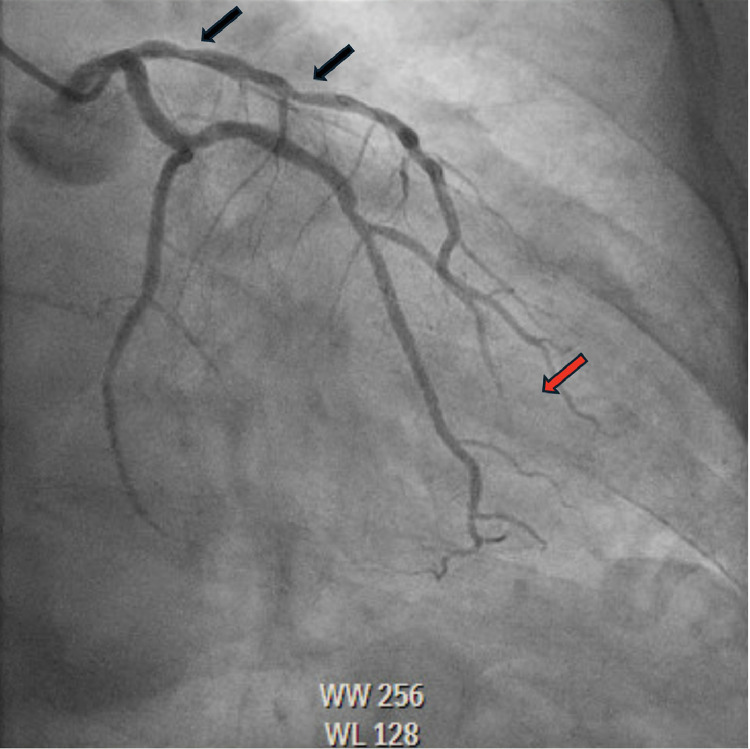 Figure 1
Figure 1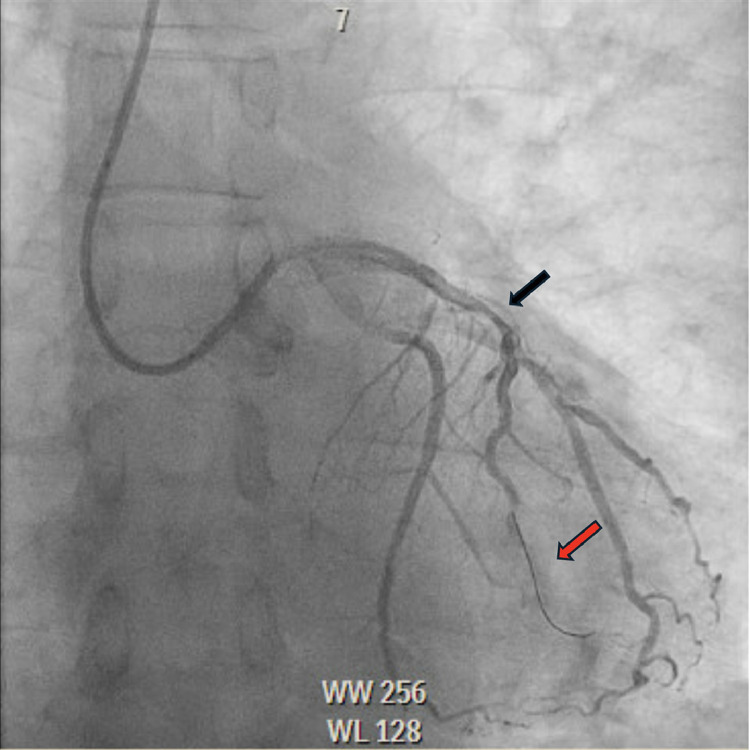 Figure 2
Figure 2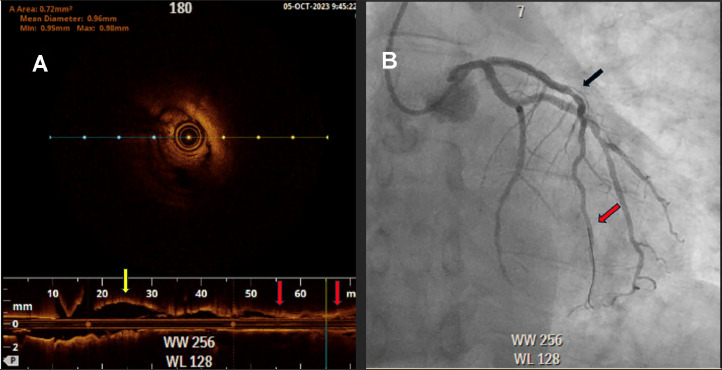 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOptical Coherence Tomography Applications · Intraoperative Neuromonitoring and Anesthetic Effects · Peripheral Artery Disease Management
Introduction
Optical coherence tomography (OCT) is used to identify and differentiate angiographic lesions in the coronary arteries from various phenotypes of coronary artery disease [1]. Coronary vasospasm is a rare complication of left heart catheterization, with an estimated occurrence of 0.75% [2]. More commonly this adverse event is seen in the right coronary artery although involvement of the left coronary arteries has been reported in the literature [3]. Spasms may involve multiple areas of a solitary coronary artery although cases of more than one artery being involved have also been described [3]. Catheter-induced coronary artery vasospasm is most discussed in the context of case reports; however, one retrospective study demonstrated an occurrence of 0.75% in the right coronary artery (RCA) [[2], [3], [4]]. In the setting of atherosclerotic disease, the diagnosis of catheter-induced coronary spams is often challenging, and interventionalists need to be cautious to mitigate risks from cardiovascular complications in diseased coronary arteries and avoid coronary revascularization in cases when not necessary [5]. Herein, we report a case of introduction of the OCT catheter inducing coronary vasospasm that resolved with administration of intracoronary nitroglycerine.
Case presentation
A 57-year-old male with past medical history significant for primary hypertension, pulmonary hypertension, ongoing tobacco abuse (1 pack per day of cigarettes) and mixed hyperlipidemia who had presented to the hospital with worsening substernal chest pain that was not associated with activity. He was treated medically with Amlodipine 5 mg daily, Atorvastatin 40 mg daily, Ranolazine 500 mg twice daily without improvement in symptoms. He was not treated with beta blockade due to baseline resting sinus bradycardia. He was brought to the cardiac catheterization laboratory for left coronary angiography to further evaluate the etiology of his chest pain. During coronary angiography a 70% lesion was noted in the proximal segment of the left anterior descending (LAD), followed by a 70% lesion in the mid segment (Fig. 1). Fractional Flow Reserve (FFR) was performed across the lesions with a result of 0.78 which was physiologically flow-limiting. A 3.0 × 20 mm balloon was advanced into the LAD, with multiple inflations performed through the proximal and mid LAD. A 3.25 × 38 mm drug-eluting stent was then deployed in the proximal to mid segments of the LAD, with OCT performed to evaluate strut apposition which revealed under expansion of the stent. A 3.5 × 50 mm noncompliant balloon was used for final expansion. Angiography postexpansion revealed a patent stent in the proximal to mid LAD without evidence of spasm (Fig. 2). OCT was reinserted and revealed a well-expanded and well apposed stent. Following OCT, spasm was noted in the LAD distal to the stent, this resolved with administration of 300 mcg of intracoronary nitroglycerin (Figs. 3A and B). There were no further complications during the procedure.Fig. 1. Coronary angiography showing severe stenosis of the proximal and mid left anterior descending artery (LAD) (Black arrows) prior to stent deployment without distal filling of the LAD (Red arrow).Fig 1. Fig. 2Coronary angiography showing coronary vasospasm of the mid LAD (Black arrows) after optical coherence tomography (OCT) catheter has been withdrawn without distal filling of the LAD (Red arrow).Fig 2. Fig. 3(A) OCT imaging of the LAD showing proximal portion without spasm (yellow arrow) along with coronary vasospasm (red arrows) which occurred following placement of the OCT catheter. A cross-sectional view of the spasmed artery is seen in the center of frame, (B) Coronary angiography post stent deployment and intracoronary nitroglycerin with resolution of coronary vasospasm (Black arrow) and distal filling of the LAD (Red arrow).Fig 3
Discussion
OCT is a technology that was first introduced in 1991 that uses the coherence of light to provide cross-sectional imaging of biological tissues by measuring optical reflections [1]. It has a high rate of reproducibility and low levels of energy used in the range of 5.0-8.0 mW, below what causes damage to tissue [6,7]. In one series of 468 patients, none had coronary artery vasospasm during OCT [7]. OCT has been used to differentiate the presence of coronary artery vasospasm versus atherosclerotic disease [7,8]. Catheter-induced vasospasm is a rarely reported complication. Studies are warranted to investigate whether there is some underlying genetic pathophysiology. Proposed mechanisms of catheter-induced coronary artery vasospasm include mechanical irritation, dysfunction of the endothelium, hyperactivity of the smooth muscles, and activation of cardiac stress receptors. Retrospective studies have showed that vast majority of catheter-related coronary spasms tend to occur in the right coronary artery (RCA) and majority of the patients also have concurrent vasospastic angina [2]. Sueda et al. conducted a multivariable analysis and found that a positive vasospasm test, young patients and diabetes were strong determinants for catheter-induced vasospasm. Their review also concluded that characteristics relating to the type and size of catheter used was not associated with catheter-induced vasospasms and interventionalists should rely more on the patient's clinical characteristics to predict this rare occurrence. History of tobacco use has been also reported as a risk for development of coronary vasosospasm in general [9]. Review of literature has also shown that patients who have a history of coronary artery spasms and Prinzmetal's angina are more likely to develop catheter-induced vasospasm therefore the use of calcium channel blocking agents and nitrate therapy has been proposed to be beneficial to these individuals [10]. Interventionalists need to be cognizant of coronary vasospasm from OCT catheters to avoid stenting of coronary arteries angiographically free of stenosis when not indicated. Intracoronary administration of nitroglycerine with OCT imaging is of utility when this occurs to best differentiate vasospasm secondary to different etiologies. A transthoracic echocardiogram can also help assess wall motion abnormalities from ischemic cardiomyopathy if present. The use of cardiac MRI for predicting long-term outcomes of OCT catheter-induced vasospasm needs to be investigated with studies in the future. Prospective studies are warranted to best identify what therapies can provide optimal care when OCT catheter-induced vasospasm is encountered.
Conclusion
OCT catheter-induced coronary artery vasospasm is a rare complication which most commonly occurs in the RCA, young, patients with diabetes, and tobacco users at highest risk. In our case, introduction of the OCT catheter caused vasospasm of the LAD, which resolved with administration of nitroglycerine. There is yet to be published case reports demonstrating coronary artery vasospasm in the LAD from this cause. This suggests further studies may reveal a heretofore unreported possible complication of OCT.
Author contributions
FM, ZAK, MM, EDG contributed to writing the original draft. CS, SH, SS, AA, JDD, MAW, MSA, MK, RR contributed to reviewing and editing the manuscript for important intellectual content and approval of the final manuscript.
Patient consent
Written, informed consent for publication of their case was obtained from the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Huang D Swanson EA Lin CP Schuman JS Stinson WG Chang W Optical coherence tomography Science 254503519911178118110.1126/science.19571691957169 PMC 4638169 · doi ↗ · pubmed ↗
- 2Sueda S Fujimoto K Sasaki Y Sakaue T Habara H Kohno H Catheter-induced spasm in the proximal right coronary artery Intern Med 5812019213010.2169/internalmedicine.1483-1830101945 PMC 6367073 · doi ↗ · pubmed ↗
- 3Esenboga K Baskovski E Ozyuncu N Tutar E Catheter-induced multiple non-proximal coronary spasm in a patient presenting with myocardial infarction Cureus 1232020 e 745610.7759/cureus.745632351835 PMC 7188002 · doi ↗ · pubmed ↗
- 4Ilia R Shimony A Cafri C Weinstein JM Angiographic characteristics of catheter-induced spasm of the left main coronary artery Am J Cardiol 1174201657157310.1016/j.amjcard.2015.11.03926721654 · doi ↗ · pubmed ↗
- 5Saeed S Flygel MLøland KH Packer E Catheter-induced vasospasm of the anatomically normal right coronary artery in a patient with non-st elevation myocardial infarction and obstructive disease in the left anterior descending artery; a challenging case report and review of the literature Curr Probl Cardiol 481202310143210.1016/j.cpcardiol.2022.10143236170909 · doi ↗ · pubmed ↗
- 6Prati F Regar E Mintz GS Arbustini E Di Mario C Jang IK Expert review document on methodology, terminology, and clinical applications of optical coherence tomography: physical principles, methodology of image acquisition, and clinical application for assessment of coronary arteries and atherosclerosis Eur Heart J 314201040141510.1093/eurheartj/ehp 43319892716 · doi ↗ · pubmed ↗
- 7Barlis P Gonzalo N Di Mario C Prati F Buellesfeld L Rieber JA multicentre evaluation of the safety of intracoronary optical coherence tomography Euro Intervention 512009909510.4244/eijv 5i 1a 1419577988 · doi ↗ · pubmed ↗
- 8Nakao M Matsuda J Iwai M Endo A Yonetsu T Otomo Y Coronary spasm and optical coherence tomography defined plaque erosion causing ST-segment-elevation acute myocardial infarction in a patient with COVID-19 pneumonia J Cardiol Cases 2322020878910.1016/j.jccase.2020.09.01233052252 PMC 7543701 · doi ↗ · pubmed ↗