Diagnostic Efficacy of Cell Block and Liquid-Based Cytology for Endoscopic Ultrasound-Guided Fine Needle Aspiration in Pancreatic Tumors
Ali Şenkaya, Ferit Çelik, Fatih Tekin, İlker Turan, Deniz Nart, Nevin Oruç, Ahmet Aydın

TL;DR
This study shows that combining cell block and liquid-based cytology improves the accuracy of diagnosing pancreatic tumors during EUS-FNA.
Contribution
The study demonstrates that combining cell block and liquid-based cytology significantly enhances diagnostic accuracy in pancreatic tumor detection.
Findings
Combined cell block and liquid-based cytology achieved 98% final diagnosis accuracy.
The combined method showed significantly higher accuracy than using either method alone (P < .001).
Malignancy was detected in 92.4% of cases using cell block alone and 87.9% using liquid-based cytology alone.
Abstract
This study aimed to evaluate the diagnostic efficacy of cell block (CB) and liquid-based cytology (LBC) for endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) in pancreatic tumors. The study included patients who underwent EUS-FNA for pancreatic tumors between January 2015 and February 2021 and whose cytology samples were both processed for LBC and CB. Data of 390 patients (220 men, mean age: 64.2 ± 11.4 years) were retrospectively analyzed. Of the detected lesions (size: 17-120 mm; mean: 39.9 ± 13.9 mm), 220 (56.4%) were located in the head and uncinate process of the pancreas. Lesions in 339 (86.9%) patients were diagnosed as malignant using CB and/or LBC and suspicious for malignancy in 44 (11.3%) patients. In 7 patients with non-diagnostic (6 cases) or negative for malignancy (1 case) EUS-FNA results using both methods, the diagnosis of malignancy was established via…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1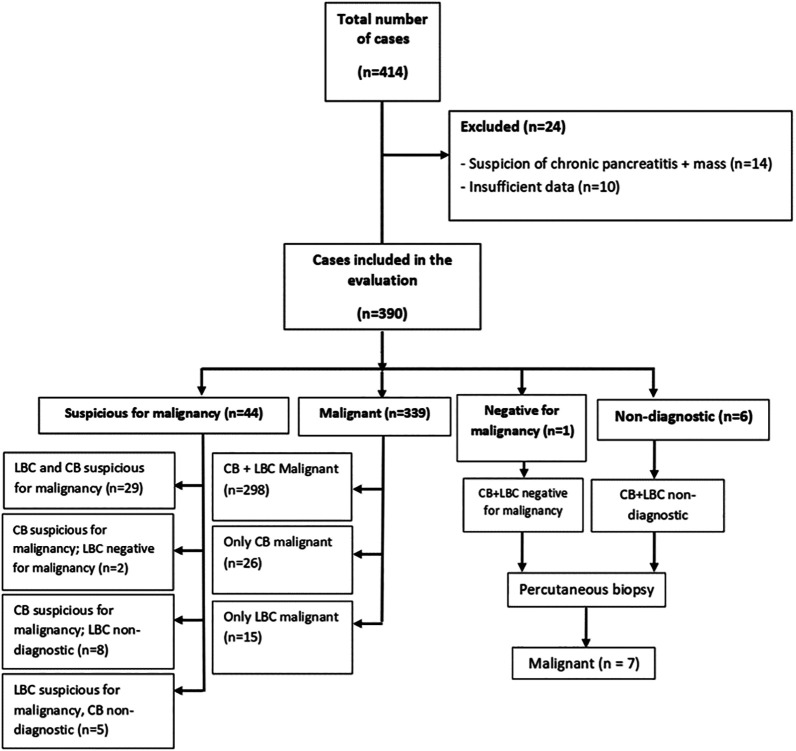 Figure 2
Figure 2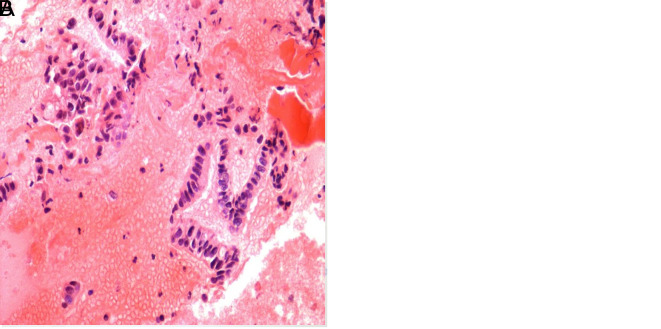 Figure 3
Figure 3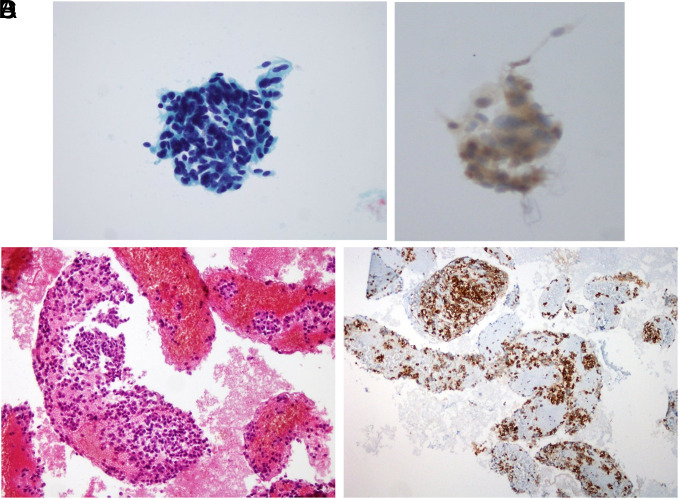 Figure 4
Figure 4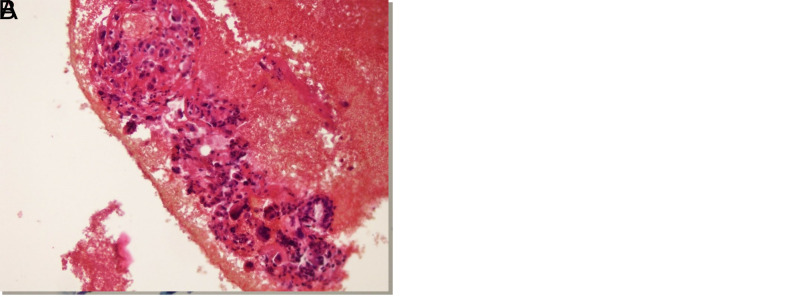 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Neuroendocrine Tumor Research Advances · Cancer Genomics and Diagnostics
Introduction
Endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) is widely used in the cytopathological diagnosis of pancreatic tumors.^1,2^ Recently, EUS-FNA was reported to have a sensitivity, specificity, and diagnostic accuracy of 85%-98%, 95%-100%, and 91%-98%, respectively, for pancreatic solid tumors.^3,4^ The diagnostic performance of EUS-FNA cytology varies depending on the experience of the clinician performing endoscopy and cytopathology, availability of a cytopathology expert for rapid on-site evaluation (ROSE), lesion characteristics, and evaluation method.^3,5^ Although performing ROSE significantly increases the diagnostic value, it is not feasible in many centers.^6^ Needles of different shapes have been developed for fine needle biopsy (FNB) to obtain samples showing tissue structure^7^ and overcome inadequacies in tissue diagnosis. Some studies showed significantly better diagnostic performance of FNB over FNA in pancreatic lesions; however,^8-12^ the application of FNB needles is limited by their unavailability in every center.
Smear cytology (SC), liquid-based cytology (LBC), and cell block (CB) preparation are commonly used techniques to analyze specimens obtained using EUS-FNA. Liquid-based cytology allows automated slide preparation based on filtration with a uniform, monolayer distribution of cells. Liquid-based fixatives remove red blood cells, mucus, and protein deposits in the background.^13^ Reportedly, CB has a greater contribution to the diagnosis than any method alone, and the application of immunocytochemistry is remarkably useful.^14,15^
In our clinic, both CB and LBC are routinely used for testing pancreatic tumor samples collected via EUS-FNA. This study aimed to compare both methods and evaluate their contribution in the diagnosis of pancreatic malignancies.
Materials and Methods
Patients who met the following criteria were included in this study: patients aged ≥18 years who underwent EUS-FNA for the diagnosis of pancreatic malignancy in the Endoscopy Unit of the Gastroenterology Department of Ege University Medical Faculty Hospital between January 2015 and February 2021 and whose cytology specimens were both fixed in a special solution for LBC and in alcohol–formalin solution for CB preparation and sent to the pathology laboratory for analyses. Patients who underwent EUS-FNA for purely cystic lesions and those with insufficient data were excluded from the study. The patients’ age, sex, lesion size and location in the pancreas, and pathology results (both LBC and CB) were recorded by searching the hospital database.
A linear echoendoscope (EG 530 UT Fujifilm, Japan or UCT180, Olympus, Center Valley, Pa, USA with Hitachi Aloka Alpha 7 system, Tokyo, Japan) was used for the procedure. Informed consent was obtained from the patients, and the procedure was initiated by sedating the patients after 12 hours of fasting. The coagulation parameters were checked before performing the procedure. Standard 22-gauge needles (Boston Scientific, Natick, Mass, USA or Wilson-Cook, Winston-Salem, NC, USA) were used for EUS-FNA. In each case, material was taken from the existing lesions by performing 2-4 passes (mean, 3) during EUS-FNA. The material was transferred to a tube containing ThinPrep fixation solution [CytoLyt (Cytyc Corp - Boxborough, Mass, USA)] for LBC and alcohol–formalin solution for CB and sent to the pathology laboratory. For LBC, the material in CytoLyt solution was prepared using a ThinPrep5000 automated slide processor (Hologic, Marlborough, Mass, USA). All slides were stained with Papanicolaou stain. The cytologic material fixed in alcohol–formalin was first directly centrifuged. Approximately, 10 mL of material was pipetted from the bottom of the cytologic material into a Falcon tube, and the entire sample was collected if the volume was <10 mL. After adding 25-30 mL of 96% alcohol and 10% formaldehyde in equal proportions, centrifugation was performed at 1660 rpm for 10 minutes. After centrifugation, the supernatant was discarded. The alcohol–formalin mixture was subsequently added again, and the tube was left for a few hours to allow precipitate formation. The precipitate was collected in a tissue cassette and subjected to tissue analysis. Sections of 4 microns were taken from the obtained paraffin blocks and stained with hematoxylin and eosin, and histopathological examination was performed. Cytopathological examinations were performed by an experienced cytopathologist, more than 10 years, blindly.
The pathology results of the patients were classified according to the classification of the Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology (PSCPC). According to this system, category I is non-diagnostic, II is negative (for malignancy), III is atypical, IV is neoplastic: benign or other, V is suspicious for malignancy, and VI is positive/malignant.^16^
Approval was obtained from the Ege University Ethics Committee (approval number: 21-5T/107, date: May 20, 2021) before starting the study. This study was conducted in accordance with the principles of the Declaration of Helsinki on Human Rights.
Statistical Analysis
The Statistical Package for the Social Sciences 25.0 program (IBM Corp., Armonk, NY, USA) was used for the analysis of variables. Conformity of data to normal distribution was evaluated using Shapiro–Wilk and Shapiro–Francia tests, and homogeneity of variance was evaluated using Levene’s test. To compare the 2 independent groups according to quantitative data, the Mann–Whitney U-test was used in combination with the Monte Carlo method. The categorical variables were compared using Pearson’s chi-square, Fisher Exact, and Fisher–Freeman–Halton tests along with the Monte Carlo simulation technique. Furthermore, the column ratios were compared with each other and analyzed using the Benjamini–Hochberg method with adjusted P-value results. Quantitative variables were expressed as mean (± standard deviation), median (minimum/maximum), and median [percentile 25 (q1)/ percentile 75 (q3)], whereas categorical variables were expressed as n (%). Variables were analyzed at a 95% confidence level, and P <.05 indicated statistical significance.
Results
Overall, 14 patients were excluded because they underwent EUS-FNA for the analysis of suspected mass based on their diagnosis of chronic pancreatitis and no malignancy was detected; furthermore, 10 patients were excluded because of insufficient data. The results of these 14 patients were discussed in a multidisciplinary hepatobiliary council and a consensus was reached that malignancy was absent and no findings indicating malignancy were detected in at least 12 months of follow-up. After excluding these cases, the data of 390 patients (220 [56.4%] male; 170 [43.5%] female; mean age, 64.2 [22–87] years) who met the inclusion criteria were retrospectively analyzed. The demographic and clinical characteristics of the patients and the CB/LBC results are shown in Table 1.
Of the 390 patients who underwent EUS-FNA, the lesions in 339 (86.9%) were cytologically diagnosed as malignant. Notably, lesions in 298 (87.9%) patients were diagnosed as malignant using both CB and LBC. Furthermore, lesions were diagnosed as malignant in 26 (7.7%) patients using CB alone and in 15 (4.4%) using LBC alone. Lesions diagnosed as malignant via CB alone were found to have different results when diagnosed using LBC alone: 2 were negative for malignancy, 14 were non-diagnostic, and 10 were suspicious for malignancy. However, lesions in 15 patients diagnosed as malignant via LBC were diagnosed as non-diagnostic using CB. Notably, the lesions in 44 (11.3%) patients could not be diagnosed as malignant by either CB or LBC. Suspicious for malignancy was diagnosed in 29 patients using both CB and LBC. Additionally, lesions in 2 patients were diagnosed as suspicious for malignancy using CB and negative for malignancy using LBC. Furthermore, lesions in 8 patients were diagnosed as suspicious for malignancy using CB and non-diagnostic using LBC, and those in 5 patients were diagnosed as suspicious for malignancy using LBC and non-diagnostic using CB. Suspicious for malignancy detected using CB and/or LBC was diagnosed in inoperable patients with locally advanced stage and/or distant metastasis. These cases were evaluated by a multidisciplinary hepatobiliary council using clinical, laboratory, and imaging findings and were considered malignant. Consequently, these patients were referred to the oncology department for treatment. Seven patients were diagnosed as malignant via ultrasound-guided percutaneous biopsy after EUS-FNA results were inconclusive in 6 cases and benign in one case using both methods (Figure 1).
To reveal the possible effects of suspicious for malignancy on the comparison results, statistical analyses were performed by considering cases with suspicion for malignancy as malignant and subsequently excluding those cases. In both the aforementioned scenarios, the use of both CB and LBC significantly enhanced the diagnostic accuracy compared with the use of CB and LBC alone (P < .001). When patients with suspicious for malignancy were considered malignant, the diagnostic accuracy of CB was slightly higher than that of LBC (P = .045) (Table 2).
In the statistical evaluation of the diagnostic accuracies obtained using both methods in relation to the patients’ age, sex, size, pancreatic location, and sonographic appearance of the lesion, no significant difference was observed in parameters other than age (Table 3). Statistical evaluation of CB and LBC separately in terms of age, sex, lesion size and location in the pancreas, and sonographic appearance revealed a significant correlation between LBC diagnostic accuracy and age and sonographic appearance of the lesion. The diagnostic accuracy of LBC was significantly higher for solid tumors than for solid-cystic tumors (P = .031) (Table 4).
Although most patients (73% and 72.1% who underwent CB and LBC, respectively) were diagnosed with pancreatic adenocarcinoma, 17 were diagnosed with neuroendocrine tumor, 5 with lung adenocarcinoma metastasis, 3 with diffuse large B-cell lymphoma, 2 with solid pseudopapillary neoplasia, 1 with renal cell carcinoma metastasis, 1 with gastrointestinal stromal tumor, and 1 with malignant metastatic melanoma (Figures 2-4).
Discussion
Despite the increasing use of FNB for EUS-guided tissue acquisition, FNA continues to be an important and valuable technique because of the disadvantages of FNB, including its lack of availability in many centers and high price. In this study, we evaluated the diagnostic efficacy of CB and LBC in EUS-FNA for diagnosing pancreatic tumors and found that the combined use of both methods resulted in higher diagnostic accuracy than the use of CB and LBC alone (P < .001). Notably, in cases where lesions in patients with suspicious for malignancy were considered malignant, a separate analysis was performed. This analysis also revealed that the combined use of both methods increased the diagnostic accuracy (P < .001) (Table 2).
Early detection of pancreatic cancer significantly affects its treatment and prognosis. The chances of surgical resection and survival rates decrease with advancements in tumor stage and size.^17^ The diagnostic sensitivity of cytologic and/or histologic specimens obtained from pancreatic lesions using EUS-FNA is affected by the experience of the endoscopist performing the procedure, the experience of the pathologist evaluating the specimen, the characteristics of the lesion (size/location), and the size and shape of the fine needle through which the specimen is taken. The procedure used for sample processing and the quality of the sample slides (cellular overlap, dryness, blood cells, and contamination) are the most important factors that affect the sensitivity.^18-20^ Diagnostic sensitivity, specificity, and accuracy of EUS-FNA in pancreatic solid tumors are 85%-98%, 95%-100%, and 91%-98%, respectively.^3,4^ In this study, the combined use of CB and LBC yielded a diagnostic accuracy of 98% when the results of the patients with suspicious for malignancy were excluded and 98.2% when the patients with suspicious for malignancy were considered malignant. Furthermore, these results were similar to those reported in the literature.
Smear cytology, a traditional and standard method for cytologic diagnosis, and performing ROSE significantly reduces the number of inconclusive samples, increasing diagnostic sensitivity and overall accuracy.^18,21,22^ However, in many developing countries, it is difficult to have an on-site cytopathologist for every patient due to financial constraints. Liquid-based cytology requires less skill than conventional SC preparation and offers favorable cellular preservation. Liquid-based cytology has been accepted as the preferred specimen collection method in the absence of ROSE because it is easy to use and has a diagnostic accuracy equivalent to that of SC prepared with ROSE,^22^ even when performed by endoscopists who are still learning.^13,23^ However, LBC is a thin-layer slide preparation method, and it is particularly advantageous for cytopathologic evaluation because it overcomes the disadvantages of SC including cell crowding and blood contamination, reveals more cellularity with a cleaner background and better cytomorphologic features, and can be used to conduct immunocytochemistry and molecular biology studies.^21,24-27^ In this study, the diagnostic accuracy of LBC was 87.9% and 89% when cases with suspicion for malignancy were excluded and considered malignant, respectively. Some studies reported diagnostic accuracy up to 88-90.2% by LBC.^28,29^ Our results are correlated with the published literature.
Pathologists prefer CB over cytologic specimens because the artifact rate is lower in CB than in SC and the appearance of CB is much closer to the actual tissue architecture.^30^ Moreover, CB is more suitable than SC and LBC for immunohistochemical applications and is considered the gold standard of histological staining.^31,32^ However, CB samples are often fragmented and small and are rarely sufficient to establish a diagnosis when used alone.^33^ Therefore, the use of additional methods contributes to increased diagnostic accuracy. In this study, the diagnostic accuracy of CB alone was 92.4% when cases with suspicion for malignancy were excluded and 93.1% when they were considered malignant. When combined with LBC, the diagnostic accuracy of the two methods reached 98%. In 15 (4.4%) cases where CB was non-diagnostic and/or misdiagnosed, the correct diagnosis was achieved using LBC. Qin et al^34^ evaluated the diagnostic accuracy of CB, SC, and LBC (91.7%, 75%, and 77.8%, respectively) and reported that CB was superior to other methods and neither the combination of CB and SC nor CB and LBC increased diagnostic accuracy. However, the results of this study demonstrated that the diagnostic accuracy increased with the combined use of both methods.
In this study, the diagnostic accuracy of LBC was significantly lower in solid-cystic lesions than in solid lesions (P = .031). This highlighted the diagnostic challenges arising from the presence of necrotic cells in the cystic degeneration areas of solid tumors; furthermore, a combination of both methods would be recommended in these cases. In this study, 6.7% and 6.9% of the samples collected for CB and LBC, respectively, had cellular deficiency, which was lower than the deficiency rates found in SC, CB, and LBC samples (12.5%, 33.3%, and 41.7%, respectively) reported by Yeon et al.^35^
Combined use of LBC with CB is also found to be useful in the diagnosis of many other diseases, such as oral diffuse large B cell lymphoma, endometrial lesions, papillary thyroid carcinoma, and evaluation of peritoneal fluid in gynecologic malignancies. Therefore, the usage of combined cytopathological techniques should be increased in pancreatic disorders.^36-39^
Limitations of the present study are its retrospective nature and single-center study.
In conclusion, LBC and CB are equally important for the diagnosis of pancreatic tumors in patients undergoing EUS-FNA. The diagnostic accuracy of the combined use of both methods was significantly higher than that of LBC and CB alone. This is particularly important in centers where ROSE cannot be performed. The use of LBC in combination with CB may be considered a favorable choice to increase the diagnostic accuracy and reduce loss of time.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agarwal B Krishna NB Labundy JL Safdar R Akduman EI . EUS and/or EUS-guided FNA in patients with CT and/or magnetic resonance imaging findings of enlarged pancreatic head or dilated pancreatic duct with or without a dilated common bile duct. Gastrointest Endosc. 2008;68(2):237 335. (10.1016/j.gie.2008.01.026)18423464 · doi ↗ · pubmed ↗
- 2Volmar KE Vollmer RT Jowell PS Nelson RC Xie HB . Pancreatic FNA in 1000 cases: a comparison of imaging modalities. Gastrointest Endosc. 2005;61(7):854 861. (10.1016/s 0016-5107(05)00364-0)15933687 · doi ↗ · pubmed ↗
- 3Sugiura R Kuwatani M Hirata K , et al. Effect of pancreatic mass size on clinical outcomes of endoscopic ultrasound-guided fine-needle aspiration. Dig Dis Sci. 2019;64(7):2006 2013. (10.1007/s 10620-018-5435-3)30604374 · doi ↗ · pubmed ↗
- 4Hewitt MJ Mc Phail MJ Possamai L Dhar A Vlavianos P Monahan KJ . EUS-guided FNA for diagnosis of solid pancreatic neoplasms: a meta-analysis. Gastrointest Endosc. 2012;75(2):319 331. (10.1016/j.gie.2011.08.049)22248600 · doi ↗ · pubmed ↗
- 5Matsubayashi H Sasaki K Ono S , et al. Pathological and molecular aspects to improve endoscopic ultrasonography-guided fine-needle aspiration from solid pancreatic lesions. Pancreas. 2018;47(2):163 172. (10.1097/MPA.0000000000000986)29346217 · doi ↗ · pubmed ↗
- 6Hébert-Magee S Bae S Varadarajulu S , et al. The presence of a cytopathologist increases the diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration cytology for pancreatic adenocarcinoma: a meta-analysis. Cytopathology. 2013;24(3):159 171. (10.1111/cyt.12071)23711182 PMC 4159090 · doi ↗ · pubmed ↗
- 7Varadarajulu S Tamhane A Eloubeidi MA . Yield of EUS-guided FNA of pancreatic masses in the presence or the absence of chronic pancreatitis. Gastrointest Endosc. 2005;62(5):728 753. (10.1016/j.gie.2005.06.051)16246688 · doi ↗ · pubmed ↗
- 8Wong T Pattarapuntakul T Netinatsunton N , et al. Diagnostic performance of endoscopic ultrasound-guided tissue acquisition by EUS-FNA versus EUS FNB for solid pancreatic mass without ROSE: a retrospective study. World J Surg Oncol. 2022;20(1):215. (10.1186/s 12957-022-02682-3)35751053 PMC 9229075 · doi ↗ · pubmed ↗