Ultrasound Imaging of Ankle Retinacula: A Comprehensive Review
Carmelo Pirri, Nina Pirri, Veronica Macchi, Andrea Porzionato, Raffaele De Caro, Carla Stecco

TL;DR
This paper reviews how ultrasound imaging can help diagnose ankle retinacula injuries, which are often missed or misdiagnosed.
Contribution
The study systematically reviews ultrasound techniques for assessing ankle retinacula and highlights their potential in clinical diagnosis.
Findings
Ultrasound imaging provides static and dynamic insights into ankle retinacula pathology.
Advanced ultrasound techniques show promise for diagnosing retinacular injuries.
Understanding normal anatomy is crucial for accurate ultrasound-based diagnosis.
Abstract
The retinacula of the ankle are specialized anatomical structures characterized by localized thickenings of the crural fascia that envelop the deep components of the lower leg, ankle and foot. The ankle retinacula include the extensor retinacula, the peroneal retinacula and flexor retinaculum. Despite their potential to explain persistent and unexplained pain following an injury, these structures are often overlooked or incorrectly diagnosed. Hence, this comprehensive review was performed aiming to investigate the use and the methodology of US imaging to assess ankle retinacula. The search was performed on PubMed and Web of Science databases from inception to May 2024. The MeSH keywords used were as follows: “Ankle Retinacula”, “Foot Retinacula”, “Superior extensor retinaculum”, “Inferior extensor retinaculum”, “peroneal retinaculum”, “superior peroneal retinaculum”, “inferior peroneal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
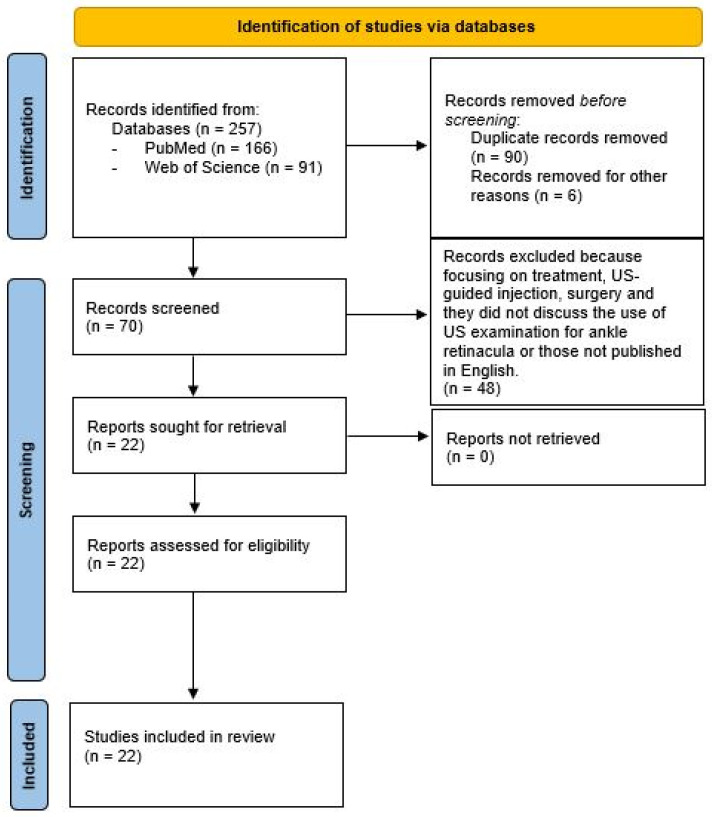 Figure 1
Figure 1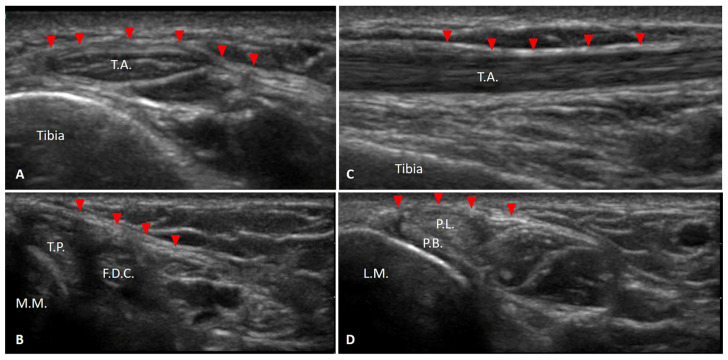 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFoot and Ankle Surgery · Tendon Structure and Treatment · Sports injuries and prevention
1. Introduction
Musculoskeletal ultrasound (MSK US) imaging plays a pivotal role in the diagnosis and management of musculoskeletal disorders [1]. Additionally, MSK US is a non-invasive, radiation-free and cost-effective tool, making it accessible for routine use in clinical practice [1]. Its utility extends to guiding therapeutic interventions such as US-guided injections [1]. Overall, MSK US imaging is indispensable for accurate, timely diagnosis, effective management of a wide range of musculoskeletal conditions, and the study of different anatomical structures [1].
This imaging modality offers high-resolution visualization of soft tissues, including muscles, tendons, ligaments, nerves, joints and fasciae [1], providing detailed anatomical and pathological information. Its real-time capability enables dynamic assessment of structures during movement, which is particularly useful for evaluating tendon gliding, detecting subluxations, diagnosing impingements, etc. [2,3].
In this era of high-definition US imaging, another structure that is garnering increased attention is the ankle retinacula [4,5]. Recent research underscores the critical role of the ankle retinacula in proprioceptive feedback and the functional stability of the ankle [6,7,8]. Retinacula are localized thickenings of the deep/muscular fascia that keep tendons in place during muscle contraction, thereby preventing bowstringing [4]. The high mechanical stress in the ankle during sport activities, coupled with frequent acute trauma and repetitive microtrauma, leads to common yet underreported disorders of the ankle retinacula in clinical practice [9,10,11]. Ultrasound (US) imaging is particularly effective in visualizing ankle retinacula due to their superficial location and the high spatial resolution of US imaging [9]. Moreover, dynamic US imaging can effectively demonstrate intermittent tendon dislocations caused by retinacular failure [9,10,11]. The retinacula are anatomically structured into three unique histological layers: an inner gliding layer rich in hyaluronic acid-secreting cells; a substantial middle layer composed of collagen bundles, fibroblasts and elastin fibers all interwoven; and an outer layer of loose connective tissue containing vascular channels [8]. Injuries to the retinacula are predominantly linked to ankle sprains, generally induced by a sudden and vigorous traction of the neighboring tendons caused by intense muscle contraction [10]. Although less frequent, microtraumatic lesions of the retinacula can also arise in the context of sport activities [10].
Despite the clear advantages of US imaging in diagnosing ankle retinacula injuries, there is a notable gap in the literature concerning a comprehensive overview of the methodology, use and reliability of US imaging in this context. Existing studies often highlight the immediate diagnostic capabilities of US, yet they seldom provide an in-depth analysis of the protocols, parameters and techniques that enhance its effectiveness and reliability. Addressing these gaps through detailed methodological reviews and reliability assessment could significantly advance the clinical utility of US imaging, offering physicians a more thorough understanding of its strengths and limitations in diagnosing and managing ankle retinacula injuries. Hence, this comprehensive review was performed aiming to firstly investigate the use and the methodology of US imaging to assess pathologic and healthy ankle retinacula, and secondly to assess the reliability of US imaging in ankle retinacula assessment.
2. Materials and Methods
2.1. Data Sources
We performed a systematic literature review adhering to the Preferred reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. This systematic review protocol is registered in Open Science Framework registries with the registration https://doi.org/10.17605/OSF.IO/UVBRC (accessed on 2 June 2024). The search of the literature was guided by PICO (Problem/Patient; Intervention/Indicator; Comparison and Outcome) (Table 1).
Our search was conducted on the PubMed and Web of Science databases, covering publications from their inception until May 2024. Additionally, we meticulously examined the references of the included studies to identify any further relevant publications. The MeSH keywords employed were “Ankle Retinacula”, “Foot Retinacula”, “Superior extensor retinaculum”, “Inferior extensor retinaculum”, “peroneal retinaculum”, “superior peroneal retinaculum”, “inferior peroneal retinaculum”, “flexor retinaculum”, “Ultrasound Imaging”, “Ultrasound”, “Ultrasonography” and “Ultrasound examination”. The search strategy was structured as follows: (“Ankle retinacula”) OR (“ankle retinacula” AND “Ultrasound Imaging”) OR (“ankle retinacula” AND “Ultrasound”) OR (“ankle retinacula” AND Ultrasonography”) OR (“ankle retinacula” AND “Ultrasound examination”) OR (“Foot Retinacula”) OR (“Foot Retinacula” AND “Ultrasound Imaging”) OR (“Foot Retinacula” AND “Ultrasound”) OR (“Foot Retinacula” AND Ultrasonography”) OR (“Foot Retinacula” AND “Ultrasound examination”) OR (“Superior extensor retinaculum”) OR (“Superior extensor retinaculum” AND “Ultrasound Imaging”) OR (“Superior extensor retinaculum” AND “Ultrasound”) OR (“Superior extensor retinaculum” AND Ultrasonography”) OR (“Superior extensor retinaculum” AND “Ultrasound examination”) OR (“Inferior extensor retinaculum”) OR (“Inferior extensor retinaculum” AND “Ultrasound Imaging”) OR (“Inferior extensor retinaculum” AND “Ultrasound”) OR (“Inferior extensor retinaculum” AND Ultrasonography”) OR (“Inferior extensor retinaculum” AND “Ultrasound examination”) OR (“peroneal retinaculum”) OR (“peroneal retinaculum” AND “Ultrasound Imaging”) OR (“peroneal retinaculum” AND “Ultrasound”) OR (“peroneal retinaculum” AND Ultrasonography”) OR (“peroneal retinaculum” AND “Ultrasound examination”) OR (“superior peroneal retinaculum”) OR (“superior peroneal retinaculum” AND “Ultrasound Imaging”) OR (“superior peroneal retinaculum” AND “Ultrasound”) OR (“superior peroneal retinaculum” AND Ultrasonography”) OR (“superior peroneal retinaculum” AND “Ultrasound examination”) OR (“inferior peroneal retinaculum”) OR (“inferior peroneal retinaculum” AND “Ultrasound Imaging”) OR (“inferior peroneal retinaculum” AND “Ultrasound”) OR (“inferior peroneal retinaculum” AND Ultrasonography”) OR (“inferior peroneal retinaculum” AND “Ultrasound examination”) OR (“flexor retinaculum”) OR (“flexor retinaculum” AND “Ultrasound Imaging”) OR (“flexor retinaculum” AND “Ultrasound”) OR (“flexor retinaculum” AND Ultrasonography”) OR (“flexor retinaculum” AND “Ultrasound examination”).
2.2. Study Selection and Searchers
Studied were included if they (1) used US imaging in the evaluation of ankle retinacula; (2) used US imaging to diagnose a pathology of ankle retinacula; (3) were published and conducted within the Table 1 criteria; and (4) were published in the English language. Exclusion criteria were applied to filter out peripheral content, maintaining a focus on primary research while including review papers and case reports. The exclusion criteria were (1) papers centered on treatment; (2) studies focused on US-guided injections; (3) studies on surgery; (4) papers that did not discuss US imaging for ankle/foot retinacula; and (5) non-English publications.
Our screening process involved reviewing title and abstracts, followed by a full-text review of eligible studies. References were also checked to identify any additional publications. The literature search was conducted by one reviewer (N.P.) and verified by a senior researcher (C.P.) with ten years of experience. Any discrepancies were resolved through consensus among the authors (Figure 1).
2.3. Data Extraction
Data concerning these parameters were collected and analyzed:
- General characteristic of the paper: first author, year of publication, study design;
- Study population characteristics: number of patients or healthy volunteers, age, gender and ankle/foot retinacula status;
- Measurement methods: type of probe, type of US imaging, positions of patients or healthy volunteers;
- Reliability;
- Outcomes: evaluated parameters.
2.4. Risk of Bias
Two researchers assessed the quality of the studies, resolving any discrepancies through discussion. The evaluation of the papers utilized the Newcastle–Ottawa Scale (NOS), specifically tailored for both observational and case–control studies. Meanwhile, case-report studies were appraised using the JBI Critical Appraisal Checklist for Case Reports.
3. Results
A meticulous analysis was conducted on papers selected specifically for their relevance to the US imaging of ankle retinacula, encompassing both patient cases and studies involving healthy volunteers. The degree of consensus among the authors regarding the inclusion of the articles was remarkably high, demonstrated by a Cohen’s kappa value of 0.92. The essential attributes of the selected studies, spanning from 1974 to 2024, are succinctly outlined in Table 1 [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31]. In total, 257 records underwent screening, resulting in the removal of 90 duplicates and the exclusion of six further records. Subsequently, the textual content of the remaining 70 potentially eligible papers was meticulously reviewed, leading to the exclusion of 48 papers that did not align with our predefined inclusion criteria. Ultimately, 22 studies met the criteria for inclusion. The schematic representation of our study process is depicted in Figure 1 and Table 2.
3.1. General Characteristics of Studies
According to their methodological design, most of the papers included in this review were review studies (n = 8) [5,13,14,21,22,24,25,26]. The other studies were cross-sectional studies (n = 2) [10,11], case report or case series (n = 6) [12,14,15,17,28,30], cohort studies (n = 2) [16,30], retrospective studies (n = 3) [18,23,24], cadaveric studies (n = 2) [19,20] and one pictorial essay (Table 3).
3.2. Typer of Population
Overall, the 22 papers in the current review included 269 participants, 67 healthy volunteers and 202 patients with pathological conditions at ankle retinacula; 155 male (58.82%) and 100 female (41.18%) individuals have been evaluated, with an average of 30.88 ± 15 years. The patients had rheumatoid arthritis, psoriatic arthritis, previous ankle sprains, ankle pain, posterior tendon dislocation, had been treated surgically for chronic peroneal tendon dislocation, inversion ankle trauma and painful snapping of peroneal tendons.
3.3. Assessed Ankle Retinacula
The papers included in this review addressed superior extensor ankle retinaculum [10,12,22,24,27,29], inferior extensor ankle retinaculum [12,18,22,27,29], superior peroneal retinaculum [5,11,13,14,15,18,21,23,25,26,27,29,30], inferior peroneal retinaculum [5,16,21,26,27,28] and flexor retinaculum [5,11,17,19,20,27].
3.4. US Equipment Features and Type of Probe
Across the studies included, multiple US devices were used, each equipped with linear array transducers [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,27,28,29,30] and one with a hockey stick probe [26]. The used frequencies varied from 9 to 20 MHz [14], 6 to 15 MHz [10,11,18], 12 to 18 MHz [11], 8 to 18 MHz [18,19,26], >9 MHz [22] and 3 to 12 MHz [24]. The US machines operated in different modes: B-mode [5,11,12,13,14,15,17,18,19,20,21,22,23,24,25,26,27,28,29,30], shear-wave elastography [16], sono-palpation [12] and power-Doppler [5,11,24]. Finally, some studies dynamically evaluated ankle retinacula [14,15,17,18,22,23,24,25,26,27,28,29].
3.5. Positioning of Patient and Type of Protocol
Different protocols were used to evaluated ankle retinacula: supine position of patient with flexed knee at 30 degrees [11]; supine position with extended knee [10,12,19,24]; standing on an articulated platelet with full weight bearing with ankle in neutral position, valgus 20° and varus 30° [16]; supine position with a slight dorsiflexion of the ankle [20]; supine position with the knee joint flexed and the ankle internally rotated [21]; and supine position, static: knee flexed and ankle internally rotated and dynamic: with a pillow under the calf in rest, with active and passive ankle dorsiflexion-eversion [22]. The position of the probe was in axial [29], longitudinal [29] and oblique [26] scans.
3.6. Parameters Evaluated with Measurements and Reliability
A multiplicity of parameters was evaluated such as integrity [14,15,21,26,28], stiffness [16], echogenicity [5,10,11,18,24,25,26,27,29,30], thickness [5,10,11,12,14,24,25,26,27] and anatomical locations [19,20,23]. Only 3 of 22 papers reported data about reliability [10,11,16].
3.7. Aims of Studies
A multiplicity of aims was reported. The main aim was the diagnosis [5,10,11,12,13,14,15,16,17,18,21,22,24,25,26,27,28,29,30] of different pathological conditions. Another aim was anatomical localization [19,20,23] through carrying out cadaveric studies.
3.8. Risk of Bias Assessment and Applicability Concern
The NOS score of the included studied articles is shown in Table 1 and Table 2. After evaluation by two researchers, the studies received an average NOS score of 5.1, indicative of intermediate quality studies (Table 4 and Table 5).
4. Discussion
This comprehensive review provided a detailed analysis of the layers of ankle retinacula, type of US equipment used, patient positioning protocols, evaluated parameters and reliability analyses. A total of 22 papers were identified that investigated ankle retinacula using advanced US imaging techniques. The studies varied in their methodological designs, including eight review studies [5,13,14,21,22,24,25,26], two cross-sectional studies [10,11], six case reports or case series (n = 6) [12,14,15,17,28,31], two cohort studies [16,29], three retrospective studies [18,23,24], two cadaveric studies [19,20] and one pictorial essay [27]. This variety reflects the comprehensive scope of the review. In total, the included studies comprised 269 participants, of which 67 were healthy volunteers and 202 were patients with pathological conditions affecting the ankle retinacula. The average age of the participants was 30.88 ± 15 years old. The review’s meticulous approach in combining diverse study designs and participant demographics provided a broad and nuanced perspective on the current state of research in ankle retinacula assessment through US imaging, highlighting both the advancements and the areas requiring further investigation.
Ultrasound imaging offers an unparalleled level of detail when it comes to visualizing the retinacula of the ankle (Figure 2A–D).
This advanced imaging technique allows for the distinct identification and thorough assessment of each retinaculum, enabling clinicians to observe their normal anatomical features as well as any deviations that may indicate underlying pathologies. The retinacula of the ankle are characterized by a range of anatomical variants, which underscore the importance of numerous anatomical review studies aimed at precisely defining their anatomical localization. These studies [19,20,23] provide crucial insights that enhance our understanding of the variability, facilitating more accurate diagnosis and treatment of related conditions. The majority of data the focused on superior peroneal retinaculum [5,11,13,14,15,18,21,23,25,26,27,29,30], followed by superior extensor ankle retinaculum [5,10,12,22,24,27], superior peroneal retinaculum [5,11,13,14,15,18,21,23,25,26,27,29,30], inferior peroneal retinaculum [5,16,21,26,27,28], flexor retinaculum [5,11,17,19,20,27] and inferior extensor ankle retinaculum [5,12,18,22,27]. However, it is important to note that this level of detailed visualizations is particularly challenging for the inferior extensor retinaculum. The inferior extensor ankle retinaculum, due to its complex structure and location, presents more difficulties in US imaging compared to other retinacula. This complexity further justifies the need for extensive anatomical studies to ensure accurate identification and assessment using US imaging.
The authors of the included studies used a multiplicity of US devices and different types of transducers. Moreover, they were evaluated mainly with linear array transducers [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,27,28,29,30,31] and to a small extent with a hockey stick probe [26]. Regarding the frequency and depth of acquisition, the majority of papers examined reported frequency ranges for the US transducers, typically averaging from 6 to 18 MHz. B-mode was the most commonly used across the majority of the studies, followed by power-Doppler [5,11,24], in static and dynamic modalities [14,15,17,18,22,23,24,25,26,27,28,29], shear-wave elastography [16] and sometimes sono-palpation [12]. The comprehensive utilization of various US devices and transducers, as well as the frequency ranges employed in these studies, highlights the versatility and adaptability of US examination in the assessment of ankle retinacula. The predominant use of linear array transducers is appropriate given their high resolution and suitability for superficial structures. However, the occasional use of hockey stick probes indicated an awareness of the need for more specialized US imaging in certain scenarios. The frequency range of 6 to 18 MHz aligns well with the requirements for US imaging of the detailed structures of the ankle retinacula, providing a balance between penetration depth and resolution. The use of B-mode as the primary imaging modality is expected, given its efficacy in structural assessment, while the supplementary use of power-Doppler, shear-wave elastography and sono-palpation demonstrates a thorough approach to capturing both anatomical and functional information.
The ultrasound ankle retinacula examinations were predominantly in the supine position with an extended knee [10,12,19,24], although the supine position with the knee flexed to varying degrees was widely used [10,12]. Some authors reported standing on an articulated platform with full weight bearing and the ankle in a neutral position allowing for 20° of valgus and 30° of varus [16]. The variety of patient positionings during the US examinations, including both supine and wight-bearing positions, reflects the need to understand the retinacula under different physiological conditions. While the supine positions, both in extended and flexed knee, provide essential baseline information, the standing position on an articulated platform with full weight bearing introduced a dynamic aspect that may reveal additional insights into the functional status of the ankle retinacula under load. Overall, the methodology described in these studies reflects a robust and well-rounded approach to US imaging of ankle retinacula, although the variation in devices, techniques and patient positions underscores the need for standardization in future research to ensure the consistency and comparability of the results. Moreover, the protocols ranged from passive positioning to active tasks to assess the integrity of ankle retinacula [14,15,21,26,28]. This approach ensures a comprehensive assessment that can better inform clinical practice by capturing the retinacula’s behavior under various conditions, thereby offering more complete understanding of their functional capabilities and potential pathological changes.
The US parameters assessed included thickness [5,10,11,12,14,24,25,26,27], stiffness [16] and echogenicity [5,10,11,18,24,25,26,27,29,30]. For the superior extensor retinaculum, Pirri et al. reported an average of 0.9 ± 0.45 mm in healthy volunteers and 1.3 ± 0.5 mm for the side of previous ankle sprains in football players [10]. For superior peroneal retinaculum, Forien et al. showed a thickness of 0.6 ± 0.12 mm in rheumatoid arthritis patients and 0.71 ± 0.27 mm for psoriatic arthritis patients [11]; for flexor retinaculum, they reported a thickness of 0.64 ± 0.15 mm in rheumatoid arthritis patients and 0.96 ± 0.4 mm in psoriatic arthritis patients [11]. The detailed assessment of various US parameters such as thickness, stiffness and echogenicity, as demonstrated in the studies, underscores the capability of US imaging to provide critical insights into the structural and pathological conditions of ankle retinacula. The significant differences in retinacula thickness between healthy individuals and those with conditions like previous ankle sprains or arthritis emphasize the potential of US imaging as a diagnostic tool. However, these variations also highlight the need for a standardized measurement protocol to ensure consistency and reliability across different studies. The findings presented in this review pave the way for future research to refine and validate US parameters, ultimately enhancing their application in clinical practice.
Only three studies assessed the reliability of ankle retinacula US measurements, with intra-rater reliability consistently reported as good to excellent agreement. Pirri et al. [10] reported an excellent intra-rater reliability in the superior extensor retinaculum with an average of ICC: 0.91 (0.88–0.94). In the vertical positioning of a patient with the valgus and varus position for inferior extensor retinaculum, Rougereau et al. [16] reported a normal ICC: 0.90 (0.81–0.94); valgus 20° ICC: 0.86 (0.76–0.92); varus 30° ICC: 0.89 (0.79–0.94). The studies reviewed provide compelling evidence supporting the reliability of US measurements for ankle retinacula, particularly highlighting the strong intra-rater reliability. The results reported by Pirri et al. [10] and Rougereau et al. [16] demonstrate consistent and high ICC values across different conditions, underscoring the robustness of these measurements in clinical practice. This consistency is crucial for the diagnostic and therapeutic use of US in evaluating the ankle retinacula, suggesting that these techniques can be reliably employed across various patient positions and conditions. However, the limited number of studies underscores the need for further research to confirm these findings and expand the evidence base, particularly in diverse patient populations and settings.
Ultrasound imaging excels in identifying and characterizing a variety of pathological conditions affecting the retinacula:
- -Traumatic injuries: Acute trauma can lead to partial or complete tears of the ankle retinacula, which appear as hypoechoic disruptions within normally hyperechoic retinacular layers [5,13,14,21,22,24,25,26]. US imaging can also reveal associated tendon dislocation or subluxation. For example, Hosack et al. reported that peroneal tendon dislocation or subluxation typically results from injury to the superior peroneal retinaculum, affecting the tendons in the retromalleolar groove; this is classified using the modified Eckert and Davies system.
- -Chronic conditions: Overuse or repetitive strain can cause chronic thickening of retinacula, often accompanied by calcifications. US imaging effectively identifies these changes, aiding in the diagnosis of conditions such as stenosing tenosynovitis [5,10,12,13,14,21,22,24,25,26].
- -Inflammatory and degenerative changes: Inflammatory conditions may present as increased vascularity on Doppler imaging, while degenerative changes can lead to inhomogeneous echotexture and loss of the normal fibrillar pattern [5,11,13,14,21,22,24,25,26]. Forien et al. showed that US abnormalities of ankle flexor retinacula were more frequent and specific in psoriatic arthritis patients than in rheumatoid arthritis patients, suggesting that US examination of ankle flexor retinacula can help distinguish between the two conditions [11].
One the most significant advantages of ankle retinacula US examination over other imaging modalities is its dynamic assessment capability [3]. Real-time imaging allows clinicians to evaluate the ankle retinacula and associated tendons during movement, providing critical insights into functional abnormalities.
-Tendon instability: dynamic US imaging can demonstrate subluxation or dislocation of tendons, particularly in the context of peroneal retinacula pathology [3,5,11,13,14,15,18,21,23,25,26,27,29,30,31].-Assessment of tendon-gliding mechanism: evaluating tendon movement relative to the ankle retinacula during active and passive maneuvers helps in diagnosing and understanding the functional impact of various retinacula pathologies [13,14,21,22,24,25,26,29].
It is crucial to recognize several limitations in the referenced studies. One of the primary issues is that the majority of these studies were reviews rather than original research, which inherently limits the strength of the conclusions that can be drawn. Another significant concern is the heterogeneity of the data across these studies, which precludes their synthesis and makes it difficult to draw consistent, overarching conclusions. Given these limitations, it is evident that future research should prioritize conducting more clinical trials. These trials are essential to validate the proposed parameters and ensure their reliability and applicability in daily clinical practice. Only through such rigorous, original research can we hope to establish a solid foundation of evidence that can be effectively utilized in practical settings.
5. Conclusions
Ultrasound imaging is invaluable in assessing the ankle retinacula of ankle and foot, offering detailed visualization of both normal and pathological conditions. Understanding the normal sonographic appearance of these structures and recognizing common pathologic changes are essential for accurate diagnosis and appropriate management of ankle retinacula disorders. Dynamic US further enhances the assessment by allowing real-time evaluation of ankle retinacula function, particularly in cases of suspected instability or dislocation. In the end, future research should focus on clinical trials to validate parameters and ensure their reliability in clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pirri C. Pirri N. Stecco C. Macchi V. Porzionato A. De Caro R. Özçakar L. ‘Ultrasound Examination’ of the Musculoskeletal System: Bibliometric/Visualized Analyses on the Terminology (Change)Tomography 2023935236110.3390/tomography 901002836828380 PMC 9958559 · doi ↗ · pubmed ↗
- 2Özçakar L. Ricci V. Mezian K. Pirri C. A New and Dedicated Video Gallery: EURO-MUSCULUS/USPRM Protocols for Dynamic Ultrasound Examination of the Joints Am. J. Phys. Med. Rehabil.202210120120210.1097/PHM.000000000000195635034063 · doi ↗ · pubmed ↗
- 3Pirri C. Stecco C. Güvener O. Mezian K. Ricci V. Jacisko J. Fojtik P. Kara M. Chang K.V. Dughbaj M. EURO-MUSCULUS: European Musculoskeletal Ultrasound Study Group in Physical and Rehabilitation Medicine. EUROMUSCULUS/USPRM Dynamic Ultrasound Protocols for Ankle/Foot Am. J. Phys. Med. Rehabil.2024103 e 29e 3410.1097/PHM.000000000000234937903600 · doi ↗ · pubmed ↗
- 4Kelikian A.S. Sarrafian S.K. Sarrafian’s Anatomy of the Foot and Ankle: Descriptive, Topographical, Functional 3rd ed.Lippincott Williams & Wilkins Philadelphia, PA, USA 2011
- 5Demondion X. Canella C. Moraux A. Cohen M. Bry R. Cotton A. Retinacular disorders of the ankle and foot Semin. Musculoskelet. Radiol.20101428129110.1055/s-0030-125451820539954 · doi ↗ · pubmed ↗
- 6Numkarunarunrote N. Malik A. Aguiar R.O. Trudell D.J. Resnick D. Retinacula of the foot and ankle: MRI with anatomic correlation in cadavers Am. J. Roentgenol.2007188 W 348W 35410.2214/AJR.05.106617377003 · doi ↗ · pubmed ↗
- 7Stecco A. Stecco C. Macchi V. Porzionato A. Ferraro C. Masiero S. De Caro R. RMI study and clinical correlations of ankle retinacula damage and outcomes of ankle sprain Surg. Radiol. Anat.20113388189010.1007/s 00276-011-0784-z 21305286 · doi ↗ · pubmed ↗
- 8Stecco C. Macchi V. Porzionato A. Morra A. Parenti A. Stecco A. Delmas V. De Caro R. The ankle retinacula: Morphological evidence of the proprioceptive role of the fascial system Cells Tissues Organs.201019220021010.1159/00029022520197652 · doi ↗ · pubmed ↗