A Case of Aspergillus calidoustus Thoracic Spine Osteomyelitis
Chidi D Okoroafor, Madhu Suryadevara, Parveen Gaba, Polly Jen

TL;DR
This paper reports the first case of Aspergillus calidoustus causing spine infection in a heart transplant patient.
Contribution
The first documented case of A. calidoustus osteomyelitis in an orthotopic heart transplant recipient.
Findings
A. calidoustus caused thoracic spine osteomyelitis in a heart transplant patient.
This case highlights the potential for A. calidoustus to cause rare infections in immunocompromised individuals.
Abstract
Aspergillus infections are of significant concern in patients who are immunocompromised, including transplant recipients. Aspergillus calidoustus is an emerging pathogen reported to cause a wide array of infections. We present a case of A. calidoustus thoracic spine osteomyelitis in a patient with an orthotopic heart transplant (OHT). To our knowledge, this is the first case of A. calidoustus osteomyelitis in a patient with OHT.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1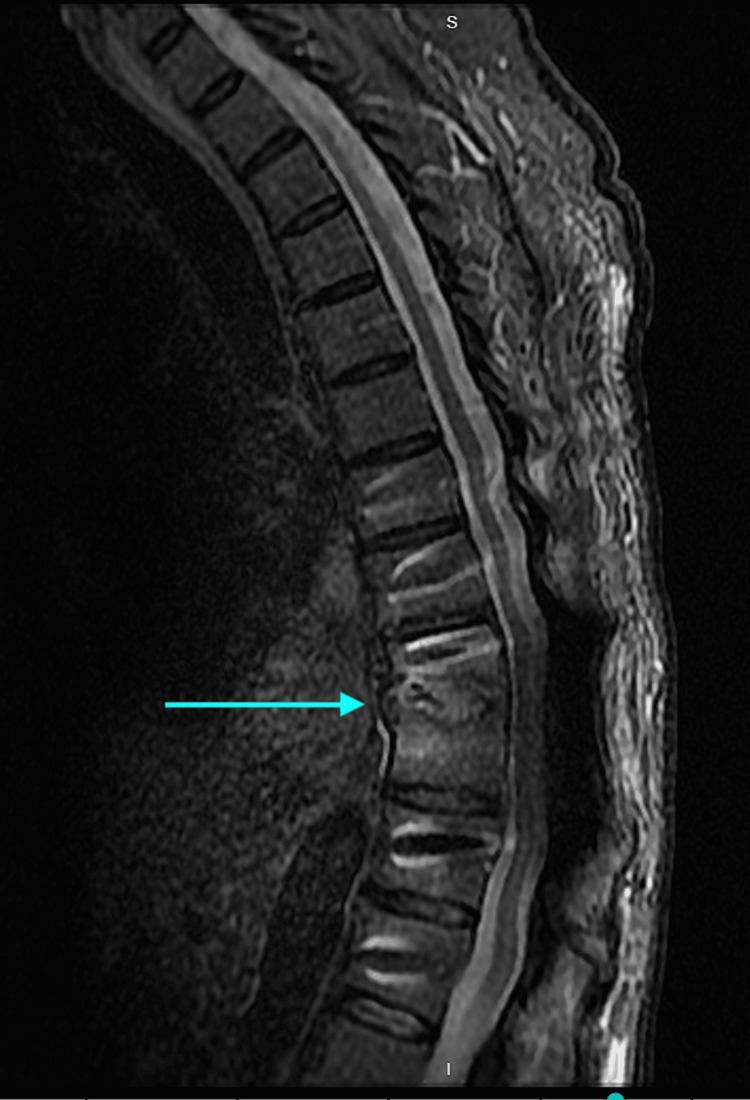 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Infectious Diseases and Tuberculosis · Fungal Infections and Studies
Introduction
Aspergillus calidoustus is a mold pathogen within the group ustus [1]. It has been gaining prominence as an emerging pathogen due to the increased use of antifungal prophylaxis in transplant patients and the resultant emergence of more resistant Aspergillus species. Solid organ transplant (SOT) and hematopoietic transplant (HCT) patients receiving immunosuppressive therapy tend to be at the greatest risk, particularly those receiving anti-mold azole prophylaxis, such as voriconazole or posaconazole [2]. Infections attributed to *A. calidoustus *may involve the lungs, central nervous system, or soft tissues, either as isolated or disseminated infections [2,3]. Calidoustus infections have been found to be increasingly resistant to antifungals, mostly triazoles, in contrast to other Aspergillus species, with the minimum inhibitory concentrations (MICs) of voriconazole of some Aspergillus species 2-16 mcg/mL and posaconazole MICs of ≥1-16 mcg/mL [2]. We present a case of *A. calidoustus *osteomyelitis affecting the thoracic spine in a patient who is one year post OHT.
Case presentation
A 64-year-old gentleman presented to the emergency room with a month-long history of sharp mid and lower back pain that had progressively worsened since the onset. He was prescribed cyclobenzaprine a few weeks prior to presentation with no significant improvement in his symptoms. He denied fever, bowel or bladder dysfunction, and upper and lower extremity weakness, but endorsed tingling of his left shoulder and left arm. The patient was afebrile on arrival with a blood pressure of 128/85 mmHg and a respiratory rate of 18 breaths per minute. Physical examination was significant for left arm paresthesia.
Significant past medical history
Orthotopic heart transplant for chronic heart failure and ischemic cardiomyopathy was performed one year ago for which he was placed on valganciclovir for CMV prophylaxis, Bactrim for antibacterial prophylaxis, and voriconazole for antifungal prophylaxis. The patient's current immunosuppression regimen consists of tacrolimus and mycophenolate mofetil.
The patient has a significant history of pulmonary aspergillosis diagnosed by pathology following a lung biopsy 13 months ago for which the patient was initially treated with voriconazole and micafungin and then switched to isavuconazole with voriconazole discontinued due to side effects.
Magnetic resonance imaging (MRI) of the spine with and without contrast done on admission was significant for ventral epidural abscess of T9-T10 with discitis and osteomyelitis, moderate spinal canal stenosis, and ventral cord impingement. Due to these findings, infectious disease and neurosurgery services were consulted. The patient was taken to the operating room by the neurosurgery service where a T9-T10 laminectomy was done with attempted abscess evacuation; however, no evidence of frank pus was noted during surgery. No growth was noted on intraoperative bacterial cultures. Fungal and acid-fast bacilli cultures were not collected. The surgical pathology of the T9-T10 specimen sent was consistent with fibrous tissue and blood clots.
The patient was empirically started on cefepime and daptomycin for suspected bacterial vertebral osteomyelitis. On the 23rd day of admission, repeat MRI imaging of the thoracic spine showed persistence of T9-T10 changes with discitis and osteomyelitis. Computed tomography (CT)-guided biopsy of the T9-T10 thoracic spine was done by interventional radiology on the 27th day of hospitalization with the pathology report consistent with prior findings. On the 40th day of hospitalization, the patient underwent thoracic spine decompression with arthrodesis done by neurosurgery with bone cultures sent for microbiology. Bone culture preliminary report was significant for rare fungus. Liposomal amphotericin B was initiated on day 42 based on the preliminary results. The bone culture specimen was sent to a reference laboratory at the University of Texas at San Antonio for further identification and susceptibility testing. The final bone culture report was positive for A. calidoustus with susceptibility results indicating amphotericin B MIC = 0.5 mcg/mL, micafungin MIC ≤ 0.015 mcg/mL, rezafungin MIC ≤ 0.015 mcg/mL, voriconazole MIC 4 mcg/mL, isavuconazole MIC 1 mcg/mL, and posaconazole MIC 4 mcg/mL. The decision was made to treat Aspergillus vertebral osteomyelitis with prolonged combination therapy, so micafungin was added to liposomal amphotericin B following the final culture report. The patient was discharged on day 82 of hospitalization and was clinically stable with upper and lower extremity motor and sensory function still preserved.
MRI findings pre- and post-initiation of antifungal treatment with liposomal amphotericin B and micafungin are shown in Figure 1 and Figure 2, with significant improvement in the imaging of vertebral lesions eight weeks into treatment compared to when it was initiated.
MRI of the thoracic spine with the T9-T10 area being involved.
MRI of the thoracic spine with the T9-T10 area now with significant improvement in the lesion.
Discussion
*A. calidoustus *is a recently defined species of Aspergillus reported as a growing cause of infections in immunosuppressed individuals. While over 300 Aspergillus species are known to exist, including many others in the same section of Usti, A. calidoustus is distinct as a thermotolerant mold that is able to grow at 37 °C, similar to the human body temperature [1]. In addition, the appearance of A. calidoustus differs from the closely related A. ustus, where the mycelium color on Czapek yeast extract agar for A. calidoustus is grayish yellow to grayish brown compared to the cream or light-yellow appearance of *A. ustus *[2,3].
*A. calidoustus *is commonly isolated from food, soil, and air; however, infections due to this species have been increasingly reported. The relative prevalence of A. calidoustus causing infections among Aspergillus species has been reported to be 1.4% in Spain and 2.8% in the United States [2,4-6]. Similar to other Aspergillus infections, solid organ and hematopoietic transplant patients are at increased risk for infection due to the need for immunosuppressive medications to prevent graft rejection [2]. However, the treatment of *A. calidoustus *infections is notoriously difficult due to the high MICs for most antifungals, with decreased susceptibility to azoles attributed to the prevalence of prophylaxis use in transplant patients [1-2]. The reported susceptibility patterns for A. calidoustus have been variable with a wide range of MICs reported: voriconazole 2-16 μg/mL, posaconazole ≥1-16 μg/mL, caspofungin 0.03-32 μg/mL [2], and amphotericin B 0.25-32 μg/mL [2,4-10]. The in vitro susceptibility results from our case are consistent with those previously published as seen in this case series [2]. While susceptibility breakpoints have not been established by professional organizations for A. calidoustus species, the triazole MICs reflect the need for concentrations that exceed those that can be reasonably achieved using standard doses of triazole antifungals based on their pharmacokinetic and pharmacodynamics properties. The use of non-azole antifungals, as a monotherapy or combination therapy, has been reported with success in isolated cases or case series [2,10,11].
There is very limited published experience on A. calidoustus infections in transplant patients. One case series [2] described a 67-year-old female with a history of lung transplantation who developed thoracic back pain and was found to have enhancement of the T12-L1 disc space and leptomeningeal enhancement of the anterior surface of the spinal cord at the T12 level. Image-guided intervertebral disc aspiration was performed, and a fungal culture grew one colony of A. calidoustus [2]. One of the other cases in the cases series describes A. calidoustus-related pulmonary aspergillosis, brain abscesses, and maxillary and ethmoidal sinus infection (in the same patient) secondary to A. calidoustus, all in HCT patients on immunosuppression. To the authors’ knowledge, there are no cases in the literature describing heart transplant patients with infections secondary A. calidoustus infections as described in this case.
In transplant recipients, infections caused by A. calidoustus have been found to have mostly occurred within the first few months or years following receipt of SOT or HCT, although some episodes occurred many years after transplantation [2]. As discussed in this case series from the TRANSNET database, the median onset of infection caused by all Aspergillus species among HCT recipients was noted to be 99 days [2]. It has been discussed in the literature that in SOT recipients in the United States, the median time to invasive aspergillosis (IA) caused by any species was 184 days post SOT [2], with a wide interquartile range of approximately one month to 27 months post SOT [2]. Approximately 20% of IA cases occurred more than three years after transplantation. The patient in our case appears to have developed a disseminated infection with the index organ being the lungs as he was diagnosed and treated for pulmonary aspergillosis over a year ago. At that time, the diagnosis was based upon the pathology of the lung tissue from biopsy as no isolate was sent for culture. A. calidoustus infections in SOT patients have been treated with a combination of antifungal therapy and surgery as in our case [1-2,10]. Confirmatory data are lacking with respect to clinical efficacy and achievement of cure using this approach. Furthermore, the incidence of toxicities associated with antifungal therapy, as a single or combination therapy, was not well-described. The potential risks and benefits of combination antifungal therapy versus surgery must be considered by clinicians when making treatment decisions in patients with these infections.
Conclusions
This is a unique case of thoracic spine osteomyelitis caused by A. calidoustus in a heart transplant recipient, from possible dissemination after an index pulmonary infection. As an emerging pathogen, it is important to understand the epidemiology and pathogenesis of this organism in humans. This report represents the first described case of vertebral osteomyelitis in a heart transplant patient due to A. calidoustus.
This case also highlights the predisposition of transplant patients on immunosuppression developing resistant fungal infections as in this case, due to the prior use of prophylactic antifungal agents post transplant.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical relevance and characteristics of Aspergillus calidoustus and other Aspergillus species of section usti J Fungi (Basel) Glampedakis E Erard V Lamoth F 6202010.3390/jof 6020084 PMC 734493332545485 · doi ↗ · pubmed ↗
- 2Aspergillus calidoustus case series and review of the literature Transpl Infect Dis Seroy J Antiporta P Grim SA Proia LA Singh K Clark NM 19201710.1111/tid.1275528741738 · doi ↗ · pubmed ↗
- 3Aspergillus calidoustus sp. nov., causative agent of human infections previously assigned to Aspergillus ustus Eukaryot Cell Varga J Houbraken J Van Der Lee HA Verweij PE Samson RA 630638720081828159610.1128/EC.00425-07PMC 2292628 · doi ↗ · pubmed ↗
- 4Emergence of Aspergillus calidoustus infection in the era of posttransplantation azole prophylaxis Transplantation Egli A Fuller J Humar A 4034109420122280544110.1097/TP.0b 013e 31825992 f 0 · doi ↗ · pubmed ↗
- 5Population-based survey of filamentous fungi and antifungal resistance in Spain (FILPOP Study)Antimicrob Agents Chemother Alastruey-Izquierdo A Mellado E Peláez T 338033875720132366937710.1128/AAC.00383-13PMC 3697314 · doi ↗ · pubmed ↗
- 6Molecular identification of Aspergillus species collected for the Transplant-Associated Infection Surveillance Network J Clin Microbiol Balajee SA Kano R Baddley JW 313831414720091967521510.1128/JCM.01070-09PMC 2756904 · doi ↗ · pubmed ↗
- 7In vitro activity of nine antifungal agents against clinical isolates of Aspergillus calidoustus Med Mycol Alastruey-Izquierdo A Cuesta I Houbraken J Cuenca-Estrella M Monzón A Rodriguez-Tudela JL 971024820101929636610.3109/13693780902803040 · doi ↗ · pubmed ↗
- 8Antifungal susceptibility profile of cryptic species of Aspergillus Mycopathologia Alastruey-Izquierdo A Alcazar-Fuoli L Cuenca-Estrella M 42743317820142497267010.1007/s 11046-014-9775-z · doi ↗ · pubmed ↗