Evaluating Immunologic and Illness Outcomes of SARS-CoV-2 Infection in Vaccinated and Unvaccinated Children Aged ≥ 5 Years, in a Multisite Longitudinal Cohort
Cynthia Porter, Zoe L. Lyski, Jennifer L. Uhrlaub, Katherine D. Ellingson, Zuha Jeddy, Lisa Gwynn, Patrick Rivers, Ryan Sprissler, Kurt T. Hegmann, Melissa M. Coughlin, Ashley L. Fowlkes, James Hollister, Lindsay LeClair, Josephine Mak, Shawn C. Beitel, Sammantha Fuller

TL;DR
Vaccinated children who later get infected with SARS-CoV-2 have stronger antibody responses and are less likely to have fevers than unvaccinated children.
Contribution
This study provides new evidence on the immune and clinical outcomes of SARS-CoV-2 infection in vaccinated versus unvaccinated children.
Findings
Vaccinated children had significantly higher antibody levels against SARS-CoV-2 Spike proteins compared to unvaccinated children.
Vaccinated children were less likely to report fever during SARS-CoV-2 infection compared to unvaccinated children.
Abstract
Children with prior vaccine-induced immunity at the time of infection had more robust antibody binding against the receptor-binding domain (RBD) and S2 domain of Spike, and experienced fever less often compared to unvaccinated children during primary SARS-CoV-2 infection. Hybrid immunity, as a result of infection and vaccination to SARS-CoV-2, has been well studied in adults but limited evidence is available in children. We evaluated the antibody responses to primary SARS-CoV-2 infection among vaccinated and unvaccinated children aged ≥ 5 years. Methods: A longitudinal cohort study of children aged ≥ 5 was conducted during August 2021–August 2022, at sites in Arizona, Texas, Utah, and Florida. Children submitted weekly nasal swabs for PCR testing and provided sera 14–59 days after PCR-confirmed SARS-CoV-2 infection. Antibodies were measured by ELISA against the receptor-binding domain…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
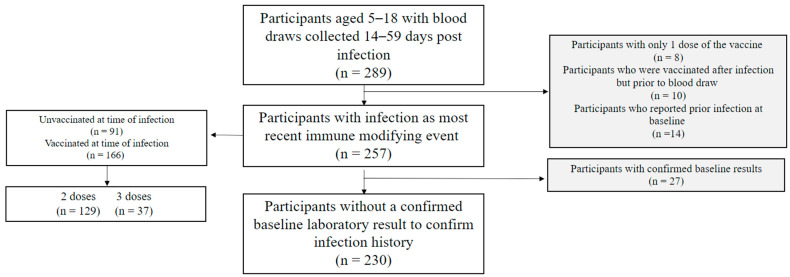 Figure 1
Figure 1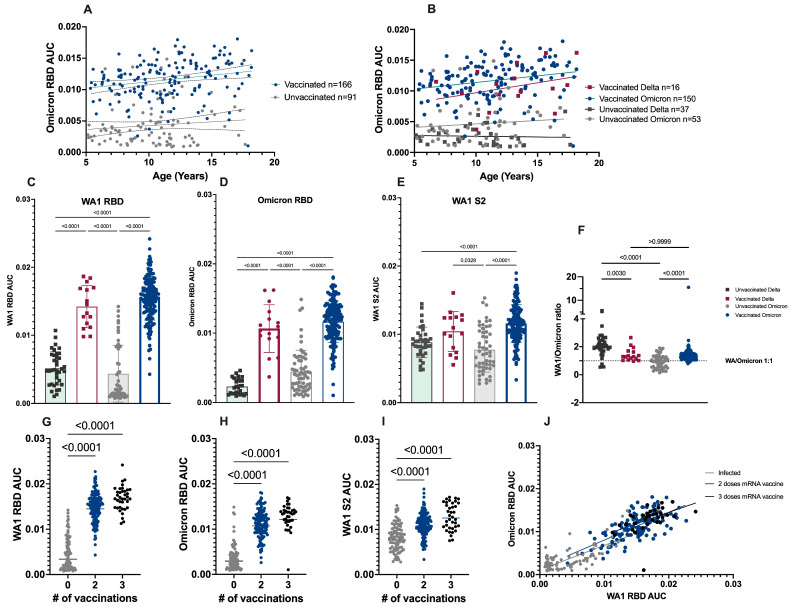 Figure 2
Figure 2- —Centers for Disease Control
- —University of Arizona
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · COVID-19 Clinical Research Studies · Respiratory viral infections research
1. Background
The humoral immune response to infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of coronavirus disease 2019 (COVID-19), has been extensively studied in adults [1,2,3,4]; however, information regarding the antibody response in children is more limited, but of high public health importance. Children are less likely to experience severe disease compared to adults and may have different humoral immune responses to infection [5,6,7].
Differences in neutralizing antibodies against SARS-CoV-2 infection have been observed in different age groups, with children younger than three years exhibiting the highest antibody titers [8,9,10] and children younger than 12 years exhibiting higher titers of binding and neutralizing SARS-CoV-2-specific antibodies compared to adolescents and adults following infection with an origin strain of SARS-CoV-2 (WA1) [1,8,11]. Following infection or vaccination with two doses of monovalent ancestral mRNA COVID-19 vaccine, elevated binding and neutralizing antibodies are present in adults and children; in both cases, SARS-CoV-2-specific antibodies remain detectable six months to one year post-infection or vaccination [9,12,13,14,15].
At the beginning of 2022, an increased incidence of SARS-CoV-2 infections was observed, largely due to the highly transmissible Omicron variant. During this time, children aged 5 years and older were eligible for COVID-19 vaccination in the United States [16]. This rise in infections resulted in a noticeable increase in hybrid immunity. In adults, hybrid immunity has been shown to result in superior antibody responses compared to infection or vaccination alone [17,18]. Specifically, adults with hybrid immunity exhibit higher antibody titers, increased antibody durability (greater than 7 months), greater neutralization against variants of concern, and a reduced risk of infection when compared to adults who are only infected or vaccinated [17,18]. However, studies are limited in children and adolescents [19,20,21].
The PROTECT (Pediatric Research Observing Trends and Exposures in COVID-19 Timelines) study provides an opportunity to assess antibody responses to primary SARS-CoV-2 infections [22]. Previous investigations using the PROTECT cohort demonstrated that children aged 5–11 years exhibit a robust antibody response following the primary monovalent ancestral mRNA COVID-19 vaccine series, and those with the highest magnitude antibody responses were less likely to experience post-vaccine infections [23]. The aim of the present investigation is to evaluate SARS-CoV-2-specific antibody responses following in-study, SARS-CoV-2 infection, confirmed by real-time reverse transcription polymerase chain reaction (rRT-PCR). Children in this analysis were either unvaccinated or had received two or three doses of ancestral monovalent mRNA COVID-19 vaccination 14 or more days prior to infection. This study aims to add to the body of knowledge regarding the antibody response and illness symptoms after initial SARS-CoV-2 infection among pediatric groups who were unvaccinated or vaccinated at the time of infection.
2. Methods
2.1. Study Design
The PROTECT study, enrolling children aged 6 months to 17 years, was initiated in July 2021 in four states: Arizona, Florida, Texas, and Utah; the protocols have been previously described [22]. PROTECT is an ancillary study by the Arizona Healthcare, Emergency Response, and Other Essential Workers Study and Research on the Epidemiology of SARS-CoV-2 in Essential Response Personnel (HEROES-RECOVER) network, which is composed of two large prospective cohorts of adult participants [24,25].
Children of HEROES-RECOVER participants and from other community members were recruited for the study. Parents/legal guardians provided informed consent and children aged 12 to 17 years provided assent for study participation. The study protocol was approved by the Abt Associates Institutional Review Board (IRB) (which serves as the single IRB of record for the Florida, Texas, and Utah sites and Centers for Disease Control and Prevention [CDC]) and by the University of Arizona IRB (for the Arizona site).
2.2. Inclusion and Exclusion Criteria
Children were included in the analysis if (1) they experienced a primary SARS-CoV-2 infection during the study period, namely August 2021–August 2022, determined by the earliest available post-infection blood draws, (2) they were five years of age or older (due to the timing of vaccine eligibility), (3) they had no self-reported history of SARS-CoV-2 infection, (4) they were either unvaccinated or fully vaccinated (received two or three doses of ancestral monovalent Pfizer-BioNTech COVID-19 mRNA vaccine, Moderna COVID-19 mRNA-1273 or a combination of the two vaccines 14 days or more prior to infection, and (5) they provided an in-study SARS-CoV-2 post-infection blood draw during the study period, and (6) within 14–59 days of infection. Baseline antibody test results were not used in the primary analysis because blood draws were optional and not completed by all participants. Children were excluded if they had only one dose of monovalent COVID-19 mRNA vaccine or obtained an additional vaccine dose after infection but prior to specimen collection or had reported a prior infection at the time of enrollment.
2.3. Data Collection
Upon enrollment, children or their parents/legal guardians provided sociodemographic information, school/daycare attendance, percent of time wearing masks outside the home, COVID-19 infection history, health insurance coverage, and medical history (e.g., influenza and other childhood vaccines, medical conditions, and daily medication use). The COVID-19 vaccination status was self- or parent-reported through electronic surveys and was verified primarily by vaccination cards, electronic medical records, or state Immunization Information Systems. Children provided a self-collected or caregiver-collected/assisted weekly mid-turbinate nasal specimen for SARS-CoV-2 testing at the Marshfield Clinical Research Laboratories (Marshfield, WI) and provided self-reported information regarding COVID-19 symptoms each week. Participants were asked to provide an additional specimen at symptom onset [22]. The predominant circulating SARS-CoV-2 variant was determined when the national prevalence exceeded 50% of the current circulating viral variants [26]. The study period coincided with the Delta (August 2021–December 2021) and Omicron (December 2021–August 2022) periods, with most infections occurring from Omicron [27].
2.4. Blood Collection
Blood collection was not required for inclusion in the PROTECT study. For this investigation, participating children could provide a blood specimen at enrollment and again 14–59 days following the in-study primary SARS-CoV-2 infection. Serum samples were obtained from 5–10 mL of whole blood, then frozen and transported on dry ice to the University of Arizona, where they were stored at −80 °C until tested [28].
2.5. Enzyme-Linked Immunosorbent Assay (EL–ISA)
Sera were sent to the University of Arizona Genetics Core laboratory for serologic testing. ELISAs were used to measure the binding antibodies specific to SARS-CoV-2 WA1 and Omicron RBD, as well as WA1 S2, as previously described [29]. Briefly, five 3-fold dilutions of sera were made starting at a 1:60 dilution and reported as the endpoint titer. The optical density was measured, and the antibody levels were reported as areas under the curve (AUC) [29,30,31]. Qualitative ELISAs against RBD and S2 were conducted on serum collected at enrollment (if provided) in unvaccinated children to verify no prior SARS-CoV-2 infection. These were not used to determine the prior infection status in this analysis for children who were already vaccinated at the time of enrollment [32].
2.6. Statistical Methods
The antibody response to infection was assessed by calculating the antibody AUC for RBD and S2 antibodies. Descriptive statistics of the participant demographics were generated and used to examine differences in the humoral immune response by vaccination status at infection. Differences between groups were separately assessed using a Kruskal–Wallis test, where p values < 0.05 were considered statistically significant. Variables were assessed for collinearity.
To further examine the relationship between the post-infection antibody response and previous vaccination status, multiple linear regression was used to examine the AUC values, adjusting for the age category, body mass index (BMI) percentile for age, gender, and symptom status (dichotomized as asymptomatic or any symptoms) [6,7,8]. Because the AUC values were not normally distributed, they were log transformed. Separate models were generated for the WA1 and BA.2 RBD antibody results. The proportional odds assumption and the goodness of fit were examined through the Hosmer and Lemeshow test. The results of the ordinal models and descriptive tables with time to vaccination are listed in the Supplemental Materials (Tables S1 and S2). All analyses were conducted in SAS v9.4 (SAS Inc., Cary, NC, USA) and Graphpad Prism (version 9.4.1 for Mac, GraphPad Software, San Diego, CA, USA).
2.7. Sensitivity Analysis
To test the robustness of the models, we used Firth’s method for the bias correction of the proportional odds regression estimator, previously used by Lipitz et al. [33]. A second sensitivity analysis was conducted by assessing participants that potentially had missed SARS-CoV-2 infections at enrollment due to limitations in the laboratory methods mentioned previously, removing participants who were unvaccinated at the time of enrollment who had a positive qualitative ELISA result measured by RBD or S2. This was to assess only those who had self-reported results and were unable to confirm their previous infection status through a blood draw.
3. Results
From August 2021 to August 2022, 289 children provided a blood specimen 14–59 days post-infection (Figure 1). Children who had obtained only one dose of the vaccine (n = 8), were vaccinated after infection but prior to blood draw (n = 10), or had reported a previous infection at baseline (n = 14) were excluded, bringing the total sample size to 257.
Of the 257 children, 166 (65%) were vaccinated at the time of infection (Table 1). Of those, 129 (78%) received two doses and 37 (22%) received three doses of ancestral monovalent mRNA COVID-19 vaccine, either Pfizer-BioNTech or a combination of the Moderna mRNA-1273 and Pfizer-BioNTech vaccines. In addition, 204 (79%) had infections that coincided with Omicron variant predominance, while 53 (21%) experienced an infection during Delta predominance.
Of the analytic sample, 123 (48%) were female, 165 (64%) were non-Hispanic white, and 64 (25%) were Hispanic; 31 (12%) were overweight or obese; 221 (86%) did not have chronic conditions; and 204 (79%) were from study sites in Arizona, 13 (5%) were from Temple, TX, 11 (4%) were from Miami, FL, and 29 (11%) were from Salt Lake City, UT.
In addition, 212 (82%) reported symptomatic infection and had PCR-positive results lasting an average of 1.5 weeks (standard deviation [SD] 1.3). Children spent a mean of 1.7 (SD 1.8) days in bed during their illnesses, and 99 (38%) reported fever and experienced symptoms lasting an average of 8.6 (SD 7.9) days. Symptoms during illness did not vary significantly for vaccinated or unvaccinated children. Significant differences in illness characteristics were observed in the duration of PCR positivity, with a shorter average number of weeks (1.2, SD 1.0, vs. 1.6 SD 1.4, p = 0.028) and a higher incidence of fever (48%, vs. 33%, p = 0.021) in unvaccinated participants compared to vaccinated participants. Significant differences were also observed between the site and vaccination status (p = 0.020) (Table 1).
3.1. Association of Immune Response and Vaccination Status
Our unadjusted linear regression models examined the relationship between vaccination status and the WA1 RBD antibody response and found that the post-infection antibody AUC values were 340% higher in vaccinated children compared to unvaccinated children (geometric mean ratio [GMR]: 4.4 (95% CI: 3.8, 5.1) p ≤ 0.0001) (Supplemental Table S1). After adjusting for weight, age, symptomatic infection, and gender, there remained 330% higher WA1 RBD antibody AUC values among vaccinated children compared to unvaccinated children (GMR: 4.3 (95% CI: 3.8, 5.0) p ≤ 0.0001). After adjustment in the BA.2 models, there were 260% higher BA.2 RBD antibody AUC values among vaccinated compared to unvaccinated children (GMR: 3.6 (95% CI: 3.2, 4.1) p ≤ 0.0001). There was no change in the GMR between the unadjusted and adjusted BA.2 models. These findings agree with the adjusted and unadjusted ordinal logistic regression models examining WA1 and BA.2 RBD antibodies using end titers (Supplemental Table S2).
After removing unvaccinated children with positive baseline qualitative ELISA results (n = 27) in the adjusted models, 340% higher WA1 RBD antibody AUC values were observed post-infection among vaccinated compared with unvaccinated participants (GMR: 4.4, 95% CI: (3.8, 5.1) p ≤ 0.0001) and 260% higher BA.2 RBD antibody AUC values were observed compared with unvaccinated participants (GMR: 3.6, 95% CI: (3.2, 4.2) p ≤ 0.0001) (Supplemental Table S1). These findings agree with the unadjusted and adjusted analysis.
Statistically significant differences were not observed between age groups and the antibody AUC (p = 0.05); however, statistically significant differences in the mean antibody AUC values for both WA1 and BA.2 RBD antibodies (p < 0.0001) were observed when stratified by vaccination status, with higher values among the previously vaccinated group (Figure 2A), regardless of whether infection was with Delta or Omicron (Figure 2B), or what antigen was tested (Figure 2C–E). The WA1 RBD mean antibody AUC values (Figure 2C) were four times higher among vaccinated compared to unvaccinated children (0.003 vs. 0.01, p < 0.0001). A similar trend was observed for BA.2 RBD antibodies (Figure 2D), where the mean AUC in vaccinated children was 3.3 times that observed in unvaccinated children. The smallest differences in the antibody response between vaccinated and unvaccinated children were observed for WA1 S2-binding antibodies, where the mean S2 antibodies were 1.4 times higher in vaccinated compared to unvaccinated children (Figure 2E).
3.2. Ratio of WA1 to Omicron Binding Antibodies
The ratio of WA1 to BA.2 RBD-binding antibodies was further explored (Figure 2F) by plotting the ratio of the WA1 RBD antibody AUC values over the BA.2 RBD antibody AUC values (for each child individually). Among unvaccinated children, there was a significant difference in the mean WA1/BA.2 ratios (p < 0.0001) by variant, with a GMR of 2.0 for Delta-infected participants and 0.8 for BA.2-infected participants. In vaccinated children, there was no significant difference in the mean WA1/BA.2 ratios (GMR for both: 1.4).
3.3. Antibody Response to Primary Infection by Number of COVID-19 Vaccine Doses
The post-infection RBD antibody AUC values were stratified by the number of ancestral monovalent mRNA COVID-19 vaccines received (Figure 2G–J). The RBD antibody AUC values increased with additional vaccine doses for all antigens tested. A significant difference was observed between zero and either two or three doses of ancestral monovalent mRNA COVID-19 vaccine (p < 0.0001), as noted above. However, there was no significant difference between two or three doses of vaccine (p < 0.0001). The relationship between the BA.2 and WA1 RBD antibody AUC values was explored (Figure 2J) to determine whether skewing towards antibody-binding WA1 or BA.2 was occurring based on the number of vaccine doses. The slopes of the regression lines were not significantly different (p = 0.78), indicating that the relationship between BA.2 and WA1-binding antibodies does not change with additional ancestral vaccine doses; however, there was a trend towards higher AUC values (both WA1 RBD and BA.2 RBD) with a greater number of vaccine doses.
4. Discussion
Here, we examined the antibody responses among children aged ≥5 years with and without prior ancestral monovalent mRNA COVID-19 vaccination at the time of infection. A relationship between the antibody response and age was not observed; however, vaccinated children who received at least two doses of ancestral monovalent mRNA COVID-19 vaccine prior to infection exhibited antibody responses of higher magnitude compared to those who were unvaccinated at the time of infection, for both RBD (WA1 and BA.2) and S2-binding antibodies (WA1) irrespective of the infecting virus (Delta or Omicron). These increased antibody titers (up to four times higher in vaccinated compared to unvaccinated against WA1 RBD) can translate to lower odds of experiencing subsequent SARS-CoV-2 infections, as previously shown by our group [23]. In this study, no significant differences in the mean antibody AUC values were observed between two or three doses of monovalent mRNA vaccination; for RBD (WA1 and BA.2) and S2 (WA1), however, differences in antibody affinity, the neutralization breadth, and durability are expected to differ greatly with additional antigen exposures [17,21,34].
Previous research has found that vaccination in children protects against multisystem inflammatory syndrome and death; consistent with that, no cases of severe illness were reported in this study [2,35,36]. Here, it was observed that children vaccinated prior to infection experienced a longer mean duration of PCR positivity, as measured by weekly PCR testing, but were symptomatic for fewer days, with a smaller proportion experiencing fever compared to unvaccinated children. This is an important finding and further supports the importance of vaccination in limiting disease symptoms.
This study has multiple limitations. First, it is possible that previously infected participants did not report infection prior to enrollment. Blood draws at enrollment were not mandatory, resulting in limited baseline serological data. However, our sensitivity analysis suggests that this did not greatly influence the study findings. Secondly, using PCR positivity to determine illness duration may not provide information about differences in the duration of infectivity among vaccinated or unvaccinated groups, because PCR can detect nucleic acids from viruses that are no longer infectious [37,38,39,40,41]. Third, children less than 5 years of age were not eligible for vaccination during this period and not included in this analysis. Fourth, these results are not generalizable to updated vaccine formulations (e.g., bivalent or XBB.1.5 monovalent mRNA vaccine). Fifth, none of the children in this study received a primary series of Moderna mRNA-1273. Sixth, the convalescent blood draws were performed 14–59 days post-infection for all children; however, the time between immune-modifying events (i.e., vaccination and infection) was not included in the analysis. Children in this cohort experienced mild symptoms during infection and did not have many comorbid conditions. Despite significant differences between the site and vaccination status, the study site was not able to be included in the model due to a lack of model convergence and small enrollment numbers at some sites. However, statistically significant differences were not observed between the antibody response and site.
The strengths of this study are that it includes a large prospective cohort of school-age children and adolescents, allowing for symptomatic and asymptomatic SARS-CoV-2 infections to be captured in real-time due to weekly PCR testing. Second, blood draws were collected 14–59 days post-infection, allowing for controlled comparisons between groups. Third, the antibody responses to both WA1 and Omicron were examined to compare the immune response across different variants.
5. Conclusions
In conclusion, children who were vaccinated at the time of infection had higher antibody levels during convalescence compared to unvaccinated children, and lower proportions reported fever during SARS-CoV-2 infection. More research is needed to understand the impact of varying numbers of antigen exposures, timing of exposure, order of immune-modifying events, and comorbid conditions, as well as differences by vaccination status with the bivalent and monovalent XBB.1.5 boosters.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bonfante F. Costenaro P. Cantarutti A. Di Chiara C. Bortolami A. Petrara M.R. Carmona F. Pagliari M. Cosma C. Cozzani S. Mild SARS-Co V-2 Infections and Neutralizing Antibody Titers Pediatrics 2021148 e 202105217310.1542/peds.2021-05217334158312 · doi ↗ · pubmed ↗
- 2Fowlkes A.L. Yoon S.K. Lutrick K. Gwynn L. Burns J. Grant L. Phillips A.L. Ellingson K. Ferraris M.V. Le Clair L.B. Effectiveness of 2-Dose BNT 162b 2 (Pfizer Bio N Tech) m RNA Vaccine in Preventing SARS-Co V-2 Infection among Children Aged 5–11 Years and Adolescents Aged 12–15 Years-PROTECT Cohort, July 2021-February 2022 MMWR Morb. Mortal. Wkly. Rep.20227142242810.15585/mmwr.mm 7111 e 135298453 PMC 8942308 · doi ↗ · pubmed ↗
- 3Levin E.G. Lustig Y. Cohen C. Fluss R. Indenbaum V. Amit S. Doolman R. Asraf K. Mendelson E. Ziv A. Waning Immune Humoral Response to BNT 162b 2 Covid-19 Vaccine over 6 Months N. Engl. J. Med.2021385 e 8410.1056/NEJ Moa 211458334614326 PMC 8522797 · doi ↗ · pubmed ↗
- 4Matusali G. Sberna G. Meschi S. Gramigna G. Colavita F. Lapa D. Francalancia M. Bettini A. Capobianchi M.R. Puro V. Differential Dynamics of SARS-Co V-2 Binding and Functional Antibodies upon BNT 162b 2 Vaccine: A 6-Month Follow-Up Viruses 20221431210.3390/v 1402031235215903 PMC 8878369 · doi ↗ · pubmed ↗
- 5Chou J. Thomas P.G. Randolph A.G. Immunology of SARS-Co V-2 infection in children Nat. Immunol.20222317718510.1038/s 41590-021-01123-935105983 PMC 8981222 · doi ↗ · pubmed ↗
- 6Rotulo G.A. Palma P. Understanding COVID-19 in children: Immune determinants and post-infection conditions Pediatr. Res.20239443444210.1038/s 41390-023-02549-736879079 PMC 9987407 · doi ↗ · pubmed ↗
- 7Brodin P. SARS-Co V-2 infections in children: Understanding diverse outcomes Immunity 20225520120910.1016/j.immuni.2022.01.01435093190 PMC 8769938 · doi ↗ · pubmed ↗
- 8Yang H.S. Costa V. Racine-Brzostek S.E. Acker K.P. Yee J. Chen Z. Karbaschi M. Zuk R. Rand S. Sukhu A. Association of Age with SARS-Co V-2 Antibody Response JAMA Netw. Open 20214 e 21430210.1001/jamanetworkopen.2021.430233749770 PMC 7985726 · doi ↗ · pubmed ↗