Effects of L-Ornithine-L-Aspartate on Angiogenesis and Perfusion in Subacute Hind Limb Ischemia: Preliminary Study
Sanghoon Jung, Ye Jin Park, Jiwon Jeon, Kyuseok Kim

TL;DR
This study shows that L-Ornithine-L-Aspartate improves blood flow and new blood vessel growth in rats with leg artery blockage.
Contribution
The study is the first to document LOLA's effect on angiogenesis and perfusion recovery in subacute hind limb ischemia.
Findings
LOLA treatment significantly increased perfusion in ischemic limbs.
LOLA led to higher CD31-positive capillary density and VEGF overexpression.
Perfusion improvements were observed during the subacute phase of HLI.
Abstract
The current treatment options for peripheral arterial disease (PAD) are limited due to a lack of significant high-level evidence to inform clinical decisions and unfavorable outcomes in terms of cost-effectiveness and amputation rates. In order to suggest the use of the commercially available L-Ornithine-L-Aspartate (LOLA) for treating PAD, we induced hind limb ischemia (HLI) by unilaterally ligating the femoral artery in a rat model. The rats were randomly divided into three groups, with seven rats assigned to each group: group 1 (control), group 2 (sorbitol), and group 3 (LOLA). Intraperitoneal injections were administered five times on post-operative days (PODs) 3, 5, 7, 10, and 12. Perfusion imaging was conducted on PODs 7 and 14 and compared to pre-operative perfusion imaging. Immunohistochemistry staining and Western blotting were performed after the final perfusion imaging. Group…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
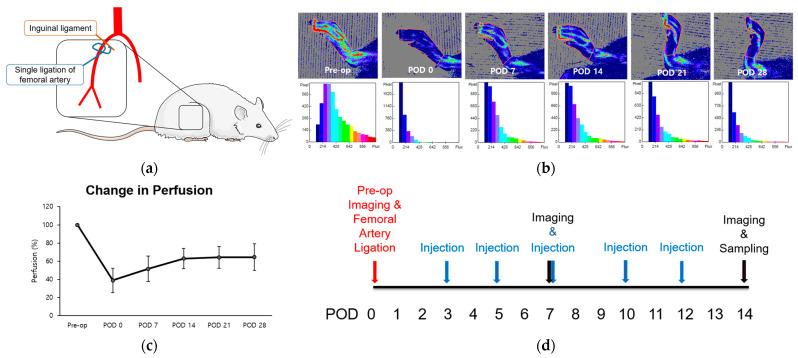 Figure 1
Figure 1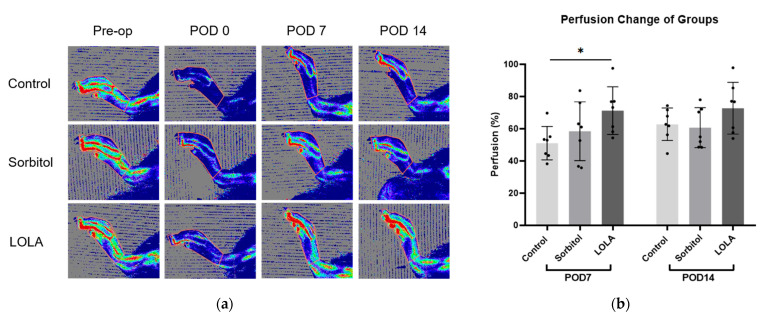 Figure 2
Figure 2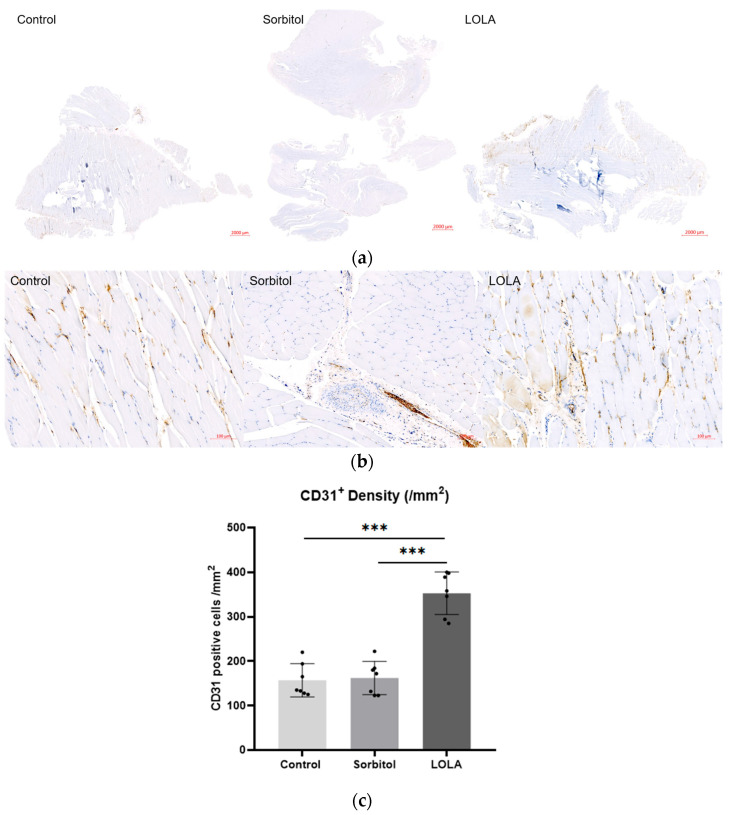 Figure 3
Figure 3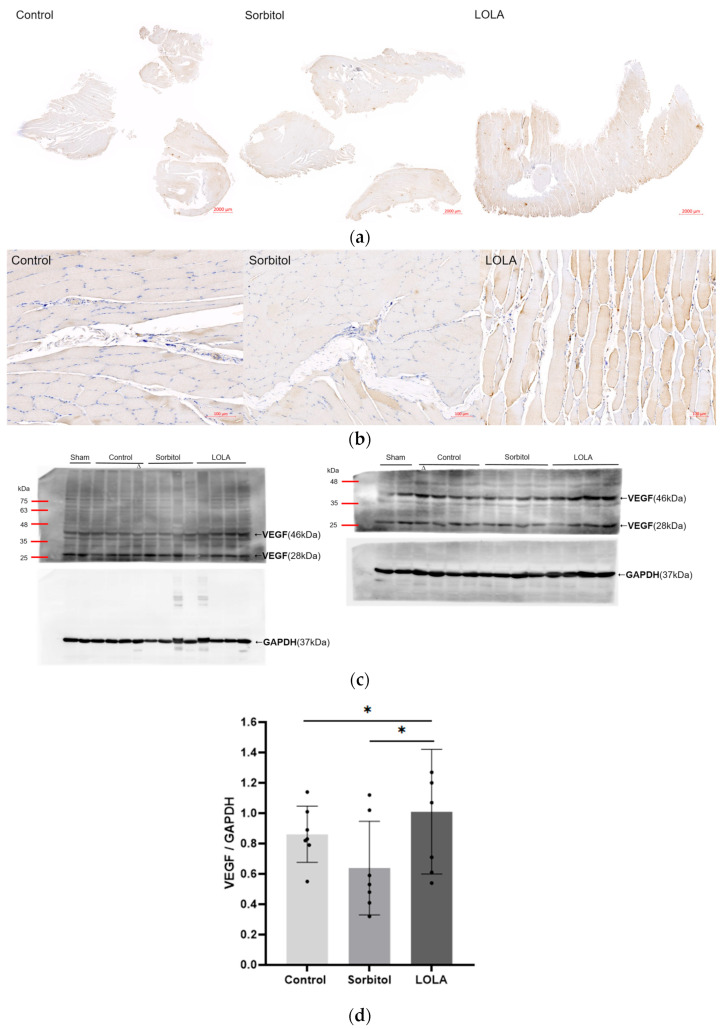 Figure 4
Figure 4- —National Research Foundation of Korea (NRF)
- —Ministry of Science and ICT
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Angiogenesis and VEGF in Cancer · Cerebrovascular and Carotid Artery Diseases
1. Introduction
As global life expectancy increases, the number of elderly people affected by type II diabetes, obesity, and hypertension—established risk factors for atherosclerosis—has also increased. This has led to a rise in the incidence of peripheral arterial disease (PAD), caused by the progression of atherosclerotic plaque, affecting over 230 million adults worldwide [1,2]. Critical limb ischemia (CLI), the advanced stage of PAD, carries significant risks of amputation, stroke, myocardial infarction, and death, resulting in a lower quality of life [3,4].
In the United States alone, about 60,000 major amputations are performed each year, with a global decrease attributed to the increased use of endovascular procedures [5,6]. Endovascular intervention is considered the standard care for patients with peripheral artery disease (PAD), especially for high-risk individuals who are not eligible for open revascularization [7,8]. However, despite the rise in endovascular interventions, the number of minor amputations has increased while major amputations have decreased [9]. The outcomes of surgical or interventional revascularization are not optimal, as repeat interventions and major amputations are still necessary for up to one-third of patients with critical limb ischemia (CLI) treated by revascularization, leaving a significant portion of the population ineligible for these treatments [4,10]. Cilostazol, the only widely approved medication for intermittent claudication, has limited effectiveness and is not recommended for individuals with heart failure, leading to discontinuation by up to half of users due to dizziness or palpitations [11,12,13]. Despite advances in medical therapy, including antiplatelet agents and statins, and improvements in managing comorbidities to enhance limb salvage rates and reduce mortality, the overall survival rate of CLI patients remains lower than that of individuals with other serious conditions like heart failure and certain cancers, averaging around 3.5 years [14,15,16,17]. Considering the limitations of current CLI treatments, therapeutic neovascularization has emerged as a promising option for addressing ischemia, but its clinical application is slow and challenging [18,19].
Nitric oxide (NO) is a well-known regulator of endothelial function, playing a crucial role in endothelial vasorelaxation [20]. NO also upregulates vascular endothelial growth factor (VEGF), a key stimulatory factor for angiogenesis [21,22,23]. Endothelial nitric oxide synthase (eNOS) contributes to collateral arterial adaptation and blood flow recovery in a mouse hind limb ischemia (HLI) model [24]. However, the complex regulation of eNOS expression and activity, involving numerous interrelated mechanisms, currently lacks a clinically applicable treatment [25].
L-Ornithine-L-Aspartate (LOLA), an existing crystalline salt, is currently employed in the clinical management of hepatic encephalopathy [26,27]. L-ornithine can enter the mitochondria and be converted to L-citrulline, while L-aspartate facilitates the conversion of L-citrulline to L-arginine—the sole physiologically significant substrate for NO synthesis [28,29,30,31,32]. There are some reports on the role of L-arginine in angiogenesis in patients with chronically hypoxic lungs and its use as a concomitant treatment for surgical angiogenesis in severe diffuse coronary arterial disease patients [33,34]. However, the long-term administration of L-arginine is not efficient in patients with PAD, even though short-term L-arginine supplementation in patients with CLI induces NO-dependent peripheral vasodilation [35,36]. Although there is no current documentation of the administration of LOLA for CLI treatment, more efficient angiogenesis is expected with LOLA compared to direct administration of L-arginine due to its physiologic production of L-arginine and subsequent NO. Because LOLA is already commercialized with proven safety, there is a high possibility of rapid clinical translation if the efficacy is proven in preclinical studies. Accordingly, this rat model study of HLI is designed to evaluate the efficacy of LOLA as a treatment option for CLI, with the aim of swift translation to human application.
2. Materials and Methods
2.1. Animals
This study was approved by the Institutional Animal Care and Use Committee of the authors’ institute (IACUC-230034) in accordance with the National Institutes of Health Guidelines. This study was carried out in compliance with the ARRIVE guidelines. Male Sprague Dawley rats (Seong-Nam, Republic of Korea) weighing 280–320 g (8 weeks old) were used. The rats were housed in a controlled environment (room temperature 20–24 °C, humidity 40–60%) with access to standard food and water ad libitum during the experiment.
2.2. Hind Limb Ischemia
Anesthesia was administered using 5% isoflurane in O_2_. After anesthesia, analgesia, sedation, and muscle relaxation were performed using intramuscular injection of tiletamine and zolazepam (Zoletil, Virbac, Carros, France) mixed with xylazine (Rompum, Elanco, Indianapolis, IN, USA) (1:1). The concentration of each was 0.7 mg/kg. Then, rats underwent unilateral femoral artery ligation distally to the origin of the deep branch in the right leg. An oblique incision was made with Metzenbaum scissors along the inguinal area. The femoral nerve, artery, and vein were isolated following the removal of the fat pad. The tissue surrounding these structures was dissected using sterile cotton swabs and Graefe forceps. A ligature (4-0 Vicryl) was then tied around the right femoral artery near the inguinal ligament [1,37].
2.3. Protocol
Just before the operations, perfusion imaging was performed. Following the operations, immediate post-op perfusion imaging was performed; post-operative day 0. The rats were then divided into three groups by stratified randomization based on body weight, which was measured by a research assistant. We assigned 7 rats per group: group 1 (control group; injection of normal saline), group 2 (sorbitol group; injection of sorbitol), and group 3 (LOLA treatment group). Normal saline (1.7 mL/kg) in group 1, a mixture of distilled water, sorbitol, and normal saline (20:2:30, 1.7 mL/kg) in group 2, and LOLA (333 mg/kg) (Hepa-Merz infusion, Hanwha Pharma, Chuncheon, Republic of Korea) in group 3 were injected intraperitoneally five times on PODs 3, 5, 7, 10 and 12. Since Herpa-Merz infusion consists of LOLA, sorbitol, and distilled water, an equal amount of sorbitol and distilled water with normal saline instead of LOLA were administrated to group 2. For the control group, an equal amount of normal saline was assigned to group 1. Perfusion imaging was scanned on PODs 7 and 14. Immunohistochemical analysis and Western blotting of gastrocnemius muscles in ischemic limbs were performed after the final perfusion imaging.
2.4. Perfusion Imaging
The anesthesia method employed during surgery was used for each perfusion imaging session. Rats were subjected to imaging for approximately 3 min using a Laser Doppler imager (Moor LDI, Axminster, UK). Images were analyzed with Moor LDI Imaging Review. Regions of interest (ROIs) were drawn around feet and ankles, and perfusion ratios comparing post-operative ischemic limbs with pre-operative limbs were calculated.
2.5. Immunohistochemical Analysis
The rats were euthanized, and their tissues were fixed with 4% paraformaldehyde 14 days after surgery. The muscles were removed, cut into blocks, embedded in paraffin, sectioned at 5 µm using a microtome, and then mounted on glass slides. The sections were incubated for 10 min with Proteinase K enzyme (S3020, Agilent DAKO, Santa Clara, CA, USA) at room temperature as a condition for antibody expression. Blocking was performed with 5% bovine serum albumin for 30 min. Subsequently, the sections were incubated for 1 h with antibodies against VEGF-A165 (1:100, MA1-16629, Thermo Scientific, Waltham, MA, USA) and CD31 (1:100, MA1-80069, Thermo Scientific, Waltham, MA, USA) at room temperature. The sections were then washed three times for 5 min each with Tris-Buffered Saline (TBS) buffer. Following this, the sections were incubated for 20 min at room temperature with a secondary antibody (Envi-112 envision + system-HRP Labeled Polymer—Anti-mouse, K4001, Agilent DAKO, Santa Clara, CA, USA). Subsequent to the incubation, the sections were washed three times for 5 min each with TBS buffer. Digital images of five microscopic fields from four different sections of each animal were captured and viewed using a Zeiss Slide scanner (ZENblue3.1_ZENblack_3-OSR-lite, Carl Zeiss Microscopy, LLC, White Plains, NY, USA; magnification, ×400). Capillary density was determined as the number of CD31-positive cells per square millimeter [38] and confirmed after a consensus review by two medical doctors for each case.
2.6. Western Blotting
Frozen muscle samples were homogenized in RIPA Lysis and Extraction Buffer (Thermo Fisher Scientific, Waltham, MA, USA) with 1% Halt™ Protease Inhibitor Cocktail (Thermo Fisher Scientific, Waltham, MA, USA) and centrifuged at 13,000× g for 15 min at 4 °C. Protein concentrations were determined using a BCA assay kit (cat. no. 23250; Pierce; Thermo Fisher Scientific, Waltham, MA, USA), according to the manufacturer’s instructions. Equal amounts of protein were loaded onto 12% Tris-glycine SDS-Polyacrylamide gels and separated by SDS-PAGE (Bio-Rad, Hercules, CA, USA). Following electrophoresis, the gels were transferred to polyvinylidene difluoride (PVDF) membranes (GenDEPOT, Baker, TX, USA). The membranes were blocked for 1 h at room temperature in TBS (Tris-Buffered Saline) with Tween-20 buffer (Biosolution, Suwon, Republic of Korea) containing 5% bovine serum Albumin (BSA) (bioWORLD, Dublin, OH, USA). Membranes were incubated overnight at 4 °C with primary antibodies against VEGF-A_165_ (MA1-16629; Thermo Fisher Scientific, Waltham, MA, USA) and Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) diluted at a ratio of 1:1000 in 5% BSA-TBS-T. The membranes were washed for 5 min, 5 times with TBS-T buffer, incubated for 1 h at room temperature with Goat Anti-mouse lgG antibody (HRP, GeneTex, Irvine, CA, USA) diluted at a ratio of 1:10,000 in 5% BSA-TBS-T, and washed for 5 min, 5 times with TBS-T buffer. Bands were detected using Clarity™ Western ECL Substrate (Bio-Rad, Hercules, CA, USA). VEGF-A_165_ is typically expressed as a 46 kDa homodimer of 23 kDa subunits [39]. Relative expression of 46 kDa homodimer was normalized to endogenous control GAPDH using ImageJ software version 4.1 (National Institutes of Health, Bethesda, MD, USA).
2.7. Statistical Analysis
Data were presented as the means ± standard deviation. One-way ANOVA test, Fisher’s least significant difference test, and an independent sample t-test were used for statistical analysis. A p-value < 0.05 was considered to indicate a statistically significant difference. The data were analyzed using SPSS software (version 29.0, SPSS, Inc., Chicago, IL, USA).
3. Results
The femoral arteries of two 8-week-old rats were unilaterally ligated to induce hind limb ischemia (HLI) and stimulate angiogenesis, particularly in the gastrocnemius muscle (Figure 1a) [1]. Immediate post-operative perfusion showed an approximate 40% reduction compared to normal pre-operative levels. Subsequently, perfusion increased over the 14-day period, reaching a plateau between weeks three and four at approximately 60% recovery (Figure 1a–c). The duration leading up to this plateau was defined as the perfusion recovery period. Using this model, we examined the alterations in perfusion and microenvironment to assess the impact of LOLA on angiogenesis during the subacute phase of HLI. LOLA was administered five times, starting from POD 3 and continuing for two weeks after surgery (Figure 1d).
3.1. Perfusion Changes
On POD seven, the group administered LOLA (group 3) exhibited a significantly higher perfusion recovery rate compared to the control (group 1) and sorbitol-administered group (group 2) (51.05 ± 10.31 vs. 58.45 ± 18.24 vs. 71.22 ± 14.79; p < 0.05). Although not statistically significant, there was a tendency towards increased perfusion recovery at POD 14 in group 3 compared to the other groups (group 1 vs. group 2 vs. group 3: 62.77 ± 10.10 vs. 60.67 ± 12.45 vs. 72.76 ± 16.09; p = 0.211) (Figure 2).
3.2. Histological Evaluation for Capillary Density
For a more in-depth examination of perfusion differences among the groups, muscle samples on POD 14 underwent immunohistochemistry targeting the endothelial cell marker CD31 to quantify vessel lumen density. The CD31-positive lumen density, indicative of capillary neovascularization, was significantly higher in rats treated with LOLA (group 3) compared to the other groups (157.14 ± 37.25 vs. 162.29 ± 37.53 vs. 352.86 ± 47.80; p < 0.001) (Figure 3).
3.3. Expression of VEGF
The levels of VEGF expression in the ischemic limb, as determined by Western blotting on POD 14, were notably higher in rats treated with LOLA (group 3) compared to the other groups (group 1 vs. group 2 vs. group 3: 0.86 ± 0.17 vs. 0.64 ± 0.28 vs. 1.01 ± 0.38; p < 0.05). Compared to the other groups, group 3’s immunohistochemical staining for VEGF was also enhanced (Figure 4).
4. Discussion
Our study using a rat model with LOLA administration demonstrated a significant increase in perfusion in the ischemic limb, high CD31-positive capillary lumen density, and substantial overexpression of VEGF during the subacute phase of HLI.
The pharmacokinetic and pharmacodynamic properties of LOLA are well-established in hepatic encephalopathy and it is already commercialized [26,27,40]. Our interest in the angiogenetic effect of L-arginine in patients with chronically hypoxic lung and asthma, along with endothelial modulation in patients with severe diffuse coronary arterial disease, prompted our investigation [33,34,41]. LOLA increases L-arginine via the conversion of L-ornithine, which is crucial for nitric oxide (NO) synthesis [28,29,30,31,32]. NO plays a vital role in angiogenesis by upregulating the vascular generation of VEGF and coordinating with FGF-induced angiogenesis [21,22,23,41,42]. Endothelial nitric oxide synthase (eNOS) is critical for ischemic remodeling and collateral arterial adaptation, leading to flow recovery in the hind limb ischemia (HLI) mouse model [24,43]. Recent research indicates that aspartate regulates endothelial translation machinery for VEGFR2 and FGFR1 synthesis via mTORC1 [44]. Long-term administration of L-arginine inhibits atherosclerosis and myointimal hyperplasia while enhancing angiogenesis in preclinical studies [45,46,47]. Additionally, short-term L-arginine supplementation in patients with cardiovascular risk factors has been shown to increase NO synthesis and improve vasoreactivity [35]. Consistent with these studies, the administration of LOLA increased the expression of VEGF and promoted angiogenesis in our CLI model. However, long-term administration of L-arginine in patients with PAD does not increase NO synthesis or improve vascular reactivity and may even pose a risk of harm [36]. Unlike administering arginine directly, LOLA induces an increase in arginine by adding reactants in the urea cycle, which may result in greater physiological efficacy and safety. Therefore, further long-term study with LOLA in the CLI model is necessary.
We believe it is challenging to uniformly apply methods and results from a specific mouse or rat model to other mouse or rat HLI models due to different perfusion recovery patterns dependent on the rate of arterial occlusion in mice and rats, as well as varying tissue necrosis in mouse strains [1,48,49,50]. Therefore, the HLI model and protocol in this study were designed to align with our hypotheses and aims. Unilateral proximal femoral artery ligation, without total excision or coagulation of its branches, allowed sufficient reperfusion between PODs 7 and 14, making it suitable for evaluating angiogenesis in the calf muscle [1]. Perfusion imaging was conducted solely on the ischemic hind limb without comparison to the non-ischemic contralateral limb. This approach aligns with the need for quantitative perfusion imaging in the affected lower extremity of CLI patients before and after revascularization [51]. Immediate post-operative perfusion in our HLI model experienced a 40% reduction compared to normal pre-operative levels. Subsequently, perfusion increased over 14 days, reaching a plateau between weeks three and four at approximately 60% recovery without any treatment, resembling the recovery pattern seen in a previous mouse HLI model [52]. While the 60% perfusion recovery plateau does not fully meet the diagnostic criteria of CLI in humans, it falls within at least a moderate degree of PAD [51,53]. Hepa-Merz can be administered to patients with hepatic encephalopathy, usually up to four ampoules daily (5 g per ampoule). If the patient is in a pre-coma state, the dose can be increased up to eight ampoules/24 h with a maximum infusion rate of 5 g/h, depending on the severity of the condition. This means that 308–615 mg/kg of Hepa-Merz can be administered per day for a 65 kg adult. Unfortunately, there is no standardized dosage of Herpa-Merz for administration to rat CLI models. Thus, the LOLA dosage was determined based on previous toxicity reports in Sprague Dawley rats (lethal dose 50%: 4.7 g/kg, no systemic toxicity between 1 and 4 g/kg) and the usual dosage for human application [27,54,55].
In the clinical setting, physicians encounter challenges in selecting an optimal treatment for patients with CLI due to a lack of high-level evidence to guide clinical decision-making [17,56,57,58,59,60]. Currently, endovascular revascularization is preferred for CLI due to lower morbidity and mortality compared to open surgery. However, the greater need for reinterventions in endovascular procedures results in a loss of cost-effectiveness [8,61,62]. Despite the increased use of endovascular interventions, overall amputation rates have not significantly improved [9,63]. Among promising gene therapies, hepatocyte growth factor—despite being the closest to human application—faced setbacks, as seen in the terminated phase III AnGes trial (ClinicalTrials.gov: NCT02144610) [17,64,65]. Various cell therapies, including bone marrow-derived mononuclear cells and mesenchymal stromal cells, studied in CLI, have shown no clinical efficacy to date [66,67]. Human pluripotent stem cell-derived endothelial cells, a potential candidate for cell therapy in CLI, have not yet entered clinical trials [68]. Hence, our study aimed to identify a drug for CLI treatment by leveraging a substance already in use for other human diseases, facilitating easier clinical application. A clinical trial with short-term and long-term administration of LOLA can be conducted, similar to previous studies on PAD with L-arginine. In addition, since LOLA is currently used for the clinical management of hepatic encephalopathy, we can assess the change in perfusion in the lower extremities of patients with hepatic encephalopathy and concurrent PAD after LOLA administration. The significantly lower cost of LOLA compared to endovascular interventional procedures or surgical bypass makes it an attractive option for clinical application, particularly given its established safety in managing hepatic encephalopathy. If further preclinical studies confirm LOLA’s feasibility in treating PAD based on the results of this study, clinical trials for LOLA administration will be actively pursued by investigators.
This study is subject to various limitations. Firstly, we exclusively examined the subacute phase of critical limb ischemia (CLI), and further investigation into the effects of LOLA on the chronic stage is warranted. Secondly, we did not include a robust mechanism of action study to couple with potential mechanisms for LOLA’s effects on angiogenesis and perfusion recovery, which is essential and should be pursued in subsequent research. We measured NO levels in samples from gastrocnemius muscles and plasma two days after the last LOLA injection. However, there was no significant difference between the three groups. Consequently, we speculate that L-arginine, L-citrulline, or NOS3 expression would yield similar results. We believe the interval between the last injection and sampling might have been too long. Therefore, we plan to conduct a future mechanistic study with a shorter interval, within 24 h, to evaluate the NO balance. Thirdly, we did not employ variable doses of LOLA, a consideration that will be essential for subsequent clinical trials. Fourthly, our study’s sample size was small, which may affect the power of the results. While our emphasis was on addressing the immediate requirements of CLI using a clinically available drug, future research should include preclinical investigations into the long-term administration of LOLA and clinical trials.
5. Conclusions
This study provides the first evidence of angiogenesis and improved blood flow during the subacute phase of hind limb ischemia using LOLA. Due to LOLA’s commercial availability, the application of LOLA treatment for PAD can be initiated more rapidly than other therapies that are still being developed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aref Z. de Vries M.R. Quax P.H.A. Variations in Surgical Procedures for Inducing Hind Limb Ischemia in Mice and the Impact of These Variations on Neovascularization Assessment Int. J. Mol. Sci.201920370410.3390/ijms 2015370431362356 PMC 6696155 · doi ↗ · pubmed ↗
- 2Criqui M.H. Matsushita K. Aboyans V. Hess C.N. Hicks C.W. Kwan T.W. Mc Dermott M.M. Misra S. Ujueta F. Lower Extremity Peripheral Artery Disease: Contemporary Epidemiology, Management Gaps, and Future Directions: A Scientific Statement From the American Heart Association Circulation 2021144 e 171e 19110.1161/CIR.000000000000100534315230 PMC 9847212 · doi ↗ · pubmed ↗
- 3Tebebi P.A. Kim S.J. Williams R.A. Milo B. Frenkel V. Burks S.R. Frank J.A. Improving the therapeutic efficacy of mesenchymal stromal cells to restore perfusion in critical limb ischemia through pulsed focused ultrasound Sci. Rep.201774155010.1038/srep 4155028169278 PMC 5294408 · doi ↗ · pubmed ↗
- 4Lv S. Cai H. Xu Y. Dai J. Rong X. Zheng L. Thymosin-beta 4 induces angiogenesis in critical limb ischemia mice via regulating Notch/NF-kappa B pathway Int. J. Mol. Med.202046134713583294535710.3892/ijmm.2020.4701 PMC 7447324 · doi ↗ · pubmed ↗
- 5Kim T.I. Mena C. Sumpio B.E. The Role of Lower Extremity Amputation in Chronic Limb-Threatening Ischemia Int. J. Angiol.20202914915510.1055/s-0040-171007532904807 PMC 7458760 · doi ↗ · pubmed ↗
- 6Egorova N.N. Guillerme S. Gelijns A. Morrissey N. Dayal R. Mc Kinsey J.F. Nowygrod R. An analysis of the outcomes of a decade of experience with lower extremity revascularization including limb salvage, lengths of stay, and safety J. Vasc. Surg.201051878885.e 87110.1016/j.jvs.2009.10.10220045618 · doi ↗ · pubmed ↗
- 7Mustapha J.A. Finton S.M. Diaz-Sandoval L.J. Saab F.A. Miller L.E. Percutaneous Transluminal Angioplasty in Patients With Infrapopliteal Arterial Disease: Systematic Review and Meta-Analysis Circ. Cardiovasc. Interv.20169 e 00346810.1161/CIRCINTERVENTIONS.115.00346827162214 · doi ↗ · pubmed ↗
- 8Kinlay S. Management of Critical Limb Ischemia Circ. Cardiovasc. Interv.20169 e 00194610.1161/CIRCINTERVENTIONS.115.00194626858079 PMC 4827334 · doi ↗ · pubmed ↗