Adult-Onset Still’s Disease with Distinctive Skin Signs and Elevated LDH
Eleni Klimi, Evaggelia Kataxaki

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1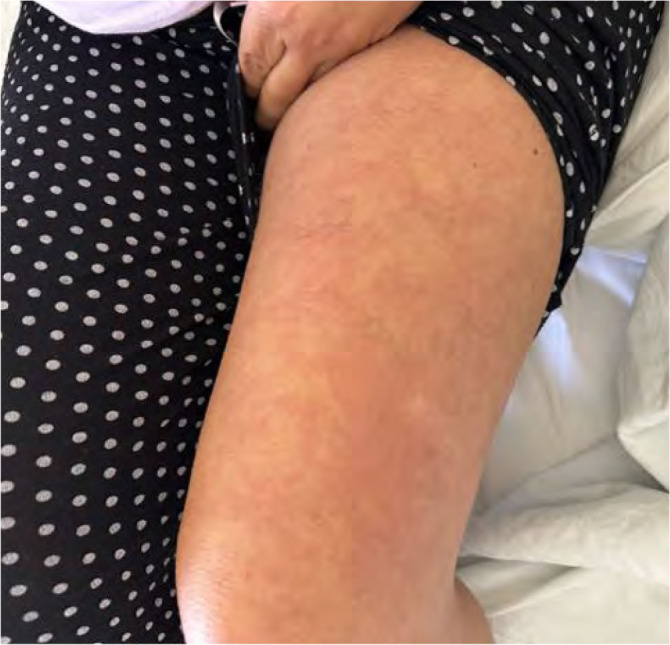 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders Research · Otitis Media and Relapsing Polychondritis · Immune Cell Function and Interaction
Adult-onset Still’s disease (AOSD) is a rare, inflammatory disorder characterised by the appearance of fever and salmon-patch like lesions, that may affect multiple organs and joints, including the liver and spleen. The disease responds to the administration of steroids, although biological agents have been used in the treatment of recalcitrant cases. Recently, some cases presenting atypical skin signs have been reported in literature. Herein, we describe such a case which, apart from the typical salmon-patch rash, presents erythematous urticarial papules lesions that coalesce to form plaques in the extremities. In addition, elevated LDH in the serum is a laboratory finding suggestive of a worse prognosis.
A 45-year-old woman was hospitalised in the Department of Internal Medicine with a 39^o^C fever and a rash that had appeared 4 days prior to the consultation. No intake of medications was reported by the patient. Their family history includes systemic lupus erythematosus in the mother and coeliac disease in two of the children – a son and a daughter. A dermatological consultation was requested. The clinical examination revealed salmon-like patches on the back (Figure 1) and erythematous papules that coalesce to form urticarial-like plaques on both thighs (Figure 2). Pruritus and arthralgias were not reported. The laboratory findings were leukopenia, abnormal hepatic enzymes, abnormal ESR, abnormal CRP. Haemocultures and urine cultures were sterile. The strep test from the throat and antistreptolysin-O (ASTO) were negative.
Serology for Ebstein-Barr, Coxsackie, Echo, HIV1,2 and COVID-19 also proved negative. Anti-nuclear antibody and rheumatoid factor were negative (Table 1). Thorax radiography was normal. Echography of the abdomen revealed splenomegaly.
A skin biopsy was proposed but refused by the patient. A clinical suspicion of AOSD was raised and methylprednisolone at the dose of 1 mgr/kgr was started, resulting in improvement of the skin lesions and apyrexia. Two weeks later following the administration of steroids, the skin lesions and fever were completely resolved, with no recurrence during the tapering of the steroids period. Described initially by George Still in children, the adult form of the disease defined in 1971 by Eric Bywaters is a rare inflammatory condition that manifests with rash, fever, and multiple internal organ involvement.^1^ It belongs to autoinflammatory syndromes.^2^ Its aetiology is unknown, although some cases have been triggered by COVID-19 infection^3^ and/or vaccination.4 The diagnostic criteria for adult-onset Still’s disease are those of Yamaguchi^5^ (Table 2).
Differential diagnoses include viral exanthems, drug eruption, and lymphoma. It may be complicated by internal organ involvement and macrophage activation syndrome.^6^
In the case reported, the diagnosis of AOSD was established due to the presence of a rash, a 39^o^ C fever, splenomegaly, liver dysfunction, and the negativity of rheumatoid factor and antinuclear antibody. Thus, five criteria were present, two of them being major. Liver dysfunction exhibited by elevated enzyme levels could be attributed to hypercytokinaemia (increased levels of interleukins circulating in the serum). In addition, hyper-cytokinaemia is detected in haemophagocytic syndrome, that may complicate AOSD. No re-evaluation of the liver tests was attempted.
Recently, several cases with atypical cutaneous manifestations have been reported in literature. One such case has been reported by Jeong Woo Seong et al. It was a case of AOSD in a 77-year-old woman with erythematous coalescent figurate, oedematous popular plaques over the lower lumbar region.^7^ Bhatia R et al. reported a case of flagellate erythema in a primigravida with AOSD.^8^ Another case of AOSD with atypical skin signs is reported by Camporro Angel Fernandez et al. who reported two cases of Still’s disease, one in a paediatric patient and one in an adult with dermatomyositis-like eruption.^9^ The case reported here, in addition to the typical salmon patch–like rash on the back, presents erythematous papules which coalesce to form erythematous urticarial-like plaques on both thighs. The emergence of urticarial-like lesions might be due to the circulation of interleukins in the serum that attract polynuclear and other inflammatory cells in the epidermis. Lactate dehydrogenase (LDH) is usually elevated in patients with AOSD, yet the presence of high LDH in the serum is suggestive of a worse prognosis.^10^ Although steroids are effective treatment in most patients with AOSD, methotrexate and/or biological agents may be necessary in some cases. This case of AOSD has been reported to increase awareness about cases of AOSD which combine typical with atypical clinical signs- an urticarial-like eruption, a clinical rarity in association with high LDH, a factor suggestive of a worse prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Elhawary RA Nadeem M Abdelwahed MS Somaily M Alemam SY. Adult-Onset Still’s Disease with Dermatopathic Lymphadenitis Clinicopathologic Features: A Rare Case Report and Review of the Literature. Case Reports Immunol 2022 Jun 3;2022:1653683. doi: 10.1155/2022/1653683. PMID: 35693913; PMCID: .35693913 PMC 9187476 · doi ↗ · pubmed ↗
- 2Bonnekoh H Krusche M Feist E Wagner AD Pankow A. Autoinflammatorische Syndrome [Autoinflammatory syndromes]. Inn Med (Heidelb) 2023 May;64(5):442–451. [In German] doi: 10.1007/s 00108-023-01505-1. Epub 2023 Apr 28. PMID: 37115240; PMCID: .37115240 PMC 10140729 · doi ↗ · pubmed ↗
- 3Achour TB Elhaj WB Jridi M Naceur I Smiti M Ghorbel IB Adult-onset Still’s disease after SARS-Cov-2 infection. Clin Case Rep 2023 Mar 2;11(3):e 7006. doi: 10.1002/ccr 3.7006. PMID: 36873075; PMCID: .36873075 PMC 9979958 · doi ↗ · pubmed ↗
- 4Albertino LF Moulaz IR Zogheib TF Valentim MZC Machado KL. Adult-onset Still’s disease after Ch Ad Ox 1 n Co V-19 vaccine: a possible association. Autops Case Rep 2022 Nov 7;12:e 2021403. doi: 10.4322/acr.2021.403. PMID: 36426114; PMCID: .36426114 PMC 9675091 · doi ↗ · pubmed ↗
- 5Efthimiou P Kontzias A Hur P Rodha K Ramakrishna GS Nakasato P. Adult-onset Still’s disease in focus: Clinical manifestations, diagnosis, treatment, and unmet needs in the era of targeted therapies. Semin Arthritis Rheum 2021 Aug;51(4):858–874. doi: 10.1016/j.semarthrit.2021.06.004. Epub 2021 Jun 13. PMID: 34175791.34175791 · doi ↗ · pubmed ↗
- 6Ding Y Tang S Li S Yang C Liu T Ying S Risk of macrophage activation syndrome in patients with adult-onset Still’s disease with skin involvement: A retrospective cohort study. J Am Acad Dermatol 2021 Dec;85(6):1503–9. doi: 10.1016/j.jaad.2021.02.005. Epub 2021 Feb 5. PMID: 3355641233556412 · doi ↗ · pubmed ↗
- 7Jeong WS Kim J Heo ST Kim JW Yoo JR. Atypical cutaneous features in a patient with adult-onset Still’s disease. Korean J Intern Med 2021 May;36(3):742–3. doi: 10.3904/kjim.2019.389. Epub 2020 Apr 3. PMID: 32229797; PMCID: .32229797 PMC 8137391 · doi ↗ · pubmed ↗
- 8Bhatia R Kaeley N Kant R Basi A. Fever with persistent flagellate erythema in a primigravida: a rare presentation of adult-onset Still’s disease. BMJ Case Rep 2019 Jul 12;12(7):e 229332. doi: 10.1136/bcr-2019-229332. PMID: 31302619; PMCID: 31302619 PMC 6626490 · doi ↗ · pubmed ↗