Unexpected Culprit: A Case Report of Pleuropulmonary Pantoea septica Infection in a Ketamine User
Pyae Kyaw, Nava R Sharma, Khin Soe, Yu Shia Lin, Shaurya Sharma

TL;DR
A 30-year-old man with a history of ketamine abuse developed a rare lung infection caused by Pantoea septica, highlighting a possible link between drug use and unusual infections.
Contribution
This case report identifies ketamine abuse as a potential risk factor for Pantoea septica pulmonary infection in otherwise healthy individuals.
Findings
Pantoea septica caused multifocal cavitary pneumonia and parapneumonic effusions in a ketamine user.
The patient responded to intravenous antibiotics and pleural drainage.
The case suggests a possible immunomodulatory effect of ketamine increasing susceptibility to rare pathogens.
Abstract
Pantoea septica, a gram-negative bacillus typically associated with opportunistic bloodstream infections in neonatal intensive care units, rarely causes pulmonary infections in immunocompetent individuals. We present a case of a 30-year-old male with multifocal cavitary pneumonia, bilateral parapneumonic effusions, and positive blood cultures for Pantoea septica, occurring in the setting of prior ketamine abuse. The patient presented with fever, productive cough, chest pain, and worsening dyspnea, without significant medical history or immunocompromising conditions. Diagnostic evaluation revealed elevated inflammatory markers, characteristic radiographic findings, and successful treatment with intravenous antibiotics and pleural drainage. This case highlights the diagnostic challenge posed by Pantoea septica in pulmonary infections and suggests a potential link between ketamine abuse…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
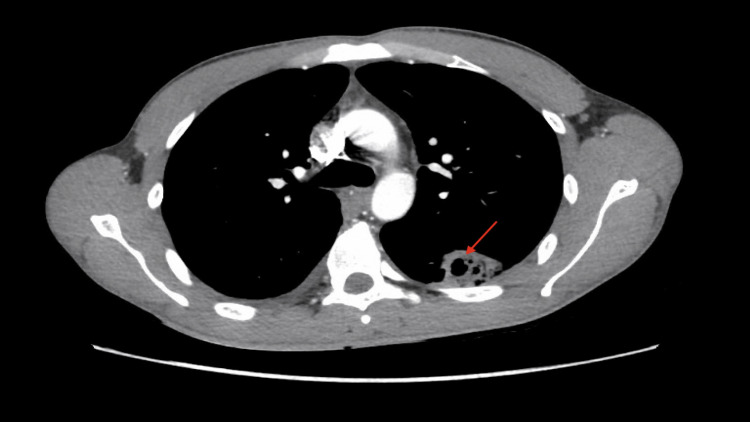 Figure 1
Figure 1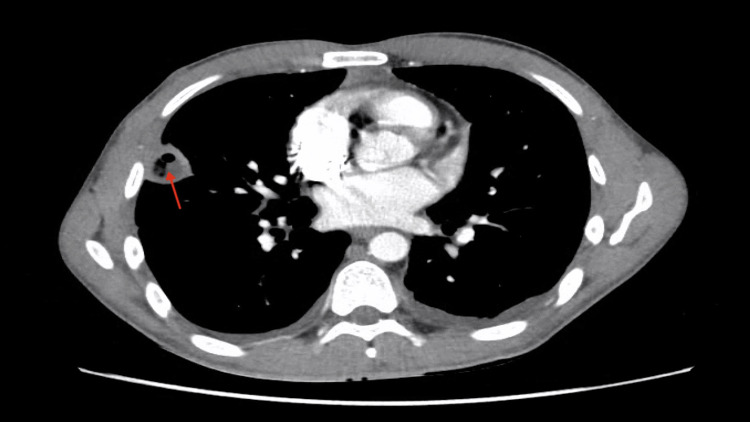 Figure 2
Figure 2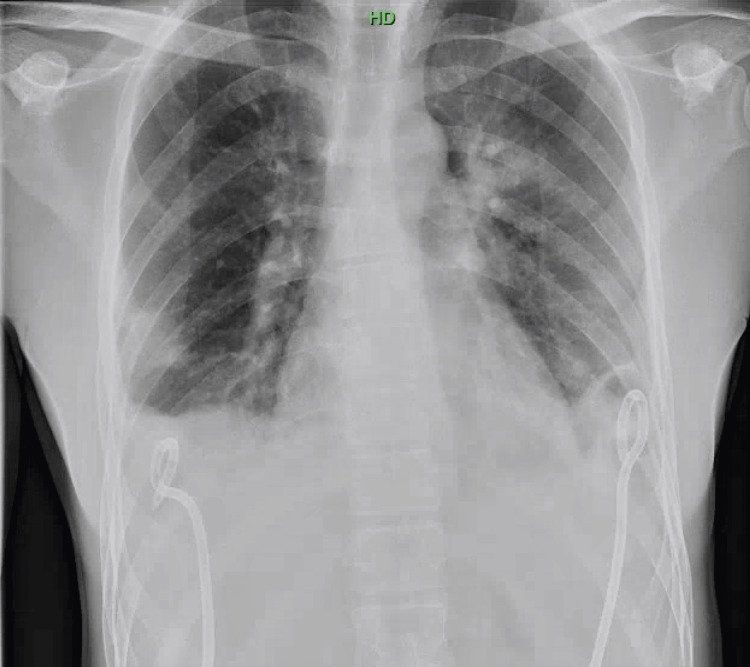 Figure 3
Figure 3| Test | Result | Normal range |
| Adenosine deaminase | 15 U/L | <15 |
| Albumin, fluid | 2.1 g/dL | 2.1 - 2.5 |
| Amylase, fluid | 20 U/L | 16 and higher |
| Glucose, fluid | 56 mg/dL | 56 - 103 |
| Lactate dehydrogenase, fluid | 1336 U/L | 144 and higher |
| Specific gravity, fluid | 1.015 | 1.015 - 1.020 |
| Total protein, fluid | 4.1 g/dL | 4.1 - 5.0 |
| Fluid color | Yellow | Yellow |
| Fluid appearance | Cloudy | Cloudy |
| Fluid WBC | 2354/mm³ | - |
| Fluid RBC | 14000/mm³ | - |
| Fluid neutrophil | 93% | - |
| Fluid lymphocyte | 7% | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPlant Pathogenic Bacteria Studies · Enterobacteriaceae and Cronobacter Research · Escherichia coli research studies
Introduction
Pantoea species are gram-negative bacilli with peritrichous flagella, part of the Enterobacteriaceae family known for opportunistic infections in healthcare settings, particularly in neonatal intensive care units causing bloodstream infections [1]. However, they are rarely identified as primary pathogens in pulmonary infections among immunocompetent individuals. Pantoea exhibits a diverse ecological range, thriving in various environments, including plants, animals, soil, and water, highlighting its adaptability and potential pathogenicity under specific conditions [2,3].
Clinical understanding of Pantoea septica infections in pulmonary settings is limited, typically affecting immunocompromised patients or those with significant environmental exposures. Pulmonary infections caused by Pantoea septica present diagnostic challenges due to their unusual presentation and resemblance to more common pathogens [1]. This case describes a young male presenting with multifocal cavitary pneumonia and bilateral parapneumonic effusions, with blood cultures positive for Pantoea septica. His history of ketamine abuse prompted an investigation into the potential immunomodulatory effects of ketamine on pulmonary defenses and its role in predisposing individuals to infections by uncommon pathogens like Pantoea septica. Clarifying the relationship between ketamine abuse and susceptibility to gram-negative infections, including Pantoea septica, is crucial for managing similar clinical presentations and warrants further investigation into host immune responses and bacterial pathogenesis in such cases.
Case presentation
A 30-year-old male presented to the emergency department with a one-week history of fever, productive cough, chest pain, and worsening dyspnea. Upon initial examination, he appeared acutely ill with a temperature of 101.3°F, heart rate of 94 beats per minute, respiratory rate of 18 per minute, and blood pressure of 112/66 mmHg. He denied any significant medical history, recent sick contacts, or exposure to pets, and reported working as a sushi chef.
Laboratory investigations revealed a markedly elevated white blood cell count of 32,000/μL, predominantly neutrophilic (86%) with 3% band cells. His hemoglobin level was 12.6 g/dL, and his platelet count was 332,000/μL. Further diagnostic workup, including a comprehensive metabolic panel, legionella antigen testing, fungal infection markers, and HIV testing, returned negative results. A chest computed tomography (CT) scan demonstrated bilateral pleural effusions and cavitary lesions consistent with pneumonia and lung abscesses, as shown in Figures 1, 2.
Red arrow showing cavitary lesion in the lung base.The CT scan revealed multiple discrete cavitating lesions (as shown by the red arrow) in both lungs, accompanied by several small non-cavitating lesions. Additionally, there were moderate-sized pleural effusions bilaterally, with multiple loculations within the pleural effusions.
Red arrow showing cavitary lesion.A red arrow indicates a cavitary lesion located adjacent to the pleura. This lesion is accompanied by several small non-cavitating lesions along the peripheral surface adjacent to the pleura.
Blood cultures collected on admission showed the growth of a gram-negative organism by day two, later identified as Pantoea septica. Transthoracic echocardiography did not reveal any valvular abnormalities or vegetations, ruling out infective endocarditis. Due to the presence of bilateral pleural effusions, interventional radiology was consulted for drainage, and bilateral chest tubes were inserted, as shown in Figure 3. Analysis of the pleural fluid revealed an exudative effusion with a normal adenosine deaminase level. Cultures of pleural fluid for bacterial, mycobacterial, and fungal pathogens yielded no growth, and cytological examination did not detect malignant cells. The pleural fluid analysis result is shown in Table 1.
Bilateral chest tube.The image demonstrates the interval placement of bilateral chest pigtail catheters for the management of pleural effusions. There is no evidence of pneumothorax.
Initial antibiotic therapy comprised intravenous cefepime and metronidazole, which was later switched to intravenous ceftriaxone upon identification of Pantoea septica in blood cultures, targeting the bacteremia. The patient responded well to treatment, evidenced by minimal chest tube output and clinical improvement. He was discharged on hospital day 12 with a course of oral amoxicillin-clavulanic acid and scheduled for follow-up in the infectious disease clinic.
This case underscores the diagnostic challenge posed by Pantoea septica as a rare pathogen causing severe pleuropulmonary infections, particularly in the absence of typical risk factors or immunocompromised states. The management highlights the importance of timely intervention with appropriate antibiotic therapy and therapeutic drainage in achieving clinical resolution.
Discussion
Pantoea septica, a gram-negative bacterium characterized by its motile, unencapsulated morphology and peritrichous flagella, typically manifests as an opportunistic pathogen, primarily associated with bloodstream infections in neonatal intensive care units and rarely implicated in pulmonary infections among immunocompetent individuals [1]. The presented case underscores a unique instance of Pantoea septica causing multifocal cavitary pneumonia and bilateral parapneumonic effusions in a 30-year-old male with a history of ketamine abuse. This association raises intriguing questions regarding the pathogenesis of Pantoea septica in the pulmonary system, particularly in the context of immunocompetence and environmental exposures such as recreational drug use [2-4].
Clinical manifestations in our patient included a one-week history of fever, productive cough, and worsening dyspnea, alongside significant laboratory findings of elevated neutrophil count and radiographic evidence of pleural effusions and cavitary lesions on chest CT. Diagnosis relied heavily on blood cultures that yielded Pantoea septica, corroborated by pleural fluid analysis showing exudative effusion without evidence of alternative pathogens [4,5]. Notably, the patient’s occupation as a sushi chef and the history of ketamine use provided contextual clues, suggesting potential occupational or recreational exposures predisposing to this uncommon pulmonary infection.
Although no literature directly links ketamine use to Pantoea septica pneumonia, studies suggest that ketamine can increase susceptibility to gram-negative infections. Evidence indicates that long-term ketamine use may lead to an immunocompromised state [6-8].
The role of ketamine in modulating immune responses, particularly its reported suppression of pro-inflammatory cytokine production and nuclear factor kappa B (NF-kB) activity in pulmonary cells, merits consideration in this case [7]. In our patient's case, prolonged ketamine use likely contributed to a weakened immune system, predisposing them to Pantoea infection [6,7]. However, the precise mechanisms behind this association are not well-documented in the literature. To better understand the relationship between ketamine abuse and increased infection vulnerability, further research is essential [9,10].
Numerous reports of Pantoea infections have included susceptibility tests, showing that the bacteria are often sensitive to antibiotics such as amikacin, gentamicin, meropenem, ciprofloxacin, levofloxacin, amoxicillin/clavulanate, and broad-spectrum cephalosporins like ceftazidime and cefepime [10]. Conducting susceptibility testing is highly valuable for selecting the appropriate antibiotic treatment [9].
Treatment encompassed initial empiric therapy with intravenous cefepime and metronidazole, later adjusted to ceftriaxone upon culture confirmation of Pantoea septica in our case. Interventional radiology facilitated drainage of pleural effusions through bilateral chest tubes, leading to clinical improvement and eventual discharge with oral antibiotics. This case highlights the importance of prompt diagnosis, multidisciplinary management, and targeted antimicrobial therapy in achieving favorable outcomes in severe pleuropulmonary infections caused by uncommon pathogens like Pantoea septica.
In conclusion, while rare, infections caused by Pantoea septica should be considered in the differential diagnosis of severe pulmonary presentations, particularly in individuals with unique occupational or recreational exposures.
Conclusions
Severe pulmonary conditions should raise suspicion for Pantoea species infections, especially among individuals with specific occupational or recreational exposures, highlighting the need for inclusion in differential diagnoses. The association with ketamine use underscores broader public health implications, urging heightened awareness and further investigation into the immunological consequences of recreational drug abuse on infectious disease susceptibility. This case prompts ongoing research efforts aimed at elucidating preventive measures and therapeutic strategies tailored to mitigate such risks in vulnerable populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pantoea infections in the neonatal intensive care unit Cureus Mani S Nair J 013202110.7759/cureus.13103 PMC 788616333643749 · doi ↗ · pubmed ↗
- 2Pantoea agglomerans: an elusive contributor to chronic obstructive pulmonary disease exacerbation Cureus Shrestha B K CN Bastola C 013202110.7759/cureus.18562 PMC 857180234760410 · doi ↗ · pubmed ↗
- 3A case of bilateral endogenous Pantoea agglomerans endophthalmitis with interstitial lung disease Korean J Ophthalmol Seok S Jang YJ Lee SW Kim HC Ha GY 2492512420102071439110.3341/kjo.2010.24.4.249PMC 2916109 · doi ↗ · pubmed ↗
- 4Pantoea agglomerans chronic exposure induces epithelial-mesenchymal transition in human lung epithelial cells and mice lungs Ecotoxicol Environ Saf Lemieszek MK Rzeski W Golec M Mackiewicz B Zwoliński J Dutkiewicz J Milanowski J 11041619420203214619210.1016/j.ecoenv.2020.110416 · doi ↗ · pubmed ↗
- 5Characteristics and accurate identification of Pantoea dispersa with a case of spontaneous rupture of hepatocellular carcinoma in China: a case report Medicine (Baltimore) Yang Y Hu H Zhou C 0101202210.1097/MD.0000000000028541 PMC 875802835029210 · doi ↗ · pubmed ↗
- 6Ketamine and peripheral inflammation CNS Neurosci Ther De Kock M Loix S Lavand'homme P 4034101920132357463410.1111/cns.12104 PMC 6493703 · doi ↗ · pubmed ↗
- 7Mechanisms of ketamine-induced immunosuppression Acta Anaesthesiol Taiwan Liu FL Chen TL Chen RM 1721775020122338504010.1016/j.aat.2012.12.001 · doi ↗ · pubmed ↗
- 8The effect of ketamine anesthesia on the immune function of mice with postoperative septicemia Anesth Analg Takahashi T Kinoshita M Shono S Habu Y Ogura T Seki S Kazama T 1051105811120102070578910.1213/ANE.0b 013e 3181 ed 12fc · doi ↗ · pubmed ↗