Multiple Brown Tumors in Primary Hyperparathyroidism
Abrar Ali Chhachhar, Muhammad Qamar Masood

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
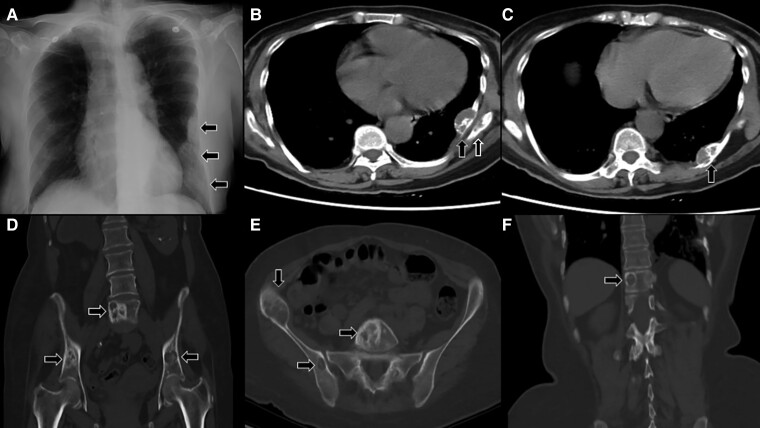 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Medical Imaging and Pathology Studies · Pancreatic and Hepatic Oncology Research
Image Legend
A 58-year-old woman with history of renal stones was evaluated after her chest radiograph incidentally revealed left pleural lesions (Fig. 1A). Computed tomography revealed multiple mixed sclerotic and lytic expansile lesions in the left eighth, ninth, and tenth ribs (Fig. 1B and 1C). Similar lesions were seen in the scapula (Fig. 1B), pelvic bones, and vertebra (Fig. 1D and 1E). On laboratory investigations, calcium was 12.6 mg/dL (3.15 mmol/L) (normal range [NR], 8.6-10.2 mg/dL [2.15-2.55 mmol/L]), phosphate was 4.4 mg/dL (1.42 mmol/L) (NR, 2.51-4.50 mg/dL [0.81-1.45 mmol/L]), and parathyroid hormone (PTH) level was 804 ng/L (16-87 ng/L). Ultrasound neck localized a large parathyroid adenoma at the lower left thyroid lobe. The patient underwent parathyroidectomy and histopathology revealed fat-depleted parathyroid tissue with a solid pattern of predominantly chief cells and focal oxyphil cells, confirming parathyroid adenoma. Confirmation of hyperparathyroidism established the diagnosis of brown tumors (BTs). Postoperative PTH was less than 3 ng/L. Despite the successful parathyroidectomy, the patient later died of an unrelated critical illness. BTs, rare variants of osteitis fibrosa cystica, are nonmalignant tumors of the giant cell family caused by high PTH, resulting in cystic fibrous tumors of the bone [1]. Radiologically often misunderstood as malignant lesions, BTs are diagnosed clinically in hyperparathyroidism as they cannot be distinguished from other giant cell lesions due to histological similarities [2]. This case emphasizes recognition of BTs in primary hyperparathyroidism.
A, Pleural lesions involving eighth, ninth, and tenth ribs. B, Mixed sclerotic and lytic lesions with cortical expansion in the scapula and left ninth rib (39 × 15 mm) near angle of the rib. C, Mixed sclerotic and lytic lesion in left tenth rib (30 × 16.4 mm) posteriorly. D and E, Multiple expansile mixed solid and lytic lesions in both iliac bones and L5 vertebral body. F, A lytic lesion of T11 vertebral body.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shavlokhova V, Goeppert B, Gaida MM, et al Mandibular brown tumor as a result of secondary hyperparathyroidism: a case report with 5 years follow-up and review of the literature. Int J Environ Res Public Health. 2021;18(14):7370.34299820 10.3390/ijerph 18147370 PMC 8304219 · doi ↗ · pubmed ↗
- 2Zhou Z, Shi Y, Li C, Wang W. Primary hyperparathyroidism-induced brown tumors caused by parathyroid carcinoma: a case report and literature review. J Int Med Res. 2022;50(9):03000605221123668.