Emergence of acute quadriparesis in a young patient following myocardial infarction. A case report
Sajjad Daneshyar, Mojtaba Khazaei, Mozhgan Nazifi

TL;DR
A young patient developed sudden muscle weakness after a heart attack, highlighting the connection between heart and brain issues in those with rheumatoid arthritis.
Contribution
This case report emphasizes the complex interplay between rheumatoid arthritis, myocardial infarction, and neurological complications.
Findings
The patient experienced acute quadriparesis following a myocardial infarction.
Rheumatoid arthritis was identified as a contributing factor to the patient's complex medical condition.
The case underscores the importance of interdisciplinary care in managing such patients.
Abstract
Cerebrovascular events are closely related to cardiac events. Chronic inflammatory diseases, such as rheumatoid arthritis (RA), increase the risk of cardiovascular and cerebrovascular stroke. The link between RA, myocardial infarction, and resulting neurological issues highlights the case's complexity, stressing the need for a comprehensive, interdisciplinary medical approach.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
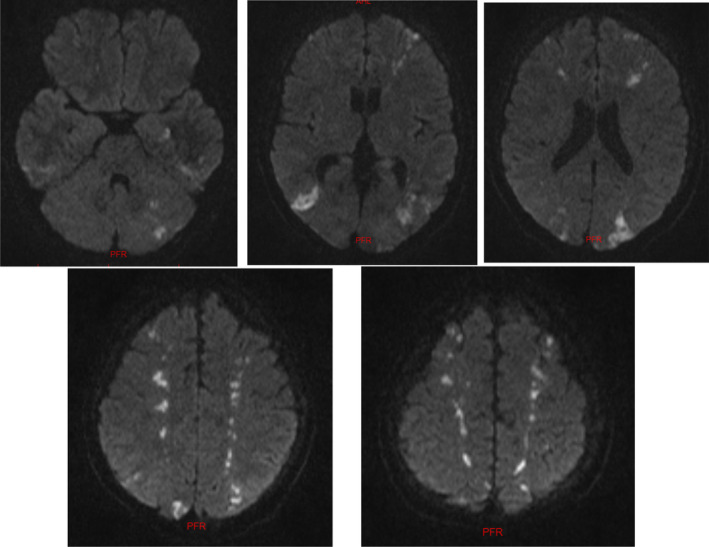 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRheumatoid Arthritis Research and Therapies · Acute Ischemic Stroke Management · Cardiac Imaging and Diagnostics
INTRODUCTION
1
Myocardial infarction (MI) remains the primary cause of mortality among both men and women in the United States, with stroke ranking as the third leading cause of death and the primary contributor to disability.1 Acute coronary syndrome and cerebrovascular accidents (CVA) constitute medical emergencies that necessitate simultaneous diagnosis and treatment.2 Among the myriad factors contributing to MI, individuals with rheumatoid arthritis (RA) face an elevated risk of cardiovascular disease (CVD). Recent studies consistently highlight an increased risk of MI in individuals with RA compared to the general population.3 In this context, we present a case involving a patient with RA who initially exhibited early‐onset fatigue and nonspecific chest pain, leading to an acute MI. During hospitalization, the patient developed neurological symptoms, subsequently diagnosed as a cerebral stroke following the MI. This case underscores the significance of promptly addressing heart attacks to protect the brain and identifying neurological impairments through unusual symptoms for effective patient management.
CASE HISTORY/EXAMINATION
2
We introduce a 40‐year‐old female patient with a history of RA who visited the hospital emergency department following a cold, presenting with nonspecific symptoms of weakness and malaise. In the patient's drug history, the only medication noted was the use of corticosteroids, considering the history of RA. Physical examination revealed tachycardia (rate:128 beats/min, regular rhythm) and hypotension (blood pressure 75/50 mmHg).
METHODS
3
Initial measures, including basic tests and an ECG, were conducted upon admission. During these investigations, sinus tachycardia and evidence of ST elevation were observed in leads V2‐4 and leads I and AVL on the patient's ECG, along with minimal reciprocal ST depression in leads III and AVF. The patient's cardiac troponin level was also measured at 172 ng/L. Liver function and other blood chemistries were normal. Diagnosed with an acute MI, the patient was admitted to the cardiac care unit, and according to the instructions from the cardiology service, the patient underwent appropriate medical management with proper doses of antiplatelets and statins, along with intravenous morphine. Additionally, they were considered a candidate for PCI (percutaneous coronary intervention) for reperfusion. In the early minutes of hospitalization, the patient developed neurological symptoms, manifesting as weakness in all four limbs, progressively worsening. Neurological consultation was promptly requested for the patient. Initially, the patient underwent a detailed neurological examination. In this examination, cranial nerves were intact. In bilateral plantar reflex examinations, an upward response was observed. Proximal motor strength in the lower limbs was three‐fifths, and in the upper limbs was two‐fifths. Given the upper motor neuron symptoms, The patient underwent emergency echocardiography, as well as brain and cervical CT scans. The patient's echocardiography reported an ejection fraction of 45% without LV thrombosis. For the cervical spine CT scan, considering the patient's history of RA, an assessment of the integrity of the C1 and C2 vertebrae was requested, which revealed no abnormalities. The brain CT scan revealed indistinct hypodensities in the parietal and occipital regions, suggestive of a stroke. Therefore, alongside continued treatment with antiplatelet and anticoagulant medications, as well as addressing the patient's hypotension through intravenous hydration, the patient underwent a brain MRI. (Figure 1).
Axial section of brain MRI utilizing the DWI sequence, illustrating an acute watershed infarct involving both territories of the anterior and posterior cerebral vascular supplies.
In the brain MRI, as depicted in Figure 1, evidence of watershed cerebral infarction was observed in most territories within the anterior and posterior cerebral vascular supply, including the ACA‐MCA and MCA‐PCA territories. This pattern of involvement indicates a decrease in blood supply to the brain. It appears that in this patient, following a MI, systemic blood pressure has dropped, affecting both anterior and posterior cerebral circulation systems, leading to the occurrence of watershed infarction. Additionally, a brain CT angiography was conducted to evaluate intracranial vessels, revealing no significant stenosis in the intracranial arteries. The patient underwent medical treatment as well as physiotherapy and occupational therapy during the hospitalization. The strength in all four limbs showed improvement. Further examinations for the patient included bilateral transcranial Doppler ultrasonography, with no pathological findings reported. After completing the course of treatment and neurological assessments, the patient was transferred to the cardiology department for additional cardiac investigations.
CONCLUSIONS AND RESULTS
4
To prevent the occurrence of watershed cerebral infarctions, it is advisable to avoid sudden drops in blood pressure as much as possible. Endovascular interventions are recommended in the presence of any symptomatic stenosis in extracranial vessels. Additionally, if any acute neurological symptoms arise from cardiac causes, a neurological examination is warranted.
DISCUSSION
5
Watershed infarctions are acute ischemic strokes that predominantly occur in regions of the brain known as border zones, between the two blood supply territories.4 Two hypotheses exist to determine the mechanism of watershed infarction, with one attributing it to decreased blood flow to brain tissue (hypoperfusion). Reports indicate instances of syncope preceding watershed infarctions, supporting the hypoperfusion hypothesis. Another theory considered for the mechanism of watershed infarction is the micro embolism infarct theory. It suggests that unstable atherosclerotic plaque in arterial walls leads to micro emboli formation, resulting in multiple infarcts in brain tissue. Imaging and pathological studies suggest that embolic infarctions predominantly affect distal cortical vessels.5 Accurate diagnosis of watershed infarction, like other infarctions, involves using MRI. Brain CT angiography (CTA) examines major intracranial vessels and small arteries. CTA enables a more in‐depth investigation of the causes of watershed infarction for therapeutic and preventive measures, including assessing risk factors for CVAs.6 RA, mentioned in our patient's medical history due to its inflammatory nature, predisposes individuals to a higher incidence of vascular diseases compared to the general population, such as MIs and vasculitis.3 A reduction in cerebral blood flow, for any reason, can disrupt the autoregulation system, leading to cerebral metabolic disturbances. Causes for this decrease in cerebral blood flow that can result in watershed infarction include syncope or other cardiac issues such as arrhythmias or MIs. In our studied patient, a drop in blood pressure and decreased cerebral blood flow following a MI set the stage for watershed infarction in both anterior and posterior cerebral vascular systems. Most patients with watershed infarctions have favorable outcomes. However, cases, where infarction occurs post‐cardiac surgery, have a higher probability of bilateral watershed infarction and often have poorer outcomes. It is reported that 8 out of 10 cases of mortality in watershed infarctions occur post‐cardiac surgery.7 Non‐surgical patients usually have unilateral infarctions, often accompanied by gradual arterial stenosis leading to collateral formation. In our study patient, despite experiencing both MI and bilateral watershed cerebral infarctions, there was a favorable prognosis, with improved muscle strength and other neurological symptoms during hospitalization.
AUTHOR CONTRIBUTIONS
Sajjad Daneshyar: Data curation; writing – original draft. Mojtaba Khazaei: Project administration. Mozhgan Nazifi: Writing – original draft.
FUNDING INFORMATION
None.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
ETHICAL APPROVAL
Patient's informed written consent was obtained.
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nascimento BR , Brant LCC , Marino BCA , Passaglia LG , Ribeiro ALP . Implementing myocardial infarction systems of care in low/middle‐income countries. Heart. 2019;105(1):20‐26.30269080 10.1136/heartjnl-2018-313398 · doi ↗ · pubmed ↗
- 2Mishra J , Kumar A , Kumar S , Singh S , Nayan SK , Dev A . Incidence of acute myocardial infarction in patients presenting with cerebrovascular accident in a tertiary care centre in Eastern India. Cureus. 2022;14(9):32‐41.10.7759/cureus.29005 PMC 955018236249661 · doi ↗ · pubmed ↗
- 3Johri N , Varshney S , Gandha S , et al. Association of cardiovascular risks in rheumatoid arthritis patients: management, treatment and future perspectives. HSR. 2023;8:100108.
- 4Torvik A . The pathogenesis of watershed infarcts in the brain. Stroke. 1984;15(2):221‐223.6701929 10.1161/01.str.15.2.221 · doi ↗ · pubmed ↗
- 5El Sadek A , Gaber A , Afifi H , Farag S , Salaheldien N . Microemboli versus hypoperfusion as an etiology of acute ischemic stroke in Egyptian patients with watershed zone infarction. Egypt J Neurol Psychiatr Neurosurg. 2019;55:1‐6.30679900 10.1186/s 41983-018-0045-8PMC 6321838 · doi ↗ · pubmed ↗
- 6Dong MX , Hu L , Huang YJ , Xu XM , Liu Y , Wei YD . Cerebrovascular risk factors for patients with cerebral watershed infarction: a case–control study based on computed tomography angiography in a population from Southwest China. Medicine. 2017;96(28):83‐94.10.1097/MD.0000000000007505 PMC 551577128700499 · doi ↗ · pubmed ↗
- 7Gottesman RF , Sherman PM , Grega MA , et al. Watershed strokes after cardiac surgery: diagnosis, etiology, and outcome. Stroke. 2006;37(9):2306‐2311.16857947 10.1161/01.STR.0000236024.68020.3a · doi ↗ · pubmed ↗