Colo-colonic intussusception secondary to Burkitt lymphoma with concurrent malignant small bowel mesh adhesion
Mei Jing Ho, Faisal Syed, Wieslawa Mary Wielebinski, Kamal Galketiya

TL;DR
A 28-year-old woman had a rare case of colo-colonic intussusception caused by Burkitt lymphoma and required surgery to remove affected bowel segments.
Contribution
This case report highlights a rare presentation of Burkitt lymphoma causing intussusception and concurrent mesh adhesion in the small bowel.
Findings
Colo-colonic intussusception was managed with an extended right hemicolectomy.
A segment of small bowel with malignant adhesion to a prosthetic mesh was resected.
The case emphasizes surgical considerations for adult intussusception.
Abstract
Intussusception is a rare presentation in adult population and usually occurs secondary to an underlying pathology. We report an unusual case of a 28-year-old female who developed a colo-colonic intussusception secondary to Burkitt lymphoma which was managed with an extended right hemicolectomy. The case was further complicated by a segment of small bowel with malignant adhesion to a prosthetic mesh requiring resection of the involved segment of small bowel. We have discussed the significance of this case as well as general considerations in the surgical management of adult intussusception.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
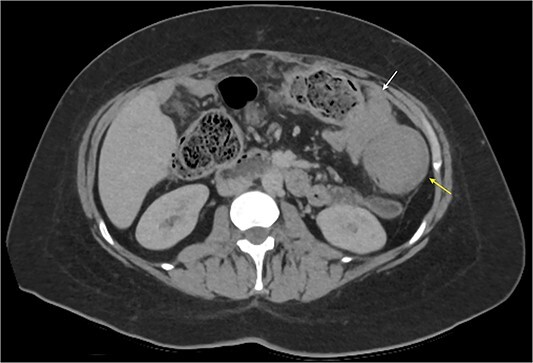 Figure 1
Figure 1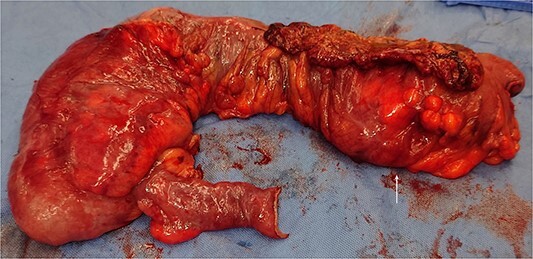 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment · Diverticular Disease and Complications
Introduction
Intussusception is a relatively rare condition which typically affects paediatric populations, with 90% of cases presenting by 2 years of age [1]. In adults, it is often secondary to a pathological lead point like malignancy [2, 3]. Extra-nodal type Burkitt lymphoma is a rapidly growing B-cell malignant neoplasm typically characterised by chromosome 8 translation involving the c-MYC oncogene, with common sites of extra-nodal manifestation including the ileum and caecum [1]. Whilst Burkitt lymphoma is the most common cause of intussusception of children over the age of 4, it is an uncommon cause of intussusception in adults [4].
Case report
A 28-year-old Caucasian female presented to a rural ED with right upper quadrant abdominal pain 5 days after a 13-week miscarriage and subsequent dilation, curettage and removal of retained products of conception. There was no report of obstructive symptoms with bowels opening that day and no history of nausea or vomiting. Her medical history was significant for asthma, migraines, reflux, anxiety and depression. In terms of surgical history, she had a laparoscopic appendicectomy 18 months prior to presentation. A week later, she presented with gallstone pancreatitis with a distal common bile duct stone identified on Magnetic retrograde cholangiopancreatography (MRCP). She underwent an Endoscopic retrograde cholangiopancreatography (ERCP) followed by an elective laparoscopic cholecystectomy a month later. Despite these procedures and a normal intra-operative cholangiogram, she had recurrent episodes of cholangitis requiring multiple ERCPs and biliary stenting for a benign CBD stricture with her last ERCP was 3 months prior to this presentation. Furthermore 5 months prior, she presented with a painful but reducible umbilical incisional hernia containing small bowel which was laparoscopically repaired with a 12 cm Symbotex mesh secured with suture and AbsorbaTacks.
On presentation, she was mildly tachycardic with a normal blood pressure. Blood results were all within normal limits. A computed tomography (CT) of her abdomen and pelvis revealed colo-colonic intussusception with a soft tissue mass in proximity to the splenic flexure (Fig. 1). A review of her last imaging performed 3 months ago showed no evidence of a colonic soft tissue mass in that location. She also had a colonoscopy 1 year ago for investigation of diarrhoea, which showed increased mucosal eosinophils of the terminal ileum and active chronic inflammation of the colon with eosinophilia.
Abdominal CT axial slice demonstrating colo-colonic intussusception at the splenic flexure and a colonic soft tissue mass just distal.
The patient was resuscitated with intravenous fluids and consented for an urgent laparotomy. Intra-operatively, a large polypoid colonic mass of the mid-transverse colon (Fig. 2) with associated lymphadenopathy were observed. Furthermore, a segment of the proximal ileum was densely adherent to the mesh from her previous incisional hernia. There were no liver lesions or evidence of obvious peritoneal disease. As such, an extended right hemicolectomy and anastomosis was performed. As the adherent small bowel was unable to be safely dissected off the mesh, a small bowel resection and anastomosis was also performed.
Clinical photo of the operative specimen with a large colonic mass (white arrow).
The patient made an uneventful recovery and was discharged home 5 days later. However, she re-presented 11 days later with right-sided abdominal pain, abdominal distension and vomiting. A repeat CT demonstrated thickened and dilated loops of small bowel and a collapsed colon, consistent with a high-grade small bowel obstruction with no evidence of anastomotic complications (Fig. 3). By this stage, her histopathology had returned with a diagnosis of high-grade Burkitt lymphoma extensively involving the large bowel, resection margins, 53 pericolic lymph nodes and omentum, as well as serosal involvement of the segment of resected small bowel. Histopathological staining indicated a Ki-67 proliferation index of almost 100% and diffuse positive staining for c-MYC.
Abdominal CT coronal slice demonstrating multiple loops of dilated fluid filled small bowel with significant wall thickening.
She was managed non-operatively with nasogastric decompression, bowel rest and intravenous hydration. The Haematology team was consulted and commenced her on steroids. As there was no improvement in her obstructive symptoms, thought to be secondary to her extensive lymphoma, she was urgently transferred to a major tertiary centre for ongoing treatment and commencement of chemotherapy.
Discussion
Intussusception occurs when a segment of bowel telescopes into an adjacent bowel segment. While it can occur at any age, it is most common in children. In contrast, it is a relatively rare clinical entity in adults, accounting for only 5% of cases and 1-5% of intestinal obstruction [5–9]. In paediatric populations, intussusception is typically idiopathic with a small number being secondary to a lead point such as a Meckel’s diverticulum, a benign or malignant lesion. This aetiology is reversed in adults, with majority of cases secondary to a pathological or neoplastic process [1, 5–8]. The exact mechanism on intussusception remains unknown. However, it is postulated that the presence of a bowel lesion changes the normal peristaltic activity, which serves as the lead point to trigger the invagination [5, 9]. Whilst there are some case reports of intussusception secondary to Burkitt lymphoma in paediatric and adult populations, it appears that colo-colonic intussusception is a less common phenomenon in both demographics [1, 8]. There is a case of ileocolic intussusception secondary to Burkitt lymphoma in a 17-year-old male with nodal involvement [10]. In addition, Sendra-Fernandez et. al described another case of Burkitt lymphoma with extranodal involvement [11]. Our current report adds to the paucity of literature primary colorectal lymphoma as a cause of adult intussusception.
The clinical presentation in adult intussusception is often chronic and non-specific in nature. Abdominal pain is the most common presenting complaint. Other symptoms include nausea, vomiting, altered bowel habits and haematochezia [5, 7, 9]. There are multiple imaging modalities used in the diagnosis of intussusception, namely, plain abdominal X-ray, abdominal ultrasound, barium studies and CT abdominal scans. Nevertheless, the diagnosis of intussusception is often made using abdominal CT imaging, given its diagnostic yield of approximately 58%–100% [9] and facilitates the identification of the underlying aetiology. The CT feature includes a ‘target sign’ which can usually be observed on the sagittal view [5, 7, 9].
In adults, the definitive approach to intussusception is surgery, especially once a malignant lesion has been identified as a potential lead point [5, 7, 8]. This usually involves an oncological resection and primary anastomosis of the involved segment of bowel. Whilst endoscopic reduction can be attempted if no such lesion has been identified, ultimately surgical resection may be required if there is any endoscopic or clinical evidence of perforation, enteric or colonic ischemia, non-resolving obstruction or a mucosal lesion [6]. Given the patient had an uneventful colonoscopy a year prior and that there was an obvious soft tissue colonic lesion on imaging, our patient was treated surgically with a resection and primary anastomosis of the involved segment of bowel.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yagmur Y , Gumus S. Burkitt's lymphoma causing intussusception in adults: report of two cases and review of the literature. J Gastroenterol Hepatol 2015;4:1689–702.
- 2Aydin N , Roth A, Misra S. Surgical versus conservative management of adult intussusception: case series and review. Int J Surg Case Rep 2016;20:142–610.1016/j.ijscr.2016.01.019.26859872 PMC 4818310 · doi ↗ · pubmed ↗
- 3Guner A , Karyagar S, Livaoglu A. et al. Small bowel intussusception due to metastasized Sarcomatoid carcinoma of the lung: a rare cause of intestinal obstruction in adults. Case Rep Surg 2012;2012:962683.23346451 10.1155/2012/962683 PMC 3546449 · doi ↗ · pubmed ↗
- 4Chung EM , Biko DM, Arzamendi AM. et al. Solid Tumors of the peritoneum, Omentum, and mesentery in children: radiologic-pathologic correlation:from the radiologic pathology archives. Radiographics 2015;35:521–46.25763737 10.1148/rg.352140273 · doi ↗ · pubmed ↗
- 5Aref H , Nawawi A, Altaf A. et al. Transient small bowel intussusception in an adult: case report with intraoperative video and literature review. BMC Surg 2015;15:3610.1186/s 12893-015-0020-6.25881028 PMC 4416349 · doi ↗ · pubmed ↗
- 6Marinis A , Yiallourou A, Samanides L. et al. Intussusception of the bowel in adults: a review. World J Gastroenterol 2009;15:407–1110.3748/wjg.15.407.19152443 PMC 2653360 · doi ↗ · pubmed ↗
- 7Salim J , Oliphant R, Krishnaswasmy M. et al. A twisted intussusception. ANZ J Surg 2019;89:E 458–9.30211476 10.1111/ans.14742 · doi ↗ · pubmed ↗
- 8Bernadi D , Asti E, Bonavina L. Adult ileocolic intussusception caused by Burkitt lymphoma. BMJ Case Rep 2016;2016:bcr 201621833410.1136/bcr-2016-218334.PMC 517489227920022 · doi ↗ · pubmed ↗