Cross‐cultural adaptation and measurement properties of the Persian version of the modified Cincinnati knee rating system
Nasim Eshraghi, Peyman Mirghaderi, Reza Omid, Mohamad Sajadi, Amirreza Pashapour‐Yeganeh, S. M. Javad Mortazavi

TL;DR
This study validates a Persian version of a knee rating system used to assess outcomes after ACL surgery.
Contribution
The Persian version of the MCRKS is shown to be reliable and valid for clinical use in Persian-speaking populations.
Findings
The Persian MCRKS has high internal consistency (Cronbach's α of 0.9).
It shows strong reliability with ICC values between 0.82 and 0.97.
The scale is sensitive and free from floor or ceiling effects.
Abstract
To validate and assess the cross‐sectional adaptation of the modified Cincinnati knee rating system (MCRKS) Persian translation. To assess test‐pretest reliability, 102 participants were asked to fill out the MCRKS (Per) scale after anterior cruciate ligament (ACL) reconstruction surgery. Internal consistency (Cronbach's α), reliability (intraclass correlation coefficients), construct validity (Pearson's r) and sensitivity (floor/ceiling effect) were determined. In addition, patients completed other relevant measures as the ACL return to sports after injury (ACL‐RSI) survey, hospital for special surgery ACL satisfaction survey (HSS ACL‐SS), visual analogue scale (VAS) of pain and patient's satisfaction, Tegner activity score (TAS), single assessment numeric evaluation, and Lysholm score. Using MCRKS (Per), the internal consistency (Cronbach's α) was 0.9 (if item deleted: 0.81–0.86);…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
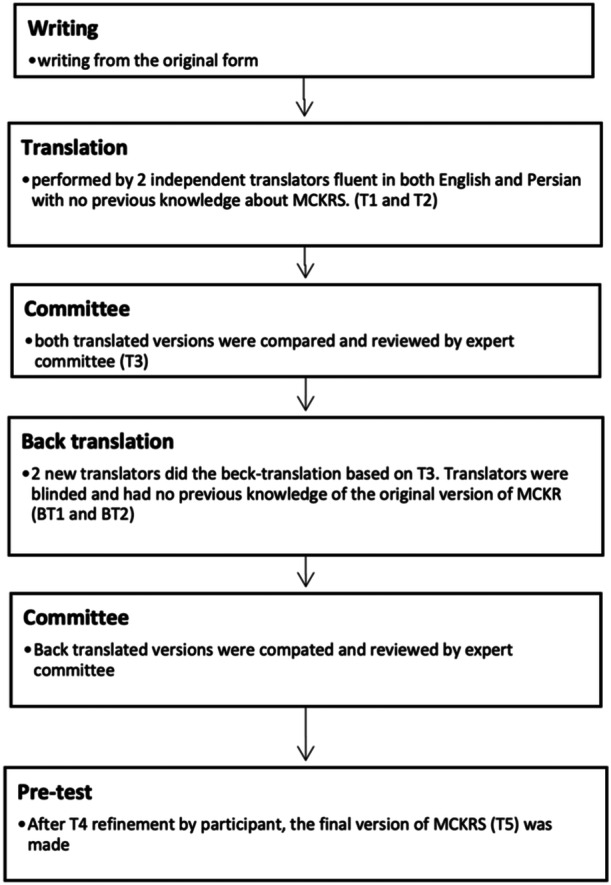 Figure 1
Figure 1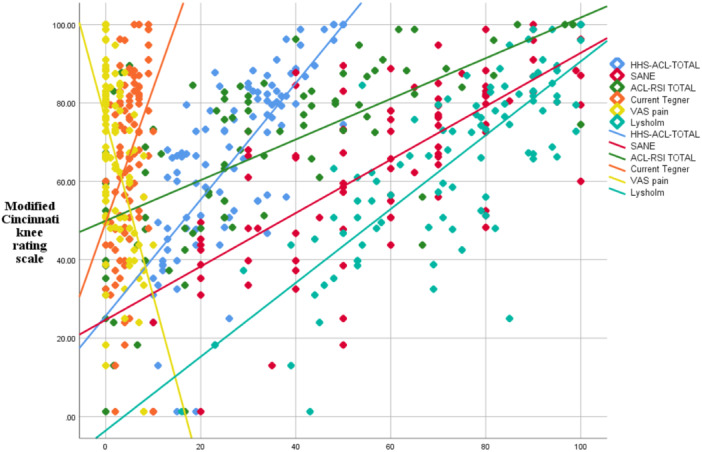 Figure 2
Figure 2| Variable ( | Mean ± SD or |
|---|---|
| Sex (male) | 90 (89.1) |
| BMI, kg/m2 | 22.8 ± 3.4 |
| Age, years | 29.1 ± 8.0 (range: 18–52) |
| Side | |
| Left | 39 (38.6) |
| Right | 62 (61.4) |
| Follow‐up (years) | 2.5 ± 1.2 (range: 1–6) |
| Mechanism | |
| Sport | 65 (64.4) |
| Contact | 16 (15.8) |
| Noncontact | 49 (48.5) |
| Accident | 20 (19.8) |
| Falling | 12 (11.9) |
| Chronic | 4 (4.0) |
| Sports before Injury | |
| Soccer | 54 (53.5) |
| Other | 17 (16.8) |
| None | 30 (29.7) |
| High‐risk sports for ACL tear (Football, basketball, lacrosse, rugby, and skiing) | |
| Yes | 56 (55.4) |
| No | 15 (14.9) |
| None | 30 (29.7) |
| Preinjury level of sport | |
| Competitive | 24 (23.8) |
| Recreational | 47 (46.5) |
| None | 30 (29.7) |
| Time from injury to surgery (months) | 21.9 ± 40.0 (range: 0.3–240) |
| Postoperative scores | |
| MCRKS | 65.9 ± 22.6 |
| Pain | 12.0 ± 5.8 |
| Swelling | 7.6 ± 3.3 |
| Giving away | 15.1 ± 6.1 |
| Overall activity level | 12.7 ± 5.0 |
| Walking | 7.6 ± 2.5 |
| Stairs | 3.6 ± 1.3 |
| Running activity | 5.1 ± 3.6 |
| Jumping | 2.4 ± 1.6 |
| ACL‐RSI | 30.7 ± 27.1 |
| Emotion | 30.4 ± 31.3 |
| Confidence in performance | 30.8 ± 28.6 |
| Risk appraisal | 31.5 ± 30.9 |
| Tegner | Median= 5 (range: 0–10) |
| Lysholm | 73.7 ± 19.3 |
| VAS pain | 2.2 ± 2.7 |
| SANE | 60.4 ± 24.2 |
| HSS ACL‐SS | 27.0 ± 11.3 |
| Item | Scale mean if item deleted | Scale variance if item deleted | Corrected item‐total correlation | Cronbach's |
|---|---|---|---|---|
| Pain | 53.9604 | 319.710 | 0.765 | 0.812 |
| Swelling | 58.3366 | 420.967 | 0.606 | 0.833 |
| Giving away | 50.8713 | 356.945 | 0.510 | 0.861 |
| Overall activity level | 53.2079 | 356.818 | 0.684 | 0.821 |
| Walking | 58.2723 | 433.321 | 0.710 | 0.830 |
| Stairs | 62.3688 | 465.409 | 0.780 | 0.843 |
| Running activity | 60.8713 | 394.757 | 0.722 | 0.819 |
| Jumping | 63.5569 | 457.486 | 0.760 | 0.839 |
| MCRKS subscales | Pain (rt) | Swelling (rt) | Giving away (rt) | Activity level (rt) | Walking (rt) | Stairs (rt) | Running activity (rt) | Jumping (rt) | Total score (rt) |
|---|---|---|---|---|---|---|---|---|---|
| Pain (t) | |||||||||
|
| 0.944 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
|
| <0.001 | ||||||||
| Swelling (t) | |||||||||
|
| ‐ | 0.829 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
|
| <0.001 | ||||||||
| Giving away (t) | |||||||||
|
| ‐ | ‐ | 0.962 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
|
| <0.001 | ||||||||
| Activity level (t) | |||||||||
|
| ‐ | ‐ | ‐ | 0.905 | ‐ | ‐ | ‐ | ‐ | ‐ |
|
| <0.001 | ||||||||
| Walking (t) | |||||||||
|
| ‐ | ‐ | ‐ | ‐ | 0.850 | ‐ | ‐ | ‐ | ‐ |
|
| <0.001 | ||||||||
| Stairs (t) | |||||||||
|
| ‐ | ‐ | ‐ | ‐ | ‐ | 0.927 | ‐ | ‐ | ‐ |
|
| <0.001 | ||||||||
| Running activity (t) | |||||||||
|
| ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | 0.938 | ‐ | ‐ |
|
| <0.001 | ||||||||
| Jumping | |||||||||
|
| ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | 0.872 | ‐ |
|
| <0.001 | ||||||||
| Total score (t) | |||||||||
|
| ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | 0.971 |
|
| <0.001 | ||||||||
| MCRKS subscales | Pain | Swelling | Giving away | Activity level | Walking | Stairs | Running activity | Jumping | Total score |
|---|---|---|---|---|---|---|---|---|---|
| Lysholm | |||||||||
|
| 0.720 | 0.551 | 0.502 | 0.519 | 0.631 | 0.703 | 0.639 | 0.615 | 0.794 |
|
| <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Tegner | |||||||||
|
| 0.290 | 0.142 | 0.123 | 0.392 | 0.400 | 0.208 | 0.476 | 0.436 | 0.421 |
|
| <0.003 | 0.156 | 0.220 | <0.001 | <0.001 | 0.037 | <0.001 | <0.001 | <0.001 |
| ACL‐RSI | |||||||||
|
| 0.567 | 0.377 | 0.433 | 0.455 | 0.426 | 0.513 | 0.563 | 0.562 | 0.642 |
|
| <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| SANE | |||||||||
|
| 0.680 | 0.492 | 0.322 | 0.643 | 0.569 | 0.654 | 0.573 | 0.602 | 0.721 |
|
| <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| HSS ACL‐SS | |||||||||
|
| 0.653 | 0.455 | 0.480 | 0.567 | 0.540 | 0.621 | 0.682 | 0.718 | 0.782 |
|
| <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| VAS pain | |||||||||
|
| −0.538 | −0.331 | −0.160 | −0.342 | −0.371 | −0.517 | −0.419 | −0.392 | −0.507 |
|
| <0.001 | 0.001 | 0.112 | 0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Study and reference | Language | Population | Test‐retest reliability (ICC) | Cronbach's | Validation scores | Correlation (Spearman's |
|---|---|---|---|---|---|---|
| Khaja 2020 MCRKS [ | Arabic | 57 | >0.70 | 0.792 | KOOS | 0.76 |
| Crespi 2020 CKRS [ | Italian | 124 | 0.85 | 0.76 | Lysholm | 0.75 |
| Ramos Marinho 2020 CKRS [ | Brazilian‐Portuguese | 150 | 0.96–0.99 | 0.54–0.79 | Lysholm | 0.19–0.82 |
| This study 2024 | Persian | 101 | 0.971 | 0.908 | Lysholm | 0.794 |
| Tegner | 0.421 | |||||
| HSS ACL‐SS | 0.782 | |||||
| ACL‐RSI | 0.642 | |||||
| VAS pain | −0.507 | |||||
| SANE | 0.721 |
- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Total Knee Arthroplasty Outcomes · Sports injuries and prevention
INTRODUCTION
The susceptibility to anterior cruciate ligament (ACL) ruptures is contingent upon a confluence of individual and environmental factors. Individual risk factors encompass the female gender [20], anatomical variations such as increased pelvic width, diminutive femoral dimensions, and heightened joint and ligamentous laxity, which collectively augment the strain exerted upon the knee joint [49]. Environmental risk factors include direct trauma to the lower extremity and participation in agility‐oriented sports necessitating rapid changes in direction, such as soccer, basketball, tennis, and lacrosse [20]. Despite the diligent endeavours of clinicians and researchers to mitigate the risk, the incidence of ACL injuries has increased twofold over the past two decades [25, 34]. Approximately 200,000–250,000 ACL injuries occur annually in the United States [35, 55], with minors under the age of 18 accounting for almost 25% of these injuries [2, 16]. For individuals who experience long‐term functional instability or recurrent instances of giving way, it is advisable to undergo anatomical ACL restoration [15].
Since its inception in 1983, the initial subjective Cincinnati knee rating system (CKRS) has been utilised extensively as a comprehensive knee assessment tool to identify ACL deficient knees [39, 40]. This scale is intended to detect clinical changes with the utmost sensitivity as it assesses the clinical condition of patients following surgical procedures [5, 44, 46]. Risberg et al., [43] examined the sensitivity of CKRS, IKDC, and Lysholm to variations over time in patients who had undergone ACLR surgery. During a two‐year follow‐up, the CKRS was the only sensitive instrument capable of identifying changes in clinical condition. Furthermore, CKRS is employed in research endeavors that assess the efficacy of various rehabilitation protocols and ACL surgery types [4, 8, 14, 21, 53, 54]. After undergoing revisions in 2000, MCRKS was founded in 1993. The patient is solely required to provide input on eight items comprising three subscales; these subscales assign an aggregate score of 6–100 (representing optimal function) and assess symptoms, function, and activities of daily living. To the best of our knowledge, the CKRS has been translated into Italian [12] and Brazilian‐Portuguese, and these translations have been confirmed to serve as a reliable foundation for comparing results across different investigations [42]. However, in the Italian version the authors cut down the original version by omitting some sections of the questionnaire [12].
Given the significant duration needed by both patients and professionals to fill out the paperwork, many writers utilise a modified version of the CKRS (MCRKS) to assess their patients and streamline data gathering [7, 31, 47]. This version refers to a widely used and not recommended short questionnaire consisting of eight items [1]. It has been proven to have a relationship with other validated surveys, such as the International Knee Documentation Committee (IKDC) subjective survey [5]. This version has only been validated and translated into Arabic [28].
The decision to culturally adapt and translate the MCRKS is driven by the need to introduce a concise Persian measurement tool for evaluating ACLR surgery and assessing its divergent and predictive validity in comparison to the original, lengthier version. This abbreviated version can be valuable in medical and rehabilitation settings with high patient volume. We anticipate that the MCRKS scale will exhibit favourable reliability, validity, and responsiveness when assessing the psychological preparedness for resuming sports activities in patients who have undergone ACL repair surgery.
MATERIALS AND METHODS
Study design
A cross‐sectional study was performed on adult patients who received ACLR surgery at our tertiary referral centre (Imam Khomeini Hospital, Tehran, Iran) from 2018 to 2022. In order to be eligible for this study, individuals must be above the age of 14 and have a confirmed diagnosis of a total or partial rupture of the ACL, regardless of the reason (whether it be sports‐related or not). The tear may or may not be accompanied by damage to the meniscus. Additionally, participants must have a scheduled surgery for ACL reconstruction (ACLR). All patients exhibited proficiency in all three linguistic modalities (writing, speaking, and reading) in the Persian language. Patients who were declined participation in the knee‐related test were excluded from the study. Furthermore, study participants were disqualified if they had articular cartilage repair, bilateral ACL injuries, or multiligament restoration. Prior to surgery, patients submitted written informed permission, which was authorised by our Institutional Review Board (IRB approval ID: IR.TUMS.MEDICINE.REC.1400.1462) in accordance with the Helsinki principles [19]. All patients were cognizant of the study's objective and provided verbal consent to participate in our research.
Translation and cross‐cultural adaptation
The translation process was performed by two independent translator (Amir Rakhshan and Alireza Moharrami) according to proposed guideline by Guillemin et al [22] and it is presented in (Figure 1). For pretest, we asked a random group of participants (n = 10) to answer the prepared version of questionnaire and explore each of them about the meaning and clarity of each item. Scoring was from 0—‘I understand nothing’; 1—‘I barely know what's the meaning’; 2—‘I understand the question’. With a Total score of 20, so study participants were able to answer the items properly. We recorded any suggestions participants had regarding the structural and functional format of the scale. T4 which was the final result of committee confirmation of back translation, was then adjusted and refined according to participants' responses. Therefore, the final version (T5) was provided and ready to use (Figure 1).
Cross‐cultural adaptation and translation of the modified Cincinnati knee rating system (MCRKS) flowchart.
Forward translation
Two English‐Persian translators were scheduled to adapt the condensed form of the original MCRKS for use in their respective cultures. Professional translators can take cultural differences into account. The initial translator (T1) possessed a profound understanding of medical terminology, exhibited extensive knowledge in orthopaedics, and comprehended the overarching objective of the study. T2 lacked medical training and possessed no comprehension of the subject matter being translated.
Consensus and revision
The original versions (T1 and T2) were reviewed and compared by a group consisting of three knee surgeons and two expert reviewers. According to the reviews, T2 is not much different from T1. The final version (T3) of MCRKS (Per) was a primary Persian version that was agreed upon by all parties.
Backward translation
Two blind translators (BT1 and BT2) worked to convert the Persian original into English. Two reverse‐translated versions (BT1 and BT2) proceeded to the next phase as a consequence.
Expert committee
The same committee meticulously assessed both the original scale and its forward and backward translated equivalents (T1, T2, BT1 and BT2). Improvements to the questionnaire were suggested and implanted. MCRKS (Per) T4, the final version, is the outcome.
Data analysis
The data analysis was conducted using the Statistical Package for Social Studies (SPSS 23; IBM Corp). Mean ± standard deviation (SD) was used to describe continuous variables, whereas frequency was used for categorical variables. The research was conducted using the outcomes of the questionnaires administered following ACLR surgery. An analysis was conducted on the measurement properties listed below:
Test‐retest reliability: It is defined as two administrations of questionnaire after two weeks when targeted concept is not changed. 102 patients were included in test‐retest measurement in order to demonstrate the consistency of the results. For test‐pretest reliability, we used intraclass correlation coefficient (ICC). A correlation coefficient value over 0.40 and 0.80 as satisfactory and excellent reliability respectively [3].
Construct validity : Spearman ρ coefficient was used to assess the correlation between Persian MCRKS subscales and in total and other instruments: VAS pain, Lysholm, Hospital for Special Surgery ACL satisfaction survey (HSS ACL‐SS), ACL‐RSI, SANE and TAS. We employed the second hypothesis: The correlation between correspond domains in MCKRS and HSS ACL‐SS or ACL‐RSI should be more significant than that of other domains. The correlation shows as strong (ρ≥0.5), medium (0.3≤ρ≤0.5) and weak (ρ<0.3) [11]
Ceiling and floor effect*:**
- content validity was evaluated via ceiling and floor effect; it's done to assess sensitivity of an instrument to detect different clinical outcomes and proportion of patient who had obtained the maximum and minimum scores. Researchers had endorsed that the effect size below 15% is fair enough to prove the content validity of a questionnaire [3].
Criterion validity: we adopted Lysholm and VAS pain scores as gold standards to calculate the correlation strength (by Spearman ρ coefficient) of our measure with them. We considered Spearman's ρ > 0.55 (confidence interval [CI] = 95%) as an adequate cut‐off [18, 48].
Patients and scores
In order to properly examine construct validity, reproducibility, ceiling and floor effects, and internal consistency, we needed a sample size of at least 100 patients, as suggested by Terwee et al. [36, 52]. A total of 102 patients aging 14–52 years enroled into the study (Table 1). Patients were asked to complete the validated Persian version of HSS ACL‐SS [33], Lysholm, Single Assessment Numeric evaluation [13], visual analogue scale (VAS), ACL‐RSI [17, 41], and Tegner activity scale (TAS). Negahban and others have cross‐culturally adapted the Persian version of the Tegner activity scale [38]. Informed consent was procured from all study participants. Furthermore, informed consent for the use of identifying information in an online open‐access publication was also obtained from all participants.
RESULTS
Patients' characteristics
A total of 102 patients with ACLR were included in the study. All of participants completed the study, therefore no data was excluded from the study. Only 55.4% (N = 56) patients were high risk [24, 37] for ACL tear. Study participants consist of professional athletes and members of the active population. The injury mechanism for 64.4% of patients (N = 65) was related to sports. Further Demographic data and clinical characteristics of the participants are presented in Table 1.
MCRKS (Per)
The subscales of MCRKS (Per) had an internal consistency (total Cronbach's α = 0.908) measuring Cronbach's α of each eight items with the highest impact on alpha coefficient if omitted for item‐3 ‘giving away’ (α = 0.896) and lowest for ‘pain’ (α = 0.812) (Table 2).
The test‐pretest intraclass correlation value (ICC) was 0.971 (p < 0.001) between total scores of test and retest phases. The most significant correlation was for swelling subscale (ICC = 0.829) (Table 3). All items' ICC was satisfactory and considered excellent (r≥0.81).
Content validity was evaluated through the floor and ceiling effects. Five (5.0%) had a 100 score (ceiling effect). However, no one got a 0 score (floor effect). Researchers had endorsed that the effect size below 15% is fair enough to prove the content validity of a questionnaire. Therefore, the MCRKS (Per) content validity was satisfactory.
The ACL‐RSI (r = 0.642), TAS (r = 0.421), SANE (r = 0.721), Lysholm (r = 0.794), HSS ACL‐SS (r = 0.782), and VAS pain ratings (r = –0.507) revealed significant correlations with the MCRKS score (all p < 0.001) (Figure 2).
Significant correlation between the Persian modified Cincinnati knee rating system (MCRKS) score and other relevant scales.
Regarding the construct validity, comparing the correlation coefficients of Lysholm, VAS, and MCRKS domains indicated that there remained a stronger association between the two quite similar parts rather than irrelevant ones. VAS pain and Lysholm pain scores were more significantly correlated to the MCRKS pain (question 1) (r = −0.538, r = 0.649, p < 0.001) than the other sections of MCRKS (r < 0.647) (Table 4). Also, for MCRKS swelling domain with Lysholm swelling domain (r = 0.785, p < 0.001), and MCRKS giving away domain with Lysholm instability domain (r = 0.719, p < 0.001) than other domains of MCKRS (r < 0.510). Due to these reasons, the MCRKS (Per) was considered a valid outcome measure concerning the construct validity.
DISCUSSION
This investigation demonstrates the favourable measurement features of MCRKS (Per) with no challenges in terms of comprehension and cultural adaptability. Furthermore, this measure demonstrated both reliability and validity in assessing the clinical result and satisfaction of patients who had received ACL reconstruction surgery. As far as we know, the Arabic MCRKS is the sole scale that has been translated and modified across different cultures [29]. The findings of this study can be used as a foundation for future verifications and adaptations of MCRKS. The test‐retest reliability of the ‘swelling’ subscale ranged from an ICC of 0.82 to an ICC of 0.96 for the ‘giving away’ subscale. Nevertheless, the interclass correlations were found to be lower in the Italian version (0.76–0.91) and greater in the Brazilian–Portuguese version of MCKRS (0.96–0.99) [12, 42]. Furthermore, our scale demonstrated exceptional internal consistency, as evidenced by a Cronbach's α coefficient of 0.908. This is notably higher than the α values of 0.76 and 0.78 observed in the Italian and Brazilian CKRS, respectively. The construct validity, as measured by Pearson's correlation coefficient (r), ranged from 0.55 to 0.72 for the Lysholm score in the Brazilian CKRS. This correlation was found to be poor, ranging from 0.19 to 0.82. However, it was statistically significant for both the Brazilian and Italian versions (Table 5).
Each patient‐reported outcome measurement (PRO) has a unique pattern of coverage across many domains (such as pain, symptoms, functional activities, occupational activities, sport/recreation, and quality of life) when assessing knee‐specific ACL injuries. The HSS ACL‐SS comprises 10 items that assess the level of patient satisfaction following ACLR. Patients assign numerical values to each question, resulting in a minimum score of 10 out of 50 and a maximum score of 50 out of 50. The MCKRS scale comprises multiple items that are categorised into five categories, each with its own distinct scoring system. Superior ratings indicate improved clinical circumstances following ACL surgery [26]. The Lysholm and Tegner activity measures were originally developed to assess cruciate ligament injuries, particularly those involving the ACL [9, 30, 51]. These scales have extensive usage in evaluating knee function and activity levels after surgery [10, 23]. The Lysholm score is employed to assess the efficacy of the knee joint in different activities, including work, sports, and leisure. Furthermore, this scale functions as an additional instrument to the knee functional rating system, with a scoring range of 0–100 [51]. The Lysholm scale demonstrates a strong association with other scales that specifically assess the knee. On the other hand, the MCRKS has been proven to be a valid, reliable, and responsive tool for evaluating knee function and symptoms in patients who have suffered an ACL injury and undergone reconstruction [32]. The Tegner activity scale consists of a numerical scale ranging from 0 to 10. A score of 0 indicates persons who are unable to work or need disability benefits because of knee‐related problems, while a score of 10 represents individuals who participate in competitive sports at a relatively high level [50]. The Single Numeric Assessment [13] is a subjective rating system used to evaluate patients' results. It involves asking patients to rank their wounded body part on a scale ranging from 0 to 100 [56]. Consequently, patients may not be required to respond to several inquiries. Furthermore, there are reports indicating a strong correlation between the SANE score and knee assessment measures such as the IKDC score and the knee outcome survey (KOS) [45]. The visual analogue scale (VAS) is a reliable and highly reproducible subjective measure used to assess a patient's pain level on a scale of 0–10 [6, 27]. However, total score of our Persian version of mKCRS showed significant moderate correlation with other PROs. but, two subscales presented weak correlations with the Tegner activity score, for items ‘swelling’ (r = 0.14) and the ‘giving away’ (r = 0.12). Selbourne et al. [45] reported moderate strong correlation between SANE and MCRKS (r = 0.66) which was quite similar with our findings (r = 0.71). With regards to floor and ceiling effect, no relevant effect was present as in Arabic version of MCRKS.
This study should encourage rehabilitators worldwide to validate the test in their own cultural context so that it can become a reference measure in assessing clinical conditions of patients after ACLR surgery.
LIMITATIONS
Our study is subject to several limitations. Initially, we did not assess the structural validity of the MCRKS (Per) instrument. Structural validity examines the dimensionality of the instrument and ensures that the subscales or domains within the instrument are distinct and measure different constructs. As per the COSMIN guidelines, structural validity is an important psychometric property that should be evaluated, especially in the early stages of validation studies. Future research should include a comprehensive assessment of structural validity, such as factor analysis or structural equation modelling, to confirm the hypothesised factor structure and dimensionality of the MCRKS (Per). Second, participants completed the questionnaire just once, hence this study does not provide any information regarding the responsiveness of MCRKS (Per). Third, we did not include patients with recurrent ACL injury or patients with ACL defect. It is advisable to utilise this scale for the evaluation of various types of ACL injuries beyond its original intended use. fourth, our study did not include any control group, so we were not able to show discriminant validity of our scale.
CONCLUSION
The present study gives evidence about the reliability and validity of MCRKS (Per) for health professionals and researchers. The MCRKS can be considered suitable for the use in the Iranian population for the assessment and monitoring of ACL reconstruction recovery.
AUTHOR CONTRIBUTIONS
Peyman Mirghaderi and Nasim Eshraghi contributed to the study conception and design, analysed data and edited the manuscript. Reza Omid contributed to the study design and wrote the first draft of the manuscript. Mohamad Sajadi and Amirreza Pashapour‐Yeganeh contributed to the study design, data collection and drew figures. S. M. Javad Mortazavi supervised the project, validate data and revised the manuscript. All authors commented on previous versions of the manuscript and revised it. All authors read and approved the final manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
ETHICS STATEMENT
The study was reviewed and approved by the Institutional Review Board of Tehran University of Medical Sciences. An informed consent signed by all the participants of study. Patient consent was obtained regarding publication of data and photographs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agel, J. & La Prade, R.F. (2009) Assessment of differences between the modified Cincinnati and International Knee Documentation Committee patient outcome scores: a prospective study. The American Journal of Sports Medicine, 37, 2151–2157. Available from: 10.1177/0363546509337698 19633231 · doi ↗ · pubmed ↗
- 2Ardern, C.L. , Ekås, G. , Grindem, H. , Moksnes, H. , Anderson, A. , Chotel, F. et al. (2018) 2018 International Olympic Committee consensus statement on prevention, diagnosis and management of paediatric anterior cruciate ligament (ACL) injuries. Knee Surgery, Sports Traumatology, Arthroscopy, 26, 989–1010. Available from: 10.1007/s 00167-018-4865-y PMC 587625929455243 · doi ↗ · pubmed ↗
- 3Atkinson, G. & Nevill, A.M. (1998) Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Medicine, 26, 217–238. Available from: 10.2165/00007256-199826040-00002 9820922 · doi ↗ · pubmed ↗
- 4Bankaoğlu, M. , Yapıcı Uğurlar, Ö. , Uğurlar, M. , Günaydın, B. , Ertürk, Ş.M. & Eren, O.T. (2021) Prediction of clinical outcomes of single‐ and double‐bundle anterior cruciate ligament reconstruction techniques using magnetic resonance imaging. Ulusal travma ve acil cerrahi dergisi = Turkish Journal of Trauma & Emergency Surgery, 27, 565–570. Available from: 10.14744/tjtes.2020.06565 34476783 · doi ↗ · pubmed ↗
- 5Barber‐Westin, S.D. , Noyes, F.R. & Mc Closkey, J.W. (1999) Rigorous statistical reliability, validity, and responsiveness testing of the Cincinnati knee rating system in 350 subjects with uninjured, injured, or anterior cruciate ligament‐reconstructed knees. The American Journal of Sports Medicine, 27, 402–416. Available from: 10.1177/03635465990270040201 10424208 · doi ↗ · pubmed ↗
- 6Beischer, S. , Gustavsson, L. , Senorski, E.H. , Karlsson, J. , Thomeé, C. , Samuelsson, K. et al. (2020) Young athletes who return to sport before 9 months after anterior cruciate ligament reconstruction have a rate of new injury 7 times that of those who delay return. Journal of Orthopaedic & Sports Physical Therapy, 50, 83–90. Available from: 10.2519/jospt.2020.9071 32005095 · doi ↗ · pubmed ↗
- 7Borsa, P.A. , Lephart, S.M. & Irrgang, J.J. (1998) Sport‐specificity of knee scoring systems to assess disability in anterior cruciate ligament‐deficient athletes. Journal of Sport Rehabilitation, 7, 44–60. Available from: 10.1123/jsr.7.1.44 · doi ↗
- 8Bozduman, Ö. , Gürün, E. & Cahit Çıtır, Ö. (2023) The effect of brace use on clinical outcomes after arthroscopic meniscus repair. European Review for Medical and Pharmacological Sciences, 27, 1863–1868. Available from: 10.26355/eurrev_202303_31550 36930482 · doi ↗ · pubmed ↗