Germline BRCA1 ‐Mutated Synchronous and Metachronous Pancreatic Acinar Cell Carcinoma With Long‐Term Survival
Tomohiro Kubo, Yuki Ikeda, Joji Muramatu, Kazuma Ishikawa, Makoto Yoshida, Kazuharu Kukita, Masafumi Imamura, Shintaro Sugita, Akihiro Sakurai, Kohichi Takada

TL;DR
A rare case of pancreatic cancer linked to a BRCA1 mutation is reported, highlighting the need for genetic testing in similar cases.
Contribution
First reported case of germline BRCA1-mutated synchronous and metachronous pancreatic acinar cell carcinoma.
Findings
A patient with BRCA1-mutated pancreatic cancer had synchronous and metachronous tumors.
Genetic testing led to cascade testing in family members, identifying the same BRCA1 mutation.
Treatment with olaparib failed after 4 months, but overall survival was prolonged.
Abstract
Pancreatic acinar cell carcinoma (PACC) is a rare pancreatic neoplasm. Recently, molecular analysis revealed that PACC shows a high frequency of the BRCA1/2 mutation and is likely to be considered a cancer associated with hereditary breast and ovarian cancer (HBOC). Hereditary cancers, including HBOC, are characterized by multifocal and/or metachronous tumors. However, no case reports exist of germline BRCA1‐mutated synchronous and metachronous PACC. A 58‐year‐old man was diagnosed with synchronous and metachronous PACC at the age of 56 and underwent two surgeries. Ten months after the second surgery, the patient developed multiple liver metastases. Gemcitabine plus nab‐paclitaxel therapy was administered as first‐line chemotherapy. After seven cycles, computed tomography examination revealed progressive disease (PD). Therefore, modified FOLFIRINOX (mFFX) was administered as second‐…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
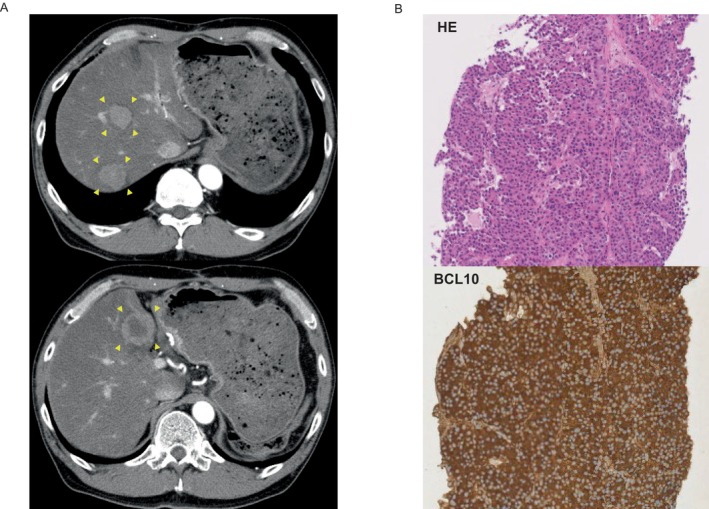 FIGURE 1
FIGURE 1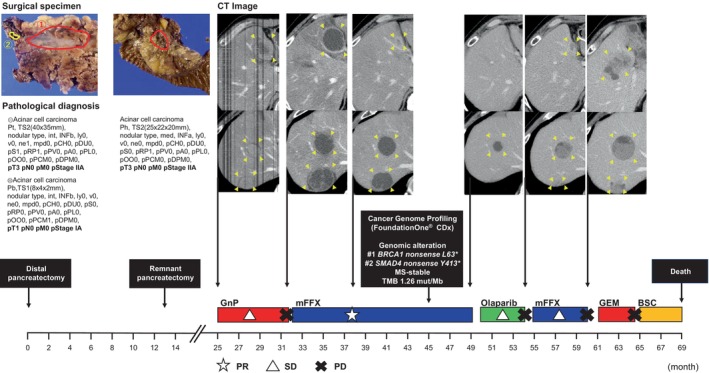 FIGURE 2
FIGURE 2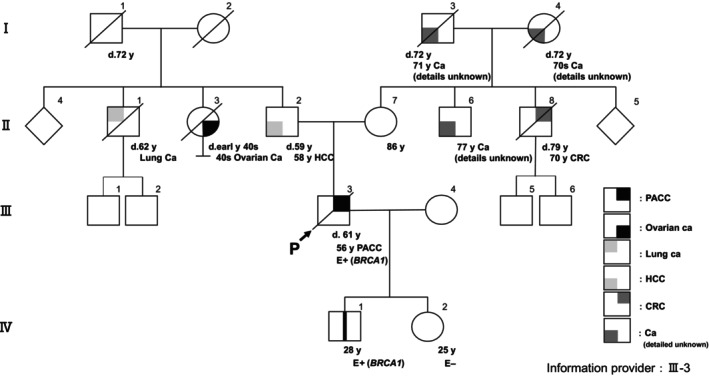 FIGURE 3
FIGURE 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Cancer Genomics and Diagnostics · Genetic factors in colorectal cancer
Introduction
1
Pancreatic acinar cell carcinoma (PACC) accounts for approximately 1% of pancreatic neoplasms and is considered a relatively rare tumor [1]. Several differences exist, in terms of biological behaviors and gene signatures, between PACC and pancreatic ductal adenocarcinoma (PDAC). Recent reports have shown that PACC has a distinctive mutational landscape [2, 3, 4, 5]. PACC exhibits a higher frequency of BRCA1/2 mutations compared to PDAC and is more likely to be an associated cancer of hereditary breast and ovarian cancer syndrome (HBOC). Hereditary cancers, including HBOC, are characterized by multifocal and/or metachronous tumors. Although PACC should be considered as part of the spectrum of BRCA1/2‐related malignancies, reports do not exist of BRCA‐mutated synchronous and metachronous PACC. We previously reported on this case as being the first instance of PACC that was found to be both synchronous and metachronous [6]. Subsequent genetic testing revealed the presence of a germline BRCA1 mutation, proving that this was an HBOC‐associated PACC. Herein, we highlight this PACC case as it suggests that aggressive genetic testing is required for this type of pancreatic cancer.
Case
2
A 58‐year‐old man was previously diagnosed with PACC of the pancreatic tail at the age of 56 and underwent a distal pancreatectomy; two masses were identified in the caudal and body of the pancreas at Sapporo Medical University Hospital (Sapporo, Japan) in March 2017. Ten months after surgery, a residual recurrence was found in the pancreatic head. The patient subsequently underwent a total resection of the residual pancreas at the same hospital in April 2018. We have previously reported details of the clinical course of the cancer [6]. Ten months after the second surgery, an abdominal computed tomography (CT) scan revealed three hypervascular masses in the liver. The hepatic tumor was diagnosed as a metastatic PACC based on the pathological analysis of a targeted hepatic tumor biopsy (Figure 1). Gemcitabine plus nab‐paclitaxel (GnP) therapy (gemcitabine, 1000 mg/m^2^ days 1, 8, 15; nab‐paclitaxel, 125 mg/m^2^ days 1, 8, 15; every 4 weeks) was administered as first‐line chemotherapy. After seven cycles, CT examination revealed the tumor had changed into a hypovascular tumor but its size had increased. We judged this to be PD. A modified combination regimen of 5‐fluorouracil, leucovorin, oxaliplatin, and irinotecan (modified FOLFIRINOX [mFFX]) therapy [5‐fluorouracil, 2400 mg/m^2^ days 1 and 2; leucovorin, 200 mg/m^2^ day 1; oxaliplatin, 85 mg/m^2^ day 1; irinotecan, 150 mg/m^2^ day 1; every 2 weeks] was administered as second‐line chemotherapy. The best response was a partial response, resulting in a 78% reduction. After 19 cycles of mFFX, comprehensive cancer genomic profiling (CGP; FoundationOne CDx) was performed on the second set of surgical specimens in order to explore effective therapeutic options according to gene alterations. Pathogenic variants were found in BRCA1 (c.188T>A, L63*, allele frequencies: 60.64%) and SMAD4 (c.1239C>A, Y413*, allele frequencies: 16.01%). The patient showed a family history of HBOC‐related cancers: For example, his paternal aunt died in her 40s due to ovarian cancer. The same BRCA1 pathogenic variant was detected in the germline of the patient by a single‐site sequencing; as a result, he was diagnosed with HBOC. After Japanese public health insurance covered treatment with olaparib, the patient was switched to this at a dose of 600 mg/day. After 4 months of treatment, the patient was judged to have PD. He was then treated with a reduced dose of mFFX (5‐fluorouracil, 1800 mg/m^2^ days 1 and 2; leucovorin, 200 mg/m^2^ day 1; oxaliplatin, 65 mg/m^2^ day 1; irinotecan, 120 mg/m^2^ day 1; every 2 weeks), but the patient was judged to have PD after 5 months. Subsequently, he was treated with gemcitabine monotherapy (gemcitabine, 1000 mg/m^2^ days 1, 8, 15 every 4 weeks); a response was not observed. The patient died 5 years and 9 months after his initial surgery, and 3 years and 8 months after the initiation of chemotherapy (Figure 2). His family members received genetic counseling and subsequent cascade genetic testing. The son and daughter underwent single‐site sequencing and the same gBRCA1 pathogenic variant was detected in the patient's son, prompting the initiation of cancer surveillance thereafter (Figure 3).
Contrast‐enhanced abdominal computed tomography and pathological findings of liver metastases. (A) Contrast‐enhanced abdominal computed tomography (CT) revealed three hypervascular masses (yellow arrowheads). (B) A percutaneous liver biopsy specimen was positive for BCL10, revealing the presence of PACC. BCL10, B‐cell lymphoma/leukemia 10; CT, computed tomography; HE, Hematoxylin eosin; PACC, pancreatic acinar cell carcinoma.
Clinical course after initial diagnosis. BSC, best supportive care; CT, computed tomography; FFX, fluorouracil, irinotecan, and oxaliplatin; mFFX, modified FFX; GEM, gemcitabine; GnP, gemcitabine and nab‐paclitaxel; MS, microsatellite status; PD, progressive disease; PR, partial response; SD, stable disease; TMB, tumor mutational burden.
The patient's family trees showing cases with germline BRCA1 variants. Ca, cancer; CRC, colorectal cancer; d, death; E, evaluation; HCC, hepatocellular carcinoma; P, proband; PACC, pancreatic acinar cell carcinoma.
Discussion
3
PACC has genetic features that are distinct from PDAC. In one study, up to 45% of PACC cases had a deficiency of DNA damage repair pathway genes such as BRCA1/2 [2]. Pathogenic variants in gBRCA1/2 are implicated in HBOC, which predisposes individuals to cancers such as those of the breast, ovary, pancreas, and prostate. The cumulative risk for developing pancreatic cancer by 70 years of the age is between 1% and 4% for carriers of gBRCA1/2 pathogenic variants [7]. Pathogenic variants in DNA damage repair gene mutations, such as ATM, PALB2, and CHEK2, have also been shown to be associated with HBOC [8, 9, 10]. Thus, PACC should be considered as part of the spectrum of HBOC‐related malignancies with the potential for being both synchronous and metachronous cancers. However, no prior reports exist of synchronous and metachronous BRCA1/2‐mutated PACC. To our knowledge, this case is the first such report.
The prognosis of postoperative recurrence or unresectable PACC remains poor, similar to that of PDAC [11]. Accumulated evidence has shown that *BRCA‐*mutated tumor cells are sensitive to platinum analog chemotherapeutics and poly ADP ribose polymerase (PARP) inhibitors [12]. Specifically, the efficacies of platinum‐based chemotherapy and PARP inhibitors for BRCA‐mutated pancreatic cancer, including PACC, have already been reported [13, 14]. In fact, the total duration of response in our case was approximately 14 months with platinum‐based chemotherapy and PARP inhibitors, resulting in long‐term survival. In addition to BRCA1/2 mutations, PACC has also been reported to have other druggable gene mutations, such as PALB2, ATM, BRAF, and JAK1 [15]. Currently, few reports exist on the efficacy of genotype‐matched therapy for PALB2, ATM, BRAF, and JAK1 mutations, with the exception of BRCA in PACC, with only case reports having achieved a CR with BRAF and MEK inhibitors for BRAF V600E [16]. Although the efficacy of genotype‐matched therapy for PACC has to first be established in clinical trials, such treatments may be good candidates for a personalized approach to therapy based on the gene mutations in PACC.
Genetic counseling to assess a patient's genetic predisposition and to plan for future healthcare may be not beneficial for those with unresectable pancreatic cancer and a poor‐prognosis. However, surveillance, risk‐reducing surgery, and oncologic treatment for gBRCA1/2 carriers have been reported to be useful in health care [17, 18, 19]. Like this case, assessing the genetic predisposition of a patient's family members based on the results of the patient's gBRCA1/2 pathogenic variant is useful in guiding the surveillance of potential carriers.
In conclusion, we diagnosed a 58‐year‐old man with a synchronous and metachronous PACC that was subsequently found to have a gBRCA1 pathogenic variant. Considering PACC is likely to be positive for BRCA1/2 mutations responsible for HBOC, resectable cases should be closely followed up with the prospect that the PACC may be synchronous or metachronous cancer. In both resectable and unresectable cases, genetic tests should be performed to assist in healthcare, including cancer surveillance, for blood relatives. Furthermore, in unresectable cases, genetic tests may lead to assisting in the selection of chemotherapeutic regimens and may contribute to a prolonged prognosis.
Author Contributions
Tomohiro Kubo: conceptualization, investigation, writing – original draft, resources, visualization. Yuki Ikeda: investigation, resources. Joji Muramatu: resources. Kazuma Ishikawa: resources. Makoto Yoshida: resources. Kazuharu Kukita: resources. Masafumi Imamura: resources. Shintaro Sugita: resources. Akihiro Sakurai: writing – review and editing. Kohichi Takada: writing – review and editing, conceptualization, supervision.
Ethics Statement
The authors have obtained informed consent from the individual involved prior to this study.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. Matsuno , S. Egawa , S. Fukuyama , et al., “Pancreatic Cancer Registry in Japan: 20 Years of Experience,” Pancreas 28, no. 3 (2004): 219–230.15084961 10.1097/00006676-200404000-00002 · doi ↗ · pubmed ↗
- 2J. Chmielecki , K. E. Hutchinson , G. M. Frampton , et al., “Comprehensive Genomic Profiling of Pancreatic Acinar Cell Carcinomas Identifies Recurrent RAF Fusions and Frequent Inactivation of DNA Repair Genes,” Cancer Discovery 4, no. 12 (2014): 1398–1405.25266736 10.1158/2159-8290.CD-14-0617 · doi ↗ · pubmed ↗
- 3N. Waddell , M. Pajic , A. M. Patch , et al., “Whole Genomes Redefine the Mutational Landscape of Pancreatic Cancer,” Nature 518, no. 7540 (2015): 495–501.25719666 10.1038/nature 14169 PMC 4523082 · doi ↗ · pubmed ↗
- 4E. D. Thompson and L. D. Wood , “Pancreatic Neoplasms With Acinar Differentiation: A Review of Pathologic and Molecular Features,” Archives of Pathology & Laboratory Medicine 144, no. 7 (2020): 808–815.31869246 10.5858/arpa.2019-0472-RA · doi ↗ · pubmed ↗
- 5D. Mandelker , A. Marra , B. Zheng‐Lin , et al., “Genomic Profiling Reveals Germline Predisposition and Homologous Recombination Deficiency in Pancreatic Acinar Cell Carcinoma,” Journal of Clinical Oncology 41, no. 33 (2023): 5151–5162.37607324 10.1200/JCO.23.00561 PMC 10667000 · doi ↗ · pubmed ↗
- 6Y. Ikeda , M. Yoshida , K. Ishikawa , et al., “Rare Case of Acinar Cell Carcinoma With Multiple Lesions in the Pancreas,” JGH Open 4, no. 6 (2020): 1242–1243.33319067 10.1002/jgh 3.12380 PMC 7731799 · doi ↗ · pubmed ↗
- 7M. A. Tempero , M. P. Malafa , M. Al‐Hawary , et al., “Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology,” Journal of the National Comprehensive Cancer Network 19, no. 4 (2021): 439–457.33845462 10.6004/jnccn.2021.0017 · doi ↗ · pubmed ↗
- 8A. Renwick , D. Thompson , S. Seal , et al., “ATM Mutations That Cause Ataxia‐Telangiectasia Are Breast Cancer Susceptibility Alleles,” Nature Genetics 38, no. 8 (2006): 873–875.16832357 10.1038/ng 1837 · doi ↗ · pubmed ↗