Clinical Characteristics and Prognosis of ICU-Admitted Patients with Guillain-Barre Syndrome: A Report from a Large Teaching Hospital in South Iran
Vida Naderi-boldaji, Farid Zand, Naeimehossadat Asmarian, Hoda Marbooti, Mansoor Masjedi, Seyedeh Maryam Tabibzadeh, Zahra Esmaeilinezhad, Masoume Nazeri

TL;DR
This study examines the clinical features and outcomes of ICU patients with Guillain-Barre Syndrome in Iran, finding that axonal type GBS requires more ventilation and has higher complication rates.
Contribution
The study provides new insights into the clinical characteristics and prognosis of GBS in a South Iranian population.
Findings
Axonal GBS was more common and required more frequent and prolonged mechanical ventilation compared to demyelinating GBS.
Pneumonia and sepsis were each observed in 16% of patients, with a 3.8% mortality rate.
Acute inflammatory demyelinating polyneuropathy was the most common GBS subtype.
Abstract
Guillain-Barre Syndrome (GBS) is the most prevalent acute peripheral polyneuropathy disorder. The disparities between populations and variations in the major risk factors highlight the importance of country-specific studies. This study aimed to report clinical characteristics and outcomes of ICU-admitted patients with GBS in an academic medical center in Iran. The data were collected retrospectively from all patients with GBS admitted to Namazi Hospital, affiliated with Shiraz University of Medical Sciences, (Shiraz, Iran), between March 2016 to March 2021. Specialized neurological information and the Acute Physiology and Chronic Health Evaluation (APACHE II) score were recorded. The SPSS software was used to analyze the data. The analyzed data were reported as numbers and percentages, or mean±SD, or median(Interquartile) The study included 132 GBS patients, with an average age of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
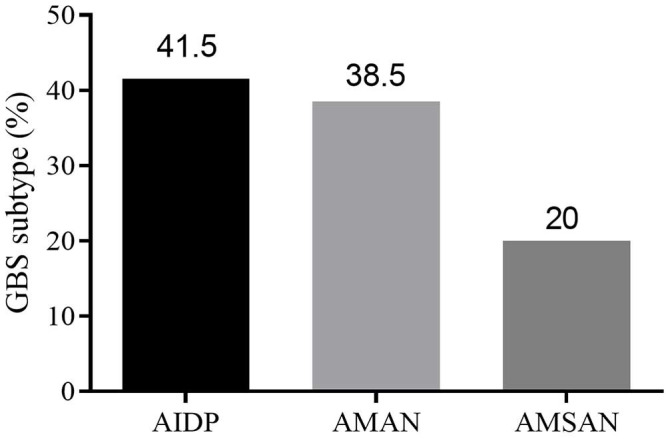 Figure 1
Figure 1| Characteristic | n (%) | |
|---|---|---|
| N=132 | ||
| Age (years) | Mean age (mean±SD) | 47.87±15.41 |
| Age≥60 years n (%) | 35 (26.3) | |
| Sex n (%) | Male | 83 (62.6) |
| Female | 49 (37.4) | |
| APACHE score, median(Q1-Q3) | 10 (6-14.25) | |
| Comorbidities | Malignancy | 0 (0) |
| Diabetes | 16 (12) | |
| Renal failure | 11 (8.2) | |
| Liver disease | 0 (0) | |
| Cardiovascular disease | 9 (6.8) | |
| Respiratory diseases | 54 (4.1) | |
| Previous infection | 80 (60.9) | |
| Grading of muscle strength | Upper extremity | |
| Grade 5 | 15 (11.2) | |
| Grade 4 | 56 (42.4) | |
| Grade 3 | 16 (12) | |
| Grade 2 | 25 (19.2) | |
| Grade 1 | 14 (10.4) | |
| Complete paralysis (Grade 0) | 6 (4.8) | |
| Lower extremity | ||
| Grade 5 | 7 (5.6) | |
| Grade 4 | 23 (17.6) | |
| Grade 3 | 34 (25.6) | |
| Grade 2 | 44 (33.6) | |
| Grade 1 | 14 (10.4) | |
| Grade 0 | 10 (7.2) | |
| Immunomodulatory treatment | Plasmapheresis (PLEX) | 38 (28.7) |
| Intravenous immunoglobulin (IVIg) | 73 (55) | |
| PLEX+IVIg | 16 (12.4) | |
| No treatment | 3 (2.3) | |
| Electrophysiological classification | Demyelinating | 55 (41.5) |
| Axonal | 77 (58.5) | |
| Mechanical ventilation | 55 (41.7) | |
| Duration, median (IQR) | 21.5 (9-38) | |
| <14 days | 40 (73) | |
| ≥14 days | 15 (27) | |
| Complications | n (%) |
|---|---|
| Pneumonia | 16 (12.3) |
| Sepsis | 16 (12.3) |
| Urinary infection | 12 (9.2) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Long-Term Effects of COVID-19
What’s Known
- Understanding the morbidity, mortality, and clinical characteristics of ICU-admitted Guillain-Barre syndrome patients is critical in recognizing correctable causes, modifying prognosis, and optimizing medical care. Epidemiologic reports have been presented from all over the world.
What’s New
- This study is the first to present the clinical characteristics of Guillain-Barre patients hospitalized in Namazi Hospital. The in-hospital mortality rate was 3.8%, and acute inflammatory demyelinating polyneuropathy (AIDP) was the most prevalent variant of Guillain-Barre syndrome.
Introduction
Guillain-Barre Syndrome (GBS) is the most prevalent acute peripheral polyneuropathy disorder, ^ 1 , 2 ^ with symptoms including symmetrical progressive flaccid paralysis with or without sensory disturbances. ^ 3 ^ This syndrome initially involves the distal legs before progressing to the arms and facial muscles. ^ 4 ^ The annual incidence is two cases per 100,000 people, ^ 5 ^ with a higher prevalence in men and the elderly. ^ 3 ^
GBS results from the cross-reaction of antibodies with peripheral nerve epitopes, ^ 3 ^ leading to acute or subacute demyelination or axonal loss in the peripheral nerves and spinal roots. ^ 1 , 2 ^ Patients afflicted with GBS typically show autonomic dysfunction, areflexia, respiratory failure, and absence of cerebrospinal fluid pleocytosis. ^ 6 ^ These symptoms are more likely to ameliorate if appropriate treatment is provided, including plasma exchange (PE) or intravenous immunoglobulins (IVIg), with or without supportive care. ^ 7 , 8 ^ Nevertheless, despite immunotherapy and supportive care, neurological symptoms might persist in approximately 20% of patients, leading to a mortality rate of 5%. ^ 6 ^ Due to the need for mechanical ventilation in most GBS patients, accurate monitoring, treatment, and supportive care in the intensive care unit (ICU)-admitted patients with GBS is critical. ^ 4 ^ The complications in such patients and their effects on patients’ outcomes were investigated in some studies, though in a limited manner. ^ 3
- 5 , 7 , 9
- 18 ^ Among previous investigations, only one study in Australia and New Zealand used the APACHE II score to evaluate the specific mortality rate. ^ 4 ^
Understanding the morbidity, mortality, and clinical features of ICU-admitted GBS patients is critical in recognizing correctable factors, modifying prognosis, and adjusting medical care. Besides, the disparities between Western and Asian populations, as well as variations in the major risk factors of GBS, highlighted the importance of country-specific studies. Therefore, this study was conducted to investigate the clinical characteristics and outcomes of ICU-admitted GBS patients at Namazi Hospital.
Patients and Methods
Study Design
In this retrospective study, adult patients with GBS, diagnosed by a treating physician, were enrolled and admitted to the ICUs of Namazi Hospital, a major referral center in southern Iran, throughout a 5-year period from March 20, 2016, to March 19, 2021. Patients with a positive history of trauma, myasthenia or other paresis, neuromuscular weakness, or poliomyelitis were excluded.
Study Procedure
Data were gathered from the Iran Intensive Care Unit Registry (IICUR), as well as the admitted patients’ paper-based and electronic medical records. The study protocol was approved by the Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran (IR.SUMS.MED.REC.1399.871). Since the study was retrospective, there was no need to obtain informed consent.
The patient’s demographic information, clinical profile, electrophysiological findings, treatments administered, ICU complications, and admission outcomes were all recorded. Using the Brighton criteria, the degree of certainty in the GBS diagnosis was classified into four levels (table 1). ^ 19 ^ Table 1. Brighton criteria levels of diagnostic certainty of Guillain-Barre syndrome.VariablesLevel 1Level 2LevelLevel 4Bilateral and flaccid weakness of limbs++++/-Decreased or absent deep tendon reflex in weak limbs++++/-Monophasic course and time between onset-nadir 12 hours and 28 days++++/-CSF cell count <50/microliter++-+/-CSF protein concentration>normal value++/--+/-NCS finding consistent with one of the subtypes of GBS++/--+/-Absence of alternative diagnosis for weakness++++CSF: Cerebrospinal Fluid; NCS: Nerve Conduction Study; GBS: Guillain-Barre Syndrome; +: present; -: absent.
After obtaining the necessary permissions and approvals, specialized neurological information was extracted from the patient’s paper records. The pattern of nerve conduction velocity was reported as normal, equivocal, demyelinating, or axonal. Comorbidities included organ dysfunction (such as liver, kidney, cardiac, and pulmonary disease), diabetes mellitus, infections, and metastatic malignancies. The APACHE II score was determined within the first 24 hours of ICU admission using the online calculator (https://clincalc.com/IcuMortality/APACHEII.aspx). ^ 20 ^ The Research Council Manual Muscle Testing scale was utilized to measure the strength of the muscles. ^ 21 ^ In this method, the muscles of the upper and lower extremities were tested against the examiner’s resistance, and the patient’s strength was graded using an ordinal scale: 0: no visible muscle contraction (complete paralysis); 1: trace muscle activation, such as a twitch, without achieving full range of motion; 2: muscle activation with gravity eliminated, achieving full range of motion; 3: muscle activation against gravity, full range of motion; 4: muscle activation against some resistance, full range of motion; 5: muscle activation against examiner’s full resistance, full range of motion.
Statistical Analysis
Data were recorded in Microsoft Excel software 2010 (Microsoft, Redmond, WA, USA) and analyzed using SPSS software (version 21, IBM, New York, United States). For descriptive analysis, the frequency, percentage, mean, median, standard deviation, and interquartile range were calculated and reported.
Results
During the five-year study period, 132 patients with GBS (83 men, 49 women) were admitted to the adult ICUs of Namazi Hospital (table 2). The majority of patients were men (62.6%), and their mean age was 47.87±15.41 years. Most patients had Brighton criteria level 2 certainty of diagnosis (64.5%), and 32% had level 3 diagnostic certainty. Just over one-fifth of patients (22%) had complete quadriplegia or only limited upper and lower limb movement. Indications for ICU admission were airway protection, respiratory failure, autonomic dysfunction, and the need for close observation. Almost all patients (97%) received immunomodulatory therapy. 73 patients out of 132 (55%) received IVIg treatment, 38 patients (28.7%) received plasmapheresis (PLEX), and 16 patients received both PLEX and IVIg. The in-hospital mortality rate was 3.8%.
Based on the electrophysiological evaluation, a considerable proportion (58.5%) were classified as having axonal disease, and 41.5% had demyelinating disease (table 2). The electrophysiological classification was significantly associated with muscle weakness. About 51.4% of axonal patients had limb power <3, and 36% had demyelinating type. This group also required mechanical ventilation more frequently (54% vs. 46%) and for a longer duration (26 [9–37] vs. 10 [1–61] days). Patients with axonal criteria electrophysiological test results (66% vs. 34%) were more likely to require prolonged ventilator support (>14 days).
Intensive Care Unit Complications
As shown in Table 3, one-fourth of the GBS patients suffered at least one serious complication during their stay in the ICU. Pneumonia and sepsis were observed to the same extent in 12.3% of patients, while a urinary tract infection was seen in 9.2%. Pain was reported in 20% of participants, most often reported as back pain. Pain was mostly treated with opioids, gabapentin, and nonsteroidal anti-inflammatory drugs.
Nerve Conduction Study Findings
The results of the nerve conduction examination showed that the most common variations of GBS were Acute inflammatory demyelinating polyneuropathy (AIDP, 41.5%), Acute motor axonal neuropathy (AMAN, 38.5%), and Acute motor sensory axonal neuropathy (AMSAN, 20%) (figure 1).
The figure shows the types of Guillain-Barre syndrome. AIDP: Acute inflammatory demyelinating polyradiculoneuropathy; AMAN: Acute motor axonal neuropathy; AMSAN: Acute motor sensory axonal neuropathy; GBS: Guillain-barre syndrome
Discussion
To the best of our knowledge, this is the first study to assess the clinical characteristics and outcomes of GBS patients admitted to ICUs of a large teaching hospital in southern Iran. In this study, 132 patients were enrolled. The mean age of the patients was 47.87±15.41 years. The findings of the present study were in accordance with the findings reported by Saroj Kumar Bhagat ^ 22 ^ and Rajat Dhar and others. ^ 10 ^ The same as a previous study, ^ 23 ^ the present study had a male predominance in cases of GBS, with male-to-female ratios of 1.69:1. Axonal involvement was found in a considerable proportion of our cases (58.5%), which was associated with muscle weakness. In a way, almost half of these patients had limb power less than 3. They also required mechanical ventilation more frequently and for a longer duration. In the present study, axonal involvement was higher than in other similar studies. ^ 10 , 23 ^ The definite criteria and the electrophysiological protocol for determining the type of nerve involvement have a significant impact on the relative frequency of the various forms of GBS. However, according to a previously published study, ^ 24 ^ the findings of the present study indicated that patients with axonal disease had a longer duration of mechanical ventilation and required a longer time to achieve independent ambulation.
The present study indicated that about 21.5% of patients were supported by mechanical ventilation, similar to data reported by Sedano and others from Spain ^ 25 ^ and Arami and colleagues from northwest Iran. ^ 23 ^ However, it was lower (55.9%) than the results reported by Yakoob and others in a tertiary care center in Pakistan, ^ 26 ^ which could be attributed to the larger number of hospital-acquired pneumonia cases in that study.
The in-hospital mortality rate for GBS in the present study was 3.8%. Sharma and others conducted a study in Nepal among the pediatric population and found that the in-hospital mortality rate of GBS was 7.4%, ^ 27 ^ while Kalita and others reported 6.8% in India. ^ 28 ^ The mortality proportion in our study was higher than that reported by Alshekhlee and others (2.58%). ^ 29 ^ The disparity in mortality rate could be attributed to the quality of health care provided by hospitals, the average age of the participants, and the patient’s disease severity. In the present study, most patients had good functional outcomes (92.8%), which was consistent with the findings of Rees and others (88%) from southeast England. ^ 30 ^
In this study, pneumonia and sepsis were each observed in 16% of patients, and urinary tract infections were diagnosed in 12% of patients. In accordance with other previous studies, ^ 10 , 31 ^ one-fourth of patients experienced pain, which was mostly treated with opioids, gabapentin, and nonsteroidal anti-inflammatory drugs. In a study conducted by Kalita and colleagues, pneumonia was observed in 34.4% of mechanically ventilated and 3.4% of non-ventilated patients with GBS. ^ 28 ^ Another study reported that 82% of GBS patients had complications during their ICU stay, with pneumonia and tracheobronchitis being the most prevalent. ^ 16 ^
The in-hospital mortality of GBS in the present study was (3.8%), which was within the 3.2-8% range reported in other published studies. Airway protection and the prevention of atelectasis with timely mechanical ventilation could reduce mortality in these patients. ^ 22 , 23 , 32 ^
In the present retrospective study, no automated script-based software was used, and the data were extracted manually. In studies dealing with large amounts of data, human error and misinterpretation of data might occur during manual extraction, and some information might be incomprehensible. Moreover, the present study was single-center in nature; nonetheless, it was conducted at the largest referral center in the South of Iran. Although the present sample size was sufficient for statistical analysis, we could not identify the factors affecting early mortality. Therefore, it is recommended to design prospective multicenter studies to generate high-quality data on the study topic.
Conclusion
The findings of this study suggested that patients classified as having axonal disease according to electrophysiological study criteria represented a larger proportion than previously reported cases. These patients required mechanical ventilation more frequently and for a longer duration than those in other electrophysiological study categories.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kilic B Gungor S Ozgor B Clinical, electrophysiological findings and evaluation of prognosis of patients with Guillain-Barre syndrome Turk J Pediatr 201961200810.24953/turkjped.2019.02.00832077646 · doi ↗ · pubmed ↗
- 2Ohnari K Okada K Mafune K Kusunoki S Adachi H Unclassified subtype of Guillain-Barre syndrome is associated with quick recovery J Clin Neurosci 202191313810.1016/j.jocn.2021.07.02534373045 · doi ↗ · pubmed ↗
- 3Leonhard SE Conde R Mde Assis Aquino Gondim F Jacobs BC Diagnosis and treatment of Guillain-Barre syndrome during the Zika virus epidemic in Brazil: A national survey study J Peripher Nerv Syst 2019243407[ PMC Free Article ]10.1111/jns.1235831746070 PMC 6972698 · doi ↗ · pubmed ↗
- 4Ancona P Bailey M Bellomo R Characteristics, incidence and outcome of patients admitted to intensive care unit with Guillain-Barre syndrome in Australia and New Zealand J Crit Care 201845586410.1016/j.jcrc.2018.01.01629413724 · doi ↗ · pubmed ↗
- 5Kishore CK Vijayabhaskar J Vishnu Vardhan R Sainaresh VV Sriramnaveen P Sridhar A Vetal Management of Guillain-Barre syndrome with plasmapheresis or immunoglobulin: our experience from a tertiary care institute in South India Ren Fail 201436732610.3109/0886022 X.2014.89085924593239 · doi ↗ · pubmed ↗
- 6Wen P Wang L Liu H Gong L Ji H Wu Hetal Risk factors for the severity of Guillain-Barre syndrome and predictors of short-term prognosis of severe Guillain-Barre syndrome Sci Rep 20211111578[ PMC Free Article ]10.1038/s 41598-021-91132-334079013 PMC 8172857 · doi ↗ · pubmed ↗
- 7Yonezawa N Jo T Matsui H Fushimi K Yasunaga H Effect of Early Tracheostomy on Mortality of Mechanically Ventilated Patients with Guillain-Barre Syndrome: A Nationwide Observational Study Neurocrit Care 20203375968[ PMC Free Article ]10.1007/s 12028-020-00965-932291575 PMC 7223482 · doi ↗ · pubmed ↗
- 8Shi M Zhu J Deng H Clinical Characteristics of Intravenous Injection of Monosialotetrahexosyl Ganglioside Sodium-Related Guillain-Barre Syndrome Front Neurol 201910225[ PMC Free Article ]10.3389/fneur.2019.0022530930839 PMC 6428729 · doi ↗ · pubmed ↗