Association of Intestinal Helminthiasis with Disseminated Leishmaniasis, Brazil
Brady Page, Alexsandro Lago, Edgar M. Carvalho

TL;DR
This study investigates if co-infection with intestinal helminths affects clinical manifestations or treatment response in Brazilian patients with disseminated leishmaniasis.
Contribution
The study explores the impact of intestinal helminth co-infection on disseminated leishmaniasis, a less understood clinical form.
Findings
Co-infection by L. braziliensis and intestinal helminths does not affect clinical manifestations in cutaneous leishmaniasis.
The study evaluates the association in disseminated leishmaniasis patients in Brazil.
Findings may inform treatment approaches for co-infected patients.
Abstract
Disseminated leishmaniasis is an emerging clinical form of Leishmania braziliensis infection. Evidence shows that co-infection by L. braziliensis and intestinal helminths does not affect clinical manifestations or response to therapy in cutaneous leishmaniasis patients. We evaluated whether co-infection was associated with those aspects in disseminated leishmaniasis patients in Brazil.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
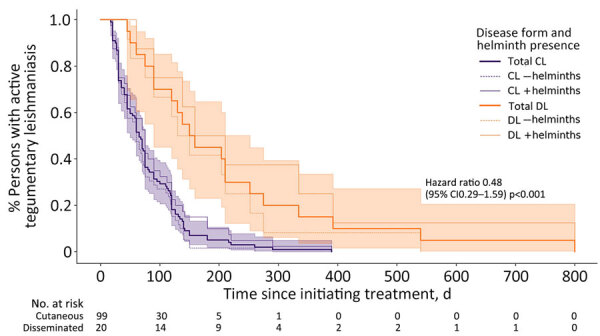 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Helminth infection and control · Parasite Biology and Host Interactions
American tegumentary leishmaniasis represents a group of neglected tropical diseases caused by protozoans of the genus Leishmania and transmitted to humans by phlebotomine sand flies. Brazil has one of the highest incidences of leishmaniasis in the world, where the predominating species is Leishmania braziliensis (1). The disease classically manifests as the localized ulcers of cutaneous leishmaniasis (CL), but in some instances, amastigotes metastasize from the site of inoculation and lead to disseminated leishmaniasis (DL), a severe and poorly understood form of disease characterized by the presence of up to several thousand skin lesions on multiple areas of the body; DL incidence has increased severalfold in recent decades (1).
No histopathologic or immunologic differences have been identified between CL and DL, but several host and parasite factors have been associated with the development of DL, including L. braziliensis strain and immune effector cell function (2,3). Although infection with intestinal helminths has been shown to modulate host immune response to bacterial and viral infections by inducing regulatory and Th2-type T cells, co-infection with L. braziliensis does not definitively affect clinical or therapeutic aspects of CL (4–7). However, a previous study showed an association between helminth infection and mucocutaneous leishmaniasis (8). To better clarify whether the presence of helminths contributes to L. braziliensis dissemination, we evaluated the influence of intestinal helminthiasis on clinical manifestations and response to therapy in DL patients in Brazil.
We recruited participants during January–December 2017 at a dedicated leishmaniasis center in the endemic region of Corte da Pedra in Bahia state, Brazil. Persons 5–70 years of age with skin lesions that had been present <60 days were eligible for enrollment. Criteria for diagnosis of CL were the presence of 1–9 well-demarcated cutaneous ulcers and detection by PCR of L. braziliensis DNA in a punch biopsy taken from a lesion. DL was defined as the presence of >10 cutaneous lesions located on >2 noncontiguous body parts and a positive PCR. At enrollment, participants provided a stool sample. We determined the presence and quantification of intestinal helminth infection by the Kato–Katz method (9). All participants, regardless of enrollment status, were clinically evaluated and treated with 20 mg/kg/day of intravenous meglumine antimoniate for 20 days.
Initial clinical examination consisted of an evaluation of the size and number of cutaneous lesions. Upon 60-day and 90-day follow-up, we evaluated participants for the appearance of new lesions and response to treatment of existing lesions. We considered participants to be cured on the basis of the presence of complete re-epithelialization without elevated borders of all CL or DL lesions within 90 days after the initiation of antimonial treatment.
We enrolled a total of 99 persons with CL and 20 with DL. The median age of participants was 26 years (range 13–69 years); 76.5% of participants were male and 23.5% female (Table). Persons with DL were significantly older than patients with CL (42 vs. 24 years; p = 0.02), although we observed no correlation between age and time to cure in DL patients (R^2^ 0.06; p = 0.5) (Appendix Figure 1). Among persons with CL, age was correlated with time to cure but does not explain much of its variability (R^2^ 0.07; p = 0.04).
The prevalence of intestinal helminthiasis was 40.3% (48/119 patients); we observed no difference in prevalence between the CL and DL patients (Appendix Table). The most commonly identified organisms were Necator americanus (23/119 patients), Trichuris trichiuris (19/119 patients), and Ascaris lumbricoides (14/119 patients). The cure rate after 90 days of treatment was significantly lower in persons with DL compared with those with CL (30% vs. 65.9%; p = 0.003), and the median time to cure was significantly longer (154.5 vs. 65 days; p<0.001) (Figure). We observed no significant difference in the median number of lesions, median area of largest lesion, cure rate at 90 days, or median time to cure between DL patients with or without intestinal helminthiasis. We also observed no correlation between quantity of helminth ova in stool and time to cure in either group (R^2^ 0.01) (Appendix Figure 2).
Future investigation is needed to expound upon the immunologic and strain-specific parasitologic factors that may compromise the host Th1 immune response. A decrease in Th1-associated interferon-γ and tumor necrosis factor α production may precipitate the development of DL in a minority of patients.
The role of concomitant intestinal helminth infection in the clinical aspects and therapeutic response of CL and DL has thus far remained uncertain. We found a high prevalence of intestinal helminthiasis, but we observed no difference between the CL and DL groups and no effect on outcomes of either disease form. Persons with DL were significantly older than persons with CL, although there was no significant effect within age groups on therapeutic response. Cure rates among persons with DL treated with antimonials were characteristically low compared with persons with CL (10).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Queiroz A, Sousa R, Heine C, Cardoso M, Guimarães LH, Machado PR, et al. Association between an emerging disseminated form of leishmaniasis and Leishmania (Viannia) braziliensis strain polymorphisms. J Clin Microbiol. 2012;50:4028–34. 10.1128/JCM.02064-1223035200 PMC 3503016 · doi ↗ · pubmed ↗
- 2Machado PR, Rosa ME, Costa D, Mignac M, Silva JS, Schriefer A, et al. Reappraisal of the immunopathogenesis of disseminated leishmaniasis: in situ and systemic immune response. Trans R Soc Trop Med Hyg. 2011;105:438–44. 10.1016/j.trstmh.2011.05.00221723576 PMC 3157292 · doi ↗ · pubmed ↗
- 3Oliveira WN, Dórea AS, Carneiro PP, Nascimento MT, Carvalho LP, Machado PRL, et al. The influence of infection by different Leishmania (Viannia) braziliensis isolates on the pathogenesis of disseminated leishmaniasis. Front Cell Infect Microbiol. 2021;11:740278. 10.3389/fcimb.2021.74027834568099 PMC 8462778 · doi ↗ · pubmed ↗
- 4Page B, Lago A, Silva JA, Schriefer A, Lago J, Oliveira L, et al. Influence of intestinal helminth burden on clinical manifestations, therapeutic response, and Leishmania braziliensis load in patients with New World cutaneous leishmaniasis. Am J Trop Med Hyg. 2021;105:1060–6. 10.4269/ajtmh.20-166434398812 PMC 8592135 · doi ↗ · pubmed ↗
- 5Gazzinelli-Guimaraes PH, Nutman TB. Helminth parasites and immune regulation. F 1000 Res. 2018;7:7. 10.12688/f 1000 research.15596.130416709 PMC 6206608 · doi ↗ · pubmed ↗
- 6O’Neal SE, Guimarães LH, Machado PR, Alcântara L, Morgan DJ, Passos S, et al. Influence of helminth infections on the clinical course of and immune response to Leishmania braziliensis cutaneous leishmaniasis. J Infect Dis. 2007;195:142–8. 10.1086/50980817152018 · doi ↗ · pubmed ↗
- 7Newlove T, Guimarães LH, Morgan DJ, Alcântara L, Glesby MJ, Carvalho EM, et al. Antihelminthic therapy and antimony in cutaneous leishmaniasis: a randomized, double-blind, placebo-controlled trial in patients co-infected with helminths and Leishmania braziliensis. Am J Trop Med Hyg. 2011;84:551–5. 10.4269/ajtmh.2011.10-042321460008 PMC 3062447 · doi ↗ · pubmed ↗
- 8Azeredo-Coutinho RBG, Pimentel MI, Zanini GM, Madeira MF, Cataldo JI, Schubach AO, et al. Intestinal helminth coinfection is associated with mucosal lesions and poor response to therapy in American tegumentary leishmaniasis. Acta Trop. 2016;154:42–9. 10.1016/j.actatropica.2015.10.01526519200 · doi ↗ · pubmed ↗