A Recurrent Case of Papillary Eccrine Adenoma
Renee Chang, Armaan Guraya, Renee Lucero, Paul Shitabata

TL;DR
A rare case of papillary eccrine adenoma in a Caucasian male is reported, highlighting its recurrence and diagnostic challenges.
Contribution
This case adds to the limited literature on PEA in non-African American males and emphasizes the importance of accurate diagnosis and complete excision.
Findings
Papillary eccrine adenoma recurred after initial excision in a 75-year-old male.
Histological and immunohistochemical features confirmed the diagnosis of PEA.
Complete excision with a 2 mm margin was performed to prevent further recurrence.
Abstract
Papillary eccrine adenoma (PEA) is a rare benign eccrine gland neoplasm presenting as a solitary nodule, primarily in middle-aged African American females. Accurate histological diagnosis is crucial due to its potential to mimic adnexal carcinomas. Complete excision is recommended due to its risk of local aggression and recurrence. A 75-year-old Caucasian male with a history of basal cell carcinoma (BCC) presented with a recurrent pink, scaly nodule on the right medial pretibial leg area. Initial biopsy showed benign PEA. The lesion recurred after one year, and a re-biopsy confirmed a tubulopapillary adenoma within a scar. The lesion was excised with a 2 mm margin. PEA is characterized histologically by dilated ducts lined by a dual layer of tumor cells, often with intraluminal papillae structures. Immunohistochemical staining aids diagnosis, with markers such as S-100, carcinoembryonic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1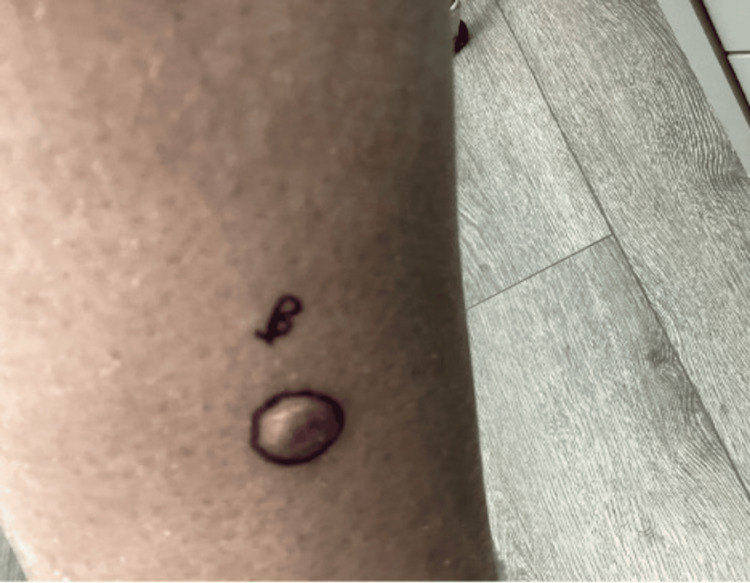 Figure 2
Figure 2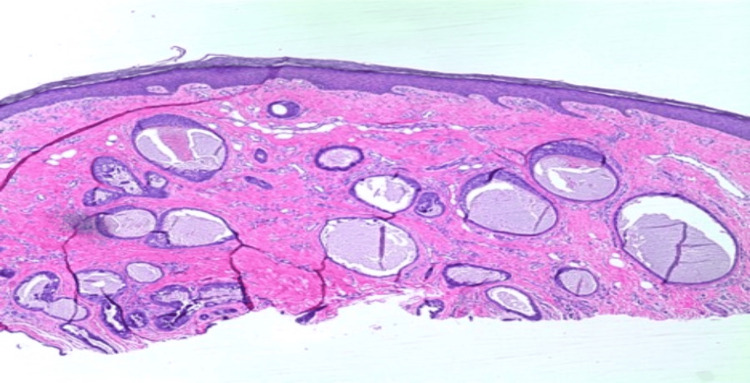 Figure 3
Figure 3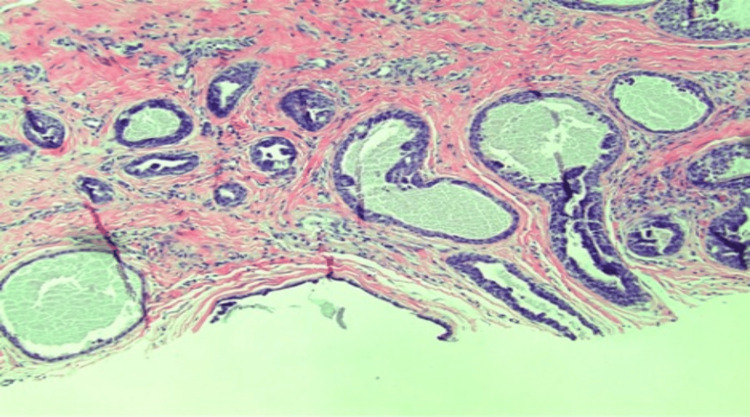 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Ear and Head Tumors · Nonmelanoma Skin Cancer Studies
Introduction
Papillary eccrine adenoma (PEA) is a rare benign eccrine gland neoplasm that typically arises in the distal extremities and appears as a solitary, firm, dome-shaped cutaneous nodule [1,2]. The nodule is normally small, ranging from 0.5 to 2 cm in diameter, and can vary in color, including red, brown, or gray [3]. This adenoma more commonly affects middle-aged African American females [2,3]. It is imperative that PEA is accurately diagnosed histologically as it can mimic adnexal carcinomas [4]. Although slow-growing and benign, complete excision of a PEA may be necessary as it can be locally aggressive and recurrent [5]. The objective of this case report is to improve recognition of this lesion and to better understand how to distinguish it from its malignant counterpart, adnexal carcinomas.
Case presentation
We present a case of a 75-year-old Caucasian male with a history of basal cell carcinoma (BCC). He first presented with a 1.1 cm, pink, scaly, and eroded nodule in the right medial pretibial leg that was present for years (Figure 1). A shave biopsy showed a benign PEA, extending to the deep margin. No evidence of malignancy was noted. The patient returned over one year later with a 1.2 cm smooth, round, pink nodule at the site of the previous biopsy (Figure 2). Re-biopsy of the lesion once again revealed a tubulopapillary adenoma within a scar (Figures 3-4). The sample demonstrated a syringoma-like example of tubular adenoma that persisted after the previous biopsy. The histopathological features in the second biopsy specimen did not suggest adnexal carcinoma. The lesion was then excised with a 2 mm margin due to recurrence and risk of local invasion. Final pathology of the excision showed a proliferation of numerous epithelial strands and tubules with lumens lined by cells of multilayered lining, consistent with PEA.
Right medial pretibial leg with a large pink, centrally eroded nodule
Right medial pretibial leg with recurrent smooth pink nodule
Biopsy showing a proliferation of numerous epithelial strands and tubules with lumens lined by cells of multilayered lining (4x magnification, hematoxylin and eosin staining)
There is a proliferation of numerous epithelial strands and tubules with lumens lined by cells of multilayered lining. Focal papillary morphology and tiny areas of necrosis are noted (10x magnification, hematoxylin and eosin staining)
Discussion
PEA is a benign neoplasm of the eccrine glands with distinct histological features that can pose diagnostic challenges due to its rarity and ability to mimic adnexal carcinomas. Differential diagnoses include adnexal carcinomas and BCC with eccrine differentiation [6]. Histologically, PEA involves a nonmalignant growth of ducts within the sweat glands, located within the dermis. These ducts are often observed to be dilated, featuring a dual layer of tumor cells. The inner epithelial cell layer frequently exhibits characteristic intraluminal papillations in a cribiform growth pattern [7,8]. Most tumors also have central “comedo-like” necrosis which may mimic ductal carcinoma in situ of the breast, raising the differential diagnosis of a malignant adnexal carcinoma [4]. To confirm a diagnosis of PEA, immunohistochemical staining is key. Positive staining for S-100, carcinoembryonic antigen (CEA), and epithelial membrane antigen (EMA) support differentiation toward sweat gland secretory epithelium [9]. Although a strong S-100 reaction suggests eccrine gland differentiation, it is not always present and thus should not be relied upon solely for confirmation [10]. More dependable markers for indicating an eccrine origin of the tumor include alpha-smooth muscle actin (alpha-SMA), keratin 8, and keratin 14 [6].
It is crucial to differentiate between PEA and malignant adnexal carcinomas. As previously mentioned, PEA typically presents as a single, slow-growing, dome-shaped nodule located on the distal extremities, varying in colors. The characteristic features of PEA must be identified in order to prevent misdiagnosis of PEA as a carcinoma. Features suggestive of PEA include symmetry, branching tubular structures within the lumen, and a stroma distinctly separated from the dermis [8]. Adnexal carcinomas often present as smooth, flesh-colored or yellow, multicystic nodules that develop over several years. Adnexal carcinomas are often asymptomatic and most commonly located in the head and neck region, especially on the lips. They have rare metastatic potential; however, they can infiltrate locally [11]. Recurrence rates of adnexal carcinoma can be up to 47% in the first three years of diagnosis, which is why it is vital to have consistent follow-ups with patients; however, with Mohs surgery, recurrence can drop between 0% and 22% with a five-year follow up [11]. Trends have shown that an all-cause age survival of adnexal carcinoma has been 82% [12]. PEA can resemble BCC with similar tubules and 1-2 layers of cuboidal cells; however, they differ due to their cystic and alveolar areas as well as their local aggressiveness and lack of recurrence if excised with caution [6].
Treatment of PEA typically involves complete excision of the tumor with clear margins to prevent recurrence. Mohs micrographic surgery has also shown to be effective [6]. This patient did not have an excision after the initial biopsy, and his recurrence highlights the importance of recognizing this tumor and performing a prompt excision with appropriate margins. After excision with clear margins, recurrence and metastasis are rare; however, cases have been reported [13]. PEA is a rare benign eccrine tumor that can mimic adnexal carcinomas and necessitates careful pathologic examination and diagnosis to rule out more aggressive carcinomas.
Conclusions
In conclusion, PEA is a rare, benign eccrine gland tumor that poses diagnostic challenges due to its resemblance to more aggressive adnexal carcinomas. Accurate histological diagnosis is essential to differentiate PEA from malignant tumors. While PEA typically follows a benign course, complete surgical excision with clear margins is crucial to prevent recurrence, as demonstrated in this case.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Papillary eccrine adenoma in association with cutaneous horn Am J Clin Dermatol Blasini W Hu S Gugic D Vincek V 179182820071749284610.2165/00128071-200708030-00005 · doi ↗ · pubmed ↗
- 2Papillary eccrine adenoma Arch Pathol Lab Med Cooper PH Frierson HF 55571081984 https://pubmed.ncbi.nlm.nih.gov/6546338/6546338 · pubmed ↗
- 3Papillary eccrine adenoma J Natl Med Assoc White SW Rodman OG 573576741982 https://pubmed.ncbi.nlm.nih.gov/71204917120491 PMC 2552891 · pubmed ↗
- 4Current diagnosis and treatment options for cutaneous adnexal neoplasms with apocrine and eccrine differentiation Int J Mol Sci Płachta I Kleibert M Czarnecka AM Spałek M Szumera-Ciećkiewicz A Rutkowski P 50772220213406484910.3390/ijms 22105077 PMC 8151110 · doi ↗ · pubmed ↗
- 5Tubular apocrine adenoma on vulva: an unusual location Indian Dermatol Online J Jain S Valiulla K Dongre AM Malkar BV 346348920183025880910.4103/idoj.IDOJ_343_17PMC 6137663 · doi ↗ · pubmed ↗
- 6Papillary eccrine adenoma: a recent review of literature Am J Med Case Rep Mathews M Kumar A Fromowitz A Simonhoff B Maroules M Akmal A 30430942016 https://www.sciepub.com/ajmcr/abstract/6579
- 7Breast: ductal carcinoma in situ: DCIS 6 2024 Tozbikian G 2020 https://www.pathologyoutlines.com/topic/breastmalignantdcis.html
- 8Papillary eccrine adenoma--a case of cutaneous sweat gland tumor with secretory and ductular differentiation Pol J Pathol Biernat W Kordek R Woźniak L 319322451994 https://pubmed.ncbi.nlm.nih.gov/7697336/7697336 · pubmed ↗