Prevalence of Malocclusion and Orthodontic Treatment Need in 9- to 12-Year-Old Schoolchildren in Ulaanbaatar, Mongolia
Od Bayarsaikhan, Ochirbal Munkh-Erdene, Tungalagtamir Boldbaatar, Oyundari Gantulga, Eiji Tanaka

TL;DR
This study assesses the need for orthodontic treatment in 9- to 12-year-old children in Ulaanbaatar, Mongolia, finding that about one-third require treatment.
Contribution
The study provides updated data on malocclusion prevalence and treatment needs in Mongolian children using the IOTN index.
Findings
84.5% of children had malocclusion, with Angle Class I being the most common.
Approximately 37.4% of children had moderate or definite need for orthodontic treatment.
Overjet, crowding, and overbite were the most common malocclusions associated with treatment need.
Abstract
Background The prevalence of malocclusion in Mongolia is increasing every year. Estimating the need for orthodontic treatment in the population is crucial for planning orthodontic care services and monitoring oral health programs. Therefore, the present study aimed to assess the need for orthodontic treatment among schoolchildren in Ulaanbaatar, Mongolia, using the Index of Orthodontic Treatment Need (IOTN). Methods A total of 656 schoolchildren aged 9-12 years were enrolled from 8 schools located in urban and suburban areas of 6 districts of Ulaanbaatar city. All the children were assessed according to the two components of the IOTN, the Dental Health Component (DHC) and the aesthetic component (AC). Statistical analyses were carried out using IBM SPSS Statistics for Windows, Version 28 (Released 2021; IBM Corp., Armonk, New York, United States). Results The prevalence of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
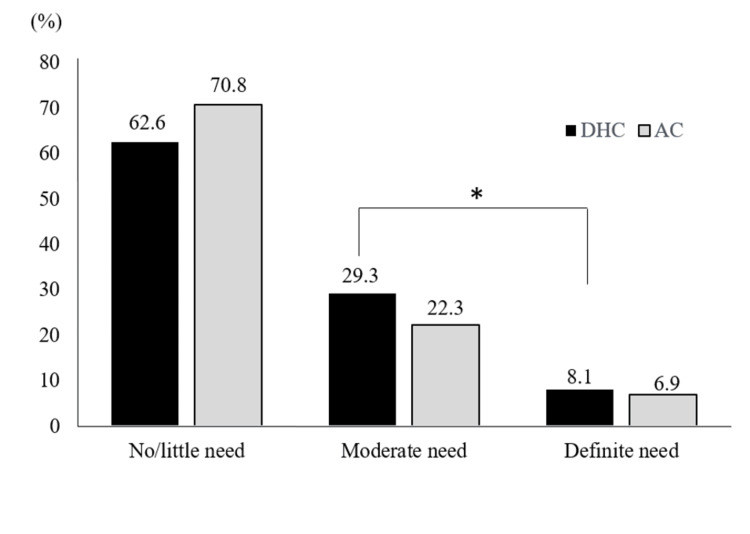 Figure 1
Figure 1| Age/Gender | Urban | Suburban | Total | |||||||
| 18th school | 48th school | 93rd school | 141st school | 57th school | 143rd school | 37th school | 35th school | |||
| 9 years | Boys | 48 (7.3%) | - | - | - | 24 (3.6%) | - | - | - | 72 (10.9%) |
| Girls | 45 (6.8%) | - | - | - | 23 (3.8%) | - | - | - | 68 (10.6%) | |
| 10 years | Boys | - | 61 (9.2%) | - | - | - | 41 (6.3%) | - | - | 102 (15.5%) |
| Girls | - | 59 (8.9%) | - | - | - | 43 (6.6%) | - | - | 102 (15.5%) | |
| 11 years | Boys | - | - | 42 (6.4%) | - | - | - | 52 (7.9%) | - | 94 (14.3%) |
| Girls | - | - | 45 (6.8%) | - | - | - | 50 (7.6%) | - | 95 (14.4%) | |
| 12 years | Boys | - | - | - | 34 (5.2%) | - | - | - | 31 (4.7%) | 65 (9.9%) |
| Girls | - | - | - | 34 (5.3%) | - | - | - | 24 (3.6%) | 58 (8.9%) | |
| Total | 93 (14.1%) | 120 (18.1%) | 87 (13.2%) | 68 (10.5%) | 47 (7.4%) | 84 (12.9%) | 102 (15.5%) | 55 (8.3%) | 656 (100%) | |
| Variables | Gender | p-value | Age | p-value | |||||
| Boys | Girls | 9 years | 10 years | 11 years | 12 years | ||||
| Angle's molar relationship | Class I | 221 | 225 | 0.685 | 114 | 123 | 126 | 83 | 0.706 |
| Class II | 94 | 82 | 40 | 54 | 50 | 32 | |||
| Class III | 17 | 17 | 6 | 7 | 13 | 8 | |||
| AC | No/Little need | 234 | 231 | 0.788 | 109 | 129 | 143 | 84 | 0.265 |
| Moderate need | 73 | 73 | 41 | 43 | 37 | 25 | |||
| Definite need | 25 | 20 | 10 | 12 | 9 | 14 | |||
| DHC | No/Little need | 209 | 202 | 0.97 | 102 | 116 | 119 | 74 | 0.596 |
| Moderate need | 97 | 95 | 42 | 54 | 60 | 36 | |||
| Definite need | 26 | 27 | 16 | 14 | 10 | 13 | |||
| Malocc lusion assessed by DHC | Increased overjet | 114 | 98 | 0.263 | 54 | 42 | 61 | 55 | <0.001* |
| Reverse overjet | 13 | 14 | 0.794 | 4 | 5 | 11 | 7 | 0.247 | |
| Contact point displacement | 102 | 90 | 0.407 | 37 | 68 | 69 | 18 | <0.001* | |
| Anterior or posterior open bite | 5 | 8 | 0.376 | 5 | 1 | 4 | 3 | 0.364 | |
| Increased overbite | 81 | 74 | 0.639 | 27 | 35 | 52 | 41 | <0.003* | |
| Anterior or posterior crossbite | 28 | 31 | 0.612 | 10 | 16 | 19 | 14 | 0.456 | |
| Partially erupted, tipped, or impacted teeth | 49 | 32 | 0.057 | 17 | 22 | 28 | 14 | 0.652 | |
| Submerged deciduous teeth | 6 | 5 | 0.792 | 1 | 8 | 1 | 1 | 0.011 | |
| Variables | Univariate logistic models | Multivariate logistic model 1 | Multivariate logistic model 2 ┤ | |||
| OR (95% CI) | p-value | ORadj (95% CI)┼ | p-value | ORadj (95% CI)┼ | p-value | |
| Gender | ||||||
| Boys | 1 | 1 | ||||
| Girls | 1.02 (0.74-1.41) | 0.873 | 1.22 (0.79-1.88) | 0.352 | ||
| Age | 0.934 | 0.689 | ||||
| 9 years | 1 | 1 | ||||
| 10 years | 1.03 (0.66-1.60) | 0.892 | 1.31 (0.70-2.42) | 0.392 | ||
| 11 years | 1.03 (0.66-1.60) | 0.879 | 1.38 (0.76-2.51) | 0.284 | ||
| 12 years | 1.16 (0.71-1.88) | 0.537 | 1.06 (0.54-2.10) | 0.851 | ||
| AC | <0.001* | <0.001* | <0.001* | |||
| No/little need | 1 | 1 | 1 | |||
| Moderate need | 15.7 (9.94-24.78) | <0.001* | 13.20 (8.04-21.68) | <0.001* | 12.83 (7.86-20.94) | <0.001* |
| Definite need | 51.12 (22.34-120.54) | <0.001* | 45.43 (19.67-98.36) | <0.001* | 41.67 (17.85-85.73) | <0.001* |
| Angle's molar relationship | <0.001* | <0.001* | <0.001* | |||
| Class I | 1 | 1 | 1 | |||
| Class II | 4.25 (2.94-6.15) | <0.001* | 1.94 (1.19-3.15) | <0.008* | 1.93 (1.19-3.11) | <0.007* |
| Class III | 7.99 (3.62-17.63) | <0.001* | 6.21 (2.31-16.66) | <0.001* | 6.09 (2.32-15.98) | <0.001* |
| Increased overjet | ||||||
| None | 1 | 1 | 1 | |||
| Yes | 3.32 (2.36-4.68) | <0.001* | 3.93 (2.39-6.47) | <0.001* | 3.54 (2.25-5.56) | <0.001* |
| Contact point displacements | ||||||
| None | 1 | 1 | 1 | |||
| Yes | 1.988 (1.41-2.80) | <0.001* | 1.66 (1.03-2.66) | <0.034* | 1.72 (1.09-2.70) | <0.019* |
| Increased overbite | ||||||
| None | 1 | 1 | ||||
| Yes | 1.89 (1.31-2.72) | <0.001* | 0.84 (0.49-1.45) | 0.552 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Dental Health and Care Utilization · Oral microbiology and periodontitis research
Introduction
Orthodontics is the most common treatment for various malocclusions and is essential for resolving patients' oral health and aesthetic problems, especially during adolescence and early adulthood [1]. According to a survey in Mongolia, the prevalence of malocclusion tends to increase year by year, such as 64.3% in 1983, 87% in 2004, 79,5% in 2006, and 87% in 2011 [2].
The use of orthodontic indices makes it possible to target individuals with the greatest need for orthodontic treatment when orthodontic resources are limited [3]. Many methods have been developed to assess the need for orthodontic treatment, and one of the most commonly used indices is the Index of Orthodontic Treatment Need (IOTN) [4]. The IOTN has two separate components, the Dental Health Component (DHC) and the aesthetic component (AC), which record anomalies based on the significance of dental health and aesthetic concerns to explore for patients who will most benefit from orthodontic treatment. This specific index provides the opportunity to identify the impact of malocclusion on the dental health and social well-being of the individual [5,6].
Estimating the need for orthodontic treatment among children is crucial for planning an orthodontic care service in terms of human and financial resources, as well as for monitoring oral health programs [7]. Thus, the present study aimed to estimate the need for orthodontic treatment among schoolchildren in six districts of Ulaanbaatar using the IOTN.
Materials and methods
The study was carried out employing an analytical cross-sectional design. A total of 656 schoolchildren aged 9-12 years were recruited as the subjects. They were selected from 129,002 schoolchildren from 8 schools located in urban and suburban areas of 6 districts of Ulaanbaatar city. The inclusion criteria for the participants were an age ranging from 9 to 12, both genders, with no ethical distinction. The exclusion criteria for the participants were a history of orthodontic treatment and congenital dentofacial anomalies. The need for orthodontic treatment was assessed using the components of the IOTN. A minimum sample of 384 children was estimated using a defined need for orthodontic treatment, with a standard error (5%) and a confidence interval (95%). Schoolchildren were randomly selected on the basis of age and school location (four urban, four suburban), with the aim of ensuring a representative sample in relation to the initial population.
The presence of malocclusion and the need for orthodontic treatment were assessed by three examiners in a room reserved by the staff of each school. Prior to performing the assessment, the intra-examiner reliability of the assessment was determined using the interclass correlation coefficient (ICC) on 40 study models selected from the patients with malocclusion by the three examiners twice within two weeks. The ICC was 0.85, confirming the reliability of the assessment. The Research Ethics Committee of the Mongolian National University of Medical Sciences approved this study, and informed consent was obtained from all participants and their parents before the procedures began (No. 2023/3-01).
The DHC recorded malocclusions in terms of the significance of tooth irregularities for an individual dental health. The DHC has a 5-grade scale, ranging from grade 1 to grade 5. Grades 1 and 2 were determined as having no/little need for orthodontic treatment; grade 3 was determined as a moderate need for treatment; and grades 4 and 5 were determined as a definite treatment need. When assessing the DHC, only the worst occlusal condition was recorded.
According to the DHC, the following occlusal features were determined as moderate treatment needs: 1) increased overjet is a malocclusion with 6.0 mm > overjet > 3.5 mm; 2) reverse overjet is a malocclusion with -3.5 mm > overjet > -1.0 mm; 3) contact point displacements are a malocclusion with 4.0 mm > displacements > 2.0 mm; 4) anterior and posterior open bite is a malocclusion with anterior or posterior open bite >2.0 mm, but <4.0 mm; 5) increased overbite is a malocclusion with deep overbite complete on gingival or palatal tissues, but no traumatic occlusion; and 6) anterior and posterior crossbite is a malocclusion with anterior and/or posterior unilateral or bilateral crossbite with >2.0 mm discrepancy.
In addition, the presence of partially erupted, tipped, or impacted teeth and submerged deciduous teeth were recorded and evaluated for the DHC grading.
The AC consisted of 10 different levels of dental attractiveness. The grade 1 represents the most attractive, while the grade 10 represents the least attractive arrangements of teeth. Grades 1 to 4 indicate no/little need for treatment; grades 5 to 7 were determined as a moderate need for treatment; and grades 8 to 10 were determined as a definite treatment need.
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 28 (Released 2021; IBM Corp., Armonk, New York, United States). Pearson’s chi-square test was used to assess the strength of correlation between variables. Multiple logistic regression was also employed to explore the relationships between orthodontic treatment needs and the independent variables. A probability of less than 0.05 was considered statistically significant.
Results
Table 1 shows the demographic characteristics of the study participants. With respect to the DHC score, 194 schoolchildren (29.3%) were determined as the moderate treatment need and 53 schoolchildren (8.1%) were determined as the definite treatment need. According to the AC score, 148 students (22.3%) were classified a moderate need for orthodontic treatment, and 45 students (6.9%) were classified a definite treatment need. The relationship between the DHC and the AC was found to be statistically significant (p<0.001 by Pearson’s chi-square test) (Figure 1).
Orthodontic treatment needs evaluated by DHC and AC: statistically significant difference at the 5% levelDHC: Dental Health Component; AC: aesthetic component*
Neither DHC nor AC showed significant differences between boys and girls (Table 2). In the age phase, these differences were observed in the DHC, an increased overjet, a contact point displacement (crowding), and an increased overbite.
Multiple logistic regression showed that the AC score, Angle’s molar relationship, an increased overjet, and crowding were factors involved in the group with the definite need for treatment (Table 3). A statistically significant cooperation among these factors was noted in the final model. When using a univariate model, other variables were connected to orthodontic treatment needs.
Discussion
The assessment of the objective need for orthodontic treatment in this study provided the baseline data for planning orthodontic services in Ulaanbaatar, Mongolia. The results of the DHC indicated that 37.4% of schoolchildren in Ulaanbaatar had an objective need for orthodontic treatment. The percentage of participants in need of orthodontic treatment was similar to those in other countries such as Russia (38.8%) [8], Thailand (39.7%) [9], New Zealand (31.3%) [10], and Peru (29.9%) [11]. It was higher than that of southern Italian, French, Brazilian, and Romanian schoolchildren (27.3%, 21%, 27.4%, and 15.3%, respectively) [12-15]. However, it was lower than Ethiopian and Hong Kong’s orthodontic treatment needs (48.2% and 52%, respectively) [16,17].
According to the data from the WHO’s Global Oral Health Status Report, most of the countries (France, Italy, New Zealand, and Brazil) with lower prevalence of orthodontic treatment need have different health system approaches than those with a higher treatment needs (Mongolia, Ethiopia, Thailand), such as the presence of dedicated oral health professionals working on non-communicable diseases (NCDs) in the Ministry of Health, the implementation of a tax on sugar-sweetened beverages, the availability of procedures for the detection, management, and treatment of oral diseases in primary care facilities in the public health sector [18]. The availability and affordability of foods with high sugar content and poor access to oral health care services in the community lead to an increasing prevalence of dental caries [19]. A previous study showed that significant associations were found between caries activity and the severity of malocclusion [20]. Thus, caries management is one of the effective ways to reduce the progression of malocclusion [20].
The difference between the DHC (37.4%) and the AC (29.2%) scores in schoolchildren requiring orthodontic treatment may be due to these two components representing different aspects of orthodontic treatment needs using discrete methods [14]. There are dental anomalies that are characterized by the DHC as serious oral health issues but not aesthetically relevant, such as posterior crossbite, missing posterior teeth, unerupted or impacted canines, and premolars [10,21]. The DHC also includes other problems such as crowding, which is not a significant indicator for treatment in AC grading scales. On the other hand, some cases are defined as having a high need for treatment by the AC alone, because certain malocclusions that are considered to be unattractive aesthetics are not evaluated by the DHC. AC differs from the exact measurement parameters of the DHC, for example, AC scaling photographs do not show anterior spacing, hypodontia, and increased overbite, and there is also the possibility that grading may vary depending on the assessing orthodontist [22].
This study showed that the main occlusal anomalies responsible for classifying students as having a high need for orthodontic treatment were an increased overjet, a deviation of the molar relationship from Class I, an increased overbite, and crowding. Severe caries and early extraction of deciduous teeth may become a cause of contact point displacement and migration of the permanent first molars, leading to the inclination and rotation of permanent teeth [14,23]. The inclination of the tooth or an imbalance between the maxillary and the mandibular arch widths may cause a crossbite [24]. These conditions are preventable, early treatment of second deciduous molars that are still functioning can prevent arch length discrepancies [25]. However, if left untreated, they can lead to asymmetric growth of the maxilla or mandible and dental complications that are difficult and costly to treat [26].
The limitation of this study is the selection bias. Due to logistical constraints, we were unable to include schoolchildren from all districts of Ulaanbaatar. Additionally, the number of participants in different age groups varied, which may have affected the accuracy of our results.
Conclusions
The prevalence of malocclusion in 9-12-year-old schoolchildren is high, with approximately one-third of the participants requiring orthodontic treatment. Furthermore, these findings will help dental practitioners better understand the oral health problems that may be affected by different types of malocclusion, leading to an improvement in the overall quality of life for children. The results show that the need for orthodontic treatment, as assessed by the DHC, increases with age. This suggests that early diagnosis and orthodontic treatment can prevent more serious problems.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Quality of life and its importance in orthodontics J Orthod Cunningham SJ Hunt NP 1521582820011139553110.1093/ortho/28.2.152 · doi ↗ · pubmed ↗
- 2Perception and attitude of Mongolians on malocclusion J Dent Sci Narangerel G Hsin-Chung Cheng J Ganburged G Sainbayar B Yi-Hsuan Lee T 13561363172022 https://doi.org/10.1016/j.jds.2022.02.0093578412010.1016/j.jds.2022.02.009PMC 9236961 · doi ↗ · pubmed ↗
- 3The prevalence of malocclusion and orthodontic treatment need in a sample of Syrian children Eur Sci J Ayhab BA Fayez KS Esam O 18577881102014 http://www.researchgate.net/publication/354918263
- 4An insight into four orthodontic treatment need indices Prog Orthod Borzabadi-Farahani A 1321421220112207483810.1016/j.pio.2011.06.001 · doi ↗ · pubmed ↗
- 5The importance of orthodontic treatment need index in the correct assessment of orthodontic therapy Rom J Oral Rehabil Sorana R Carmen S Ramona Fe Carina B 20667000112013 http://www.rjor.ro/wp-content/uploads/2019/10/
- 6The development of an index of orthodontic treatment priority Eur J Orthod Brook PH Shaw WC 309320111989279222010.1093/oxfordjournals.ejo.a 035999 · doi ↗ · pubmed ↗
- 7IOTN index based malocclusion assessment of 12 year old school going children in Mysore city Int J Adv Res Avinash Bh Shivalinga BM Muralidhar NV Avinash BS Shekar S Pradeep S 1235124032015 https://www.journalijar.com/uploads/377_IJAR-6593.pdf
- 8Orthodontic treatment need in school-age children in the Leningrad region (Article in Russian)Stomatologiia (Mosk) Bagnenko NM Bagnenko AS Grebnev GA Madai DY 485395201610.17116/stomat 201695248-5327239997 · doi ↗ · pubmed ↗