Ocular Hornet Injury: A Case Report on Corneal Microperforation and Endophthalmitis
Muhammad Hafiz As-Shaarani Mohd Amin, Abdul-Hadi Rosli, Adzura Salam

TL;DR
A 76-year-old farmer developed severe eye damage and infection after a hornet sting, highlighting the need for prompt and specialized treatment.
Contribution
This case report presents a rare instance of corneal microperforation and endophthalmitis caused by an ocular hornet injury.
Findings
A retained hornet stinger in the cornea led to microperforation and subsequent endophthalmitis.
Standard antibiotic treatments failed to prevent infection, requiring a scleral patch procedure.
The case emphasizes the importance of rapid and specialized management to prevent vision loss.
Abstract
The lesser-banded hornet (Vespa affinis indosinensis) is a prevalent species in tropical and subtropical regions of Asia, including Malaysia. Its stings can result in local reactions, severe anaphylactic shock, and even death. We report a rare case of corneal microperforation and endophthalmitis following an ocular hornet injury. A 76-year-old farmer was attacked by hornets and suffered multiple stings, including one to his right eye. He developed right eye pain, redness, and visual impairment. Ocular examination revealed right corneal haziness with a retained stinger. Attempts to remove the retained stinger were unsuccessful, as the stinger broke and stayed deep in the corneal tissue layer. Corneal microperforation occurred at the site of the retained stinger. Subsequently, he developed endophthalmitis despite extensive topical and systemic antibiotics. He also required a scleral patch…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
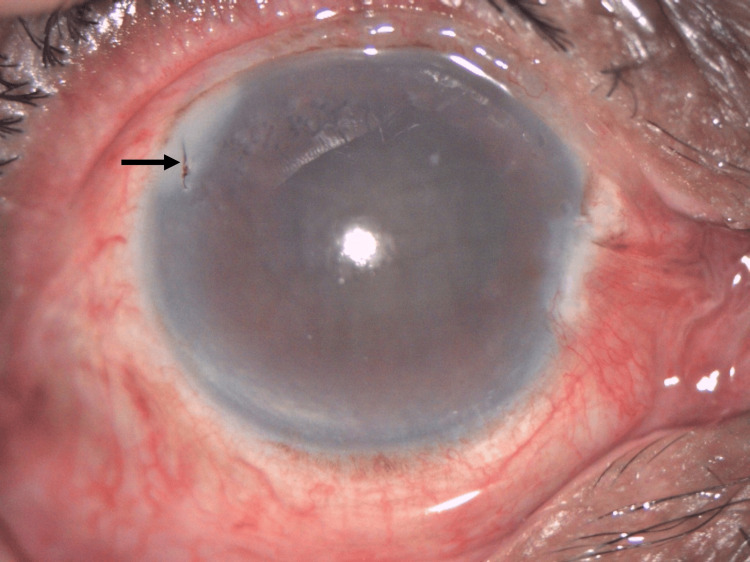 Figure 1
Figure 1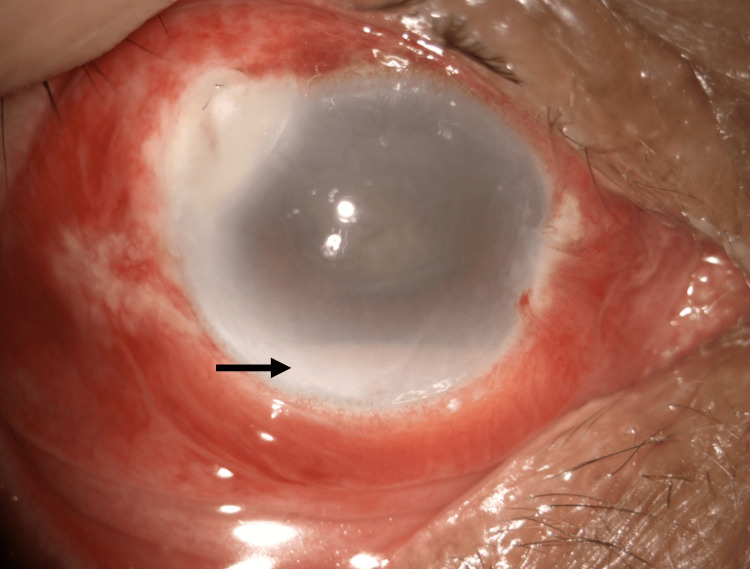 Figure 2
Figure 2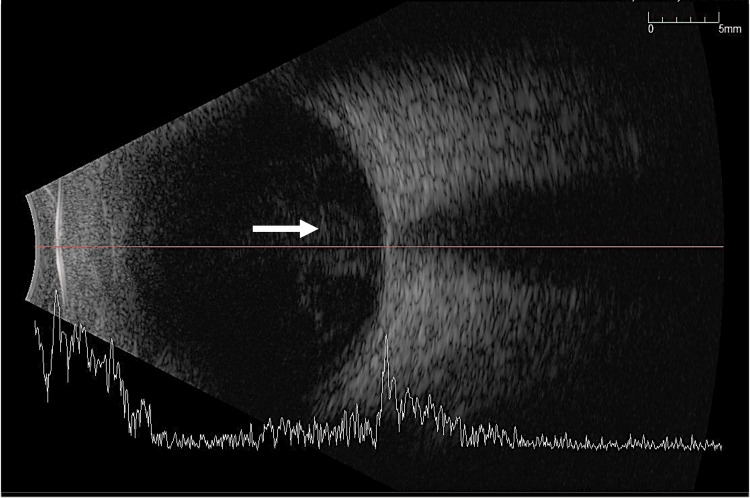 Figure 3
Figure 3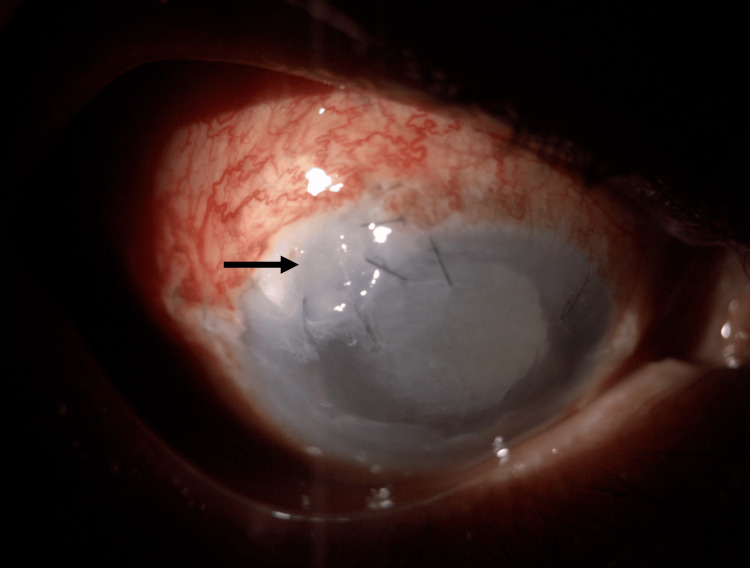 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTurtle Biology and Conservation · Corneal surgery and disorders · Ocular Infections and Treatments
Introduction
The lesser-banded hornet (Vespa affinis indosinensis) is a common hornet in tropical and subtropical Asia, including Malaysia [1]. Hornet sting injuries have been reported as rare incidents, but their potential severity and complications make it important to understand the nature of such occurrences. Hornets, with their black and white bodies and yellow head strips, are known for protecting their nests fiercely and can become aggressive when they perceive any disturbance in their vicinity [2]. Disturbances to their nests can lead to multiple sting injuries, which can have unpredictable complications and even result in death [3]. These stings can cause allergic reactions in victims, ranging from local cutaneous manifestations to potentially life-threatening anaphylactic reactions [4,5]. Furthermore, hornet stings have been associated with a range of systemic and organ-specific complications, including myocardial infarction, multiple organ failure, myasthenia gravis, mastocytosis, and reversible optic neuropathy [6]. The incidence of ocular complications following hornet stings depends on factors such as the location and extent of stings, the presence of retained stingers, and individual patient characteristics. In this case report, we present a rare case of corneal microperforation and endophthalmitis following an ocular hornet injury. This article was previously presented as a meeting abstract at the International Virtual Medical Research Symposium 2023 on December 7 and 8, 2023.
Case presentation
A 76-year-old male was attacked by a swarm of hornets on his palm oil plantation. He suffered multiple hornet stings over his face, bilateral hands, and right eye. At the primary health care facility, he received intravenous hydrocortisone, intramuscular pain relief, and intramuscular adrenaline to alleviate pain and address potential allergic reactions. Eventually, he complained of right eye pain, redness, gritty sensations, and reduced vision. He was referred to the ophthalmology department for further evaluation and management.
Upon examination, the visual acuity in the right eye was 6/60 unaided, with no improvement on pinhole testing. The left eye had a visual acuity of 6/7.5 unaided. Intraocular pressure was within normal limits in both eyes. The anterior segment examination of the right eye showed generalized haziness in the cornea, with a retained stinger in the peripheral area at 10 o’clock (Figure 1). The anterior chamber was deep, with no signs of inflammation. Fundoscopic examination was limited due to corneal edema. The left eye, conversely, had a clear cornea with nuclear sclerosis grade 1.
Anterior segment image of the right eye showing a retained hornet stinger (black arrow) at the peripheral 10 o’clock position with a generalized hazy cornea
Attempts to remove the retained stinger were unsuccessful as the stinger broke, thus halting the removal of the whole stinger. He was started on topical moxifloxacin 0.5%, topical ceftazidime 5%, topical dexamethasone 0.1%, and intravenous ciprofloxacin 400 mg twice daily. On day 2 of the injury, corneal microperforation occurred at the site of the retained stinger, which was followed by toileting and suturing to the affected area.
He developed endophthalmitis subsequently on day 3 of the injury. There was a presence of hypopyon (Figure 2), and a B-scan showed vitritis (Figure 3). We proceeded with anterior chamber washout; intravitreal vancomycin (1 mg in 0.1 ml), ceftazidime (2 mg in 0.1 ml), and amphotericin B (5 mcg in 0.1 ml) were given in the same setting. Intravitreal amphotericin B was given to prevent fungal infection. Trans pars plana vitrectomy was not performed due to a hazy cornea.
Right eye anterior segment photo showing hypopyon (black arrow)
B-scan of the right eye showing aggregates of vitritis near the posterior pole (white arrow)
Eventually, he developed sclerokeratouveitis on day 11 of the injury, which required a scleral patch procedure (Figure 4). He was closely monitored during his hospitalization, which spanned approximately two weeks, in terms of any signs of infection recurrence, corneal healing, and intraocular pressure fluctuations. He was then discharged with topical moxifloxacin, topical dexamethasone, and artificial tears. Follow-up appointments were scheduled to assess the patient’s progress and address any potential post-treatment complications.
Postoperative image of the right eye following the scleral patch procedure due to microperforation (black arrow)
Discussion
This case report highlights the severity of complications that can arise from ocular hornet injuries. While most individuals experience localized reactions to hornet stings, systemic reactions can occur, leading to severe complications such as corneal microperforation and endophthalmitis [4,7,8]. The ocular involvement in this case was particularly challenging due to the presence of the retained hornet stinger, which increased the risk of ongoing inflammation and infection. Ocular hornet injuries are relatively rare, and the management of such cases can be complex and requires a multidisciplinary approach involving ophthalmologists, infectious disease specialists, and other relevant healthcare professionals. To date, there are no standardized treatment guidelines for ocular hornet injuries, highlighting the need for further research and consensus among medical experts.
In light of this, early recognition of retained ocular foreign bodies following hornet stings is paramount to reduce the risk of severe complications. The occurrence of corneal microperforation in this case underscores the potential for severe ocular damage in ocular hornet injuries. The scleral patch procedure employed is a valuable technique for managing corneal microperforation and preventing devastating outcomes [9].
Additionally, the development of exogenous endophthalmitis is an alarming complication, warranting a closer look at the management of retained ocular foreign bodies. The retained hornet stinger served as a nidus for infection, propagating the inflammatory process and increasing the risk of vision-threatening complications. Anterior chamber washout and the use of intravitreal antibiotics serve as examples of targeted and localized therapy to combat developing endophthalmitis and reduce the microbial load intraocularly [10]. Although the treatment proved successful in this case, further research is needed to explore the optimal antimicrobial agents and dosing strategies for intravitreal injections in ocular hornet injuries.
Conclusions
Immediate and vigilant management is crucial in cases of ocular hornet injuries to prevent serious complications and preserve visual function. The presence of a retained hornet stinger represents a unique challenge, necessitating specialized interventions to mitigate inflammation and infection risk. Healthcare providers should be prepared to manage potential complications associated with ocular hornet injuries, and close follow-up is essential to ensure successful outcomes.
This case report emphasizes the importance of continued research and awareness regarding the management of ocular hornet injuries to optimize patient care and outcomes. Further studies are warranted to establish standardized treatment guidelines and improve the management of ocular complications following hornet stings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hornets (Hymenoptera: Vespinae) of Malaysia Malayan Nat J Martin SJ 7182491995 https://www.researchgate.net/publication/313190501_Hornets_Hymenoptera_Vespinae_of_Malaysia
- 2Defensive behavior of the invasive alien hornet, Vespa velutina, against color, hair and auditory stimuli of potential aggressors Peer J Choi MB Hong EJ Kwon O 09202110.7717/peerj.11249 PMC 803436833868832 · doi ↗ · pubmed ↗
- 3A fatal case of anaphylactic shock caused by the lesser banded hornet, Vespa affinis indosinensis in peninsular Malaysia Trop Biomed Lee HL Krishnasamy M Jeffery J 8182222005 https://pubmed.ncbi.nlm.nih.gov/16880759/16880759 · pubmed ↗
- 4Natural history of the Hymenoptera venom sensitivity reactions in adults: study design Int J Environ Res Public Health PerčičS BojanićL Košnik M Kukec A 43191920223540999910.3390/ijerph 19074319 PMC 8998790 · doi ↗ · pubmed ↗
- 5Immunoreactivity to Meissner corpuscles and dermal nerves in a bullous arthropod bite reaction Our Dermat Online Velez AM Jiménez-Echavarria AM Howard MS 10210382017
- 6A case of Kounis syndrome after a hornet sting and literature review BMC Res Notes Ralapanawa DM Kularatne SA 867720142546520810.1186/1756-0500-7-867PMC 4265414 · doi ↗ · pubmed ↗
- 7Corneal bee sting injuries with different presentations and outcomes - experience in a tertiary hospital in Malaysia Eye South East Asia Lim JJ Choo MM Liew YC 3339132018 https://he 01.tci-thaijo.org/index.php/eyesea/article/view/108143
- 8Bee sting presumed endophthalmitis: a devastating ocular outcome Int J Retina Vitreous Al Amry M Al Ghadeer H Al Gethami AR 52720213448890710.1186/s 40942-021-00320-w PMC 8420068 · doi ↗ · pubmed ↗