Comprehensive Multidisciplinary Management of Hyper-IgE Syndrome in an 11-Year-Old Female: A Pediatric Case Report
Ahmed Elashmawy, Mohammadali Chokr, Saima Sharif, Lauren Ferrantino

TL;DR
This case report details the treatment of an 11-year-old girl with a rare immune disorder causing frequent infections and bone issues.
Contribution
The paper presents a comprehensive management approach for HIES in a pediatric patient with pneumonia and osteopenia.
Findings
The patient required a rigorous course of antibiotics and antifungals for infection control.
Imaging and pathogen cultures were essential for diagnosing and managing the patient's condition.
Effective multidisciplinary care improved the patient's outcomes and reduced infection risks.
Abstract
Hyper-IgE syndrome (HIES) or Job syndrome is a rare immunodeficiency characterized by elevated levels of IgE and recurrent infections, eczema, and connective tissue abnormalities. Patients with HIES are prone to recurrent pyogenic and opportunistic infections due to impaired immune responses. Here, we present the case of an 11-year-old female diagnosed with HIES, who was admitted to the hospital with bacterial pneumonia and leg pain associated with a history of osteopenia. The patient’s clinical course included fever, cough, throat pain, and leg pain. Management involved a rigorous course of antibiotics, antifungals, and cultures of pertinent pathogens, along with imaging of the lower extremity. This case underscores the importance of appropriate management strategies for patients with HIES and their comorbidities to mitigate the risk of infections and improve patient outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
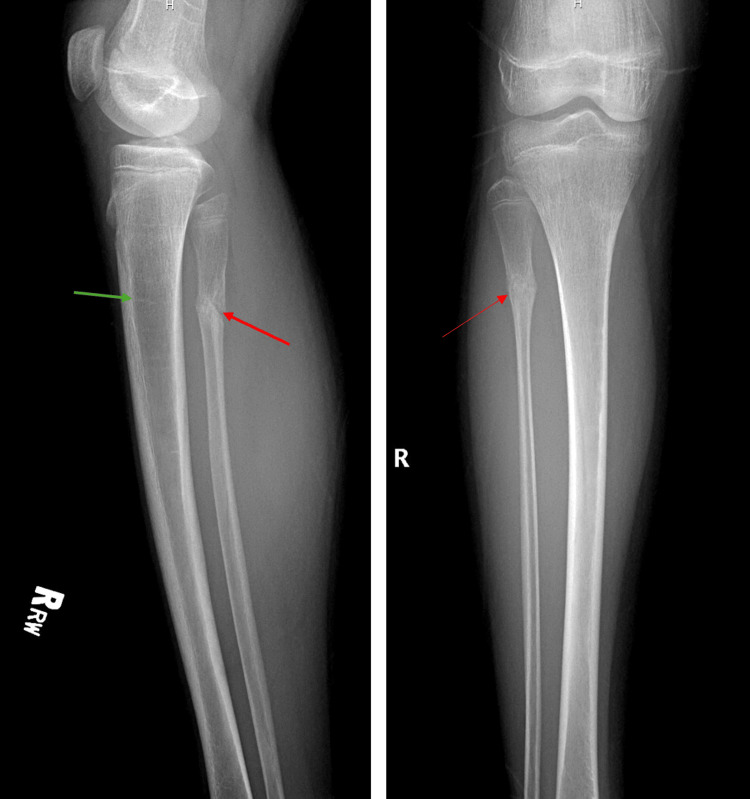 Figure 1
Figure 1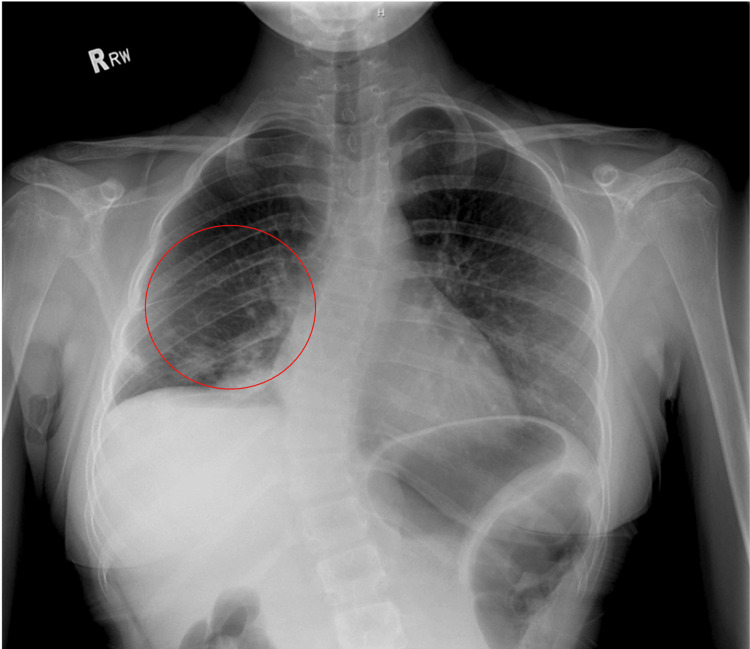 Figure 2
Figure 2| Test Name | Result | Reference Range |
| Rapid Flu A by PCR POC2 | Negative | Negative |
| Rapid Flu B by PCR POC2 | Negative | Negative |
| Rapid RSV by PCR POC2 | Negative | Negative |
| Rapid SARS (COVID-19) PCR POCT | Negative | Negative |
| Sodium | 136 mMol/L | 135-145 mMol/L |
| Potassium | 3.4 mMol/L | 3.5-5.0 mMol/L |
| Chloride | 105 mMol/L | 96-106 mMol/L |
| Carbon Dioxide | 23 mMol/L | 22-29 mMol/L |
| Anion Gap | 8 mMol/L | 3-11 mMol/L |
| Glucose | 94 mg/dL | 70-99 mg/dL |
| Urea Nitrogen (BUN) | 9 mg/dL | 6-20 mg/dL |
| Creatinine | 0.55 mg/dL | 0.6-1.2 mg/dL |
| Bilirubin - Total | 0.28 mg/dL | 0.1-1.2 mg/dL |
| Calcium | 9.7 mg/dL | 8.5-10.2 mg/dL |
| ALT (GPT) | 12 Units/L | 7-56 Units/L |
| AST (GOT) | 16 Units/L | 10-40 Units/Li |
| Alkaline Phosphatase | 184 Units/L | 44-147 Units/L |
| Total Protein | 8.4 gm/dL | 6.0-8.3 gm/dL |
| Albumin | 4.6 gm/dL | 3.5-5.0 gm/dL |
| eGFR CKD-EPI | Not calculated | >60 mL/min/1.73m² |
| WBC | 7.9 K/CUMM | 4.0-11.0 K/CUMM |
| RBC | 4.05 M/CUMM | 4.2-5.9 M/CUMM (men), 3.5-5.5 M/CUMM (women) |
| Hemoglobin | 11.8 gm/dL | 13.8-17.2 gm/dL (men), 12.1-15.1 gm/dL (women) |
| Hematocrit | 35.6% | 40.7-50.3% (men), 36.1-44.3% (women) |
| MCV | 88.1 FL | 80-100 FL |
| MCH | 29.2 pg | 27-33 pg |
| MCHC | 33.2% | 32-36% |
| Red Cell Distribution Width (RDW) | 14.0% | 11.5-14.5% |
| Platelets | 269 K/CUMM | 150-450 K/CUMM |
| Mean Platelet Volume (MPV) | 7.5 FL | 7.5-11.5 FL |
| Manual Diff Review | 1 | N/A |
| Absolute Lymphocyte Count | 1.8 K/CUMM | 1.0-3.0 K/CUMM |
| Lymphocyte % | 23% | 20-40% |
| Absolute Monocyte Count | 0.7 K/CUMM | 0.2-1.0 K/CUMM |
| Monocyte % | 9% | 2-8% |
| Absolute Neutrophil Count | 4.8 K/CUMM | 1.5-8.0 K/CUMM |
| Neutrophil % | 62% | 40-60% |
| Absolute Eosinophil Count | 0.5 K/CUMM | 0-0.5 K/CUMM |
| Eosinophil % | 6% | 1-4% |
| Absolute Basophil Count | 0.0 K/CUMM | 0-0.3 K/CUMM |
| Basophil % | 0% | 0-1% |
| Nucleated RBCs | 0.0 K/CUMM | 0 K/CUMM |
| Adenovirus | Not detected | Negative |
| Bordetella Pertussis | Not detected | Negative |
| Chlamydophila Pneumoniae | Not detected | Negative |
| Coronavirus (COVID-19) PCR - in house | Not detected | Negative |
| Coronavirus 229E | Not detected | Negative |
| Coronavirus HKU1 | Not detected | Negative |
| Coronavirus NL63 | Not detected | Negative |
| Coronavirus OC43 | Not detected | Negative |
| Human Metapneumovirus | Not detected | Negative |
| Influenza A | Not detected | Negative |
| Influenza A 2009 H1 | Not detected | Negative |
| Influenza A H1 | Not detected | Negative |
| Influenza AH3 | Not detected | Negative |
| Influenza B | Not detected | Negative |
| Mycoplasma Pneumoniae | Not detected | Negative |
| Parainfluenza 1 | Not detected | Negative |
| Parainfluenza 2 | Not detected | Negative |
| Parainfluenza 3 | Not detected | Negative |
| Parainfluenza 4 | Not detected | Negative |
| Para-pertussis PCR | Not detected | Negative |
| Resp PCR Spec Description | Nasal | N/A |
| Resp Syncytial Virus | Not detected | Negative |
| Rhinovirus/Enterovirus | Not detected | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsImmunodeficiency and Autoimmune Disorders · Immune Cell Function and Interaction · Blood disorders and treatments
Introduction
Hyper-IgE syndrome (HIES) is a rare primary immunodeficiency disorder characterized by elevated levels of IgE in the presence of recurrent infections, eczema, and a range of other systemic manifestations. This condition, also known as Job syndrome, is associated with a defect in the immune system's ability to respond to infections and regulate allergic responses due to abnormally elevated IgE levels, which normally regulate allergic reactions through mast cell and basophil degranulation [1]. Job syndrome is characterized by a genetic mutation in the STAT3 gene, which impairs the function of T helper 17 (Th-17) cells, which are crucial for managing the body's response to certain pathogens and controlling inflammation [2].
The hallmark of HIES is the combination of recurrent staphylococcal infections, eczema, and elevated serum IgE levels. Patients are particularly susceptible to eczema similar to atopic dermatitis, bacterial and viral skin infections, cold abscesses, respiratory infections with possible pulmonary complications, allergies, gastrointestinal manifestations, malignancies, connective tissue abnormalities, chronic skin infections, sinusitis, and pneumonia due to defects in the immune system's ability to mount effective responses against pathogens [3,4]. The syndrome also often leads to skeletal and dental abnormalities, such as hyperextensible joints and retained primary teeth [5].
HIES presents with a variable clinical spectrum, including features of frequent, severe infections, and chronic eczema. The elevated IgE levels contribute to the heightened allergic responses and contribute to the chronic inflammatory state observed in these patients, with an increased incidence of anaphylaxis [6]. Diagnosis typically involves clinical assessment and confirmation through genetic testing to identify mutations associated with the syndrome.
Here, we present the case of an 11-year-old female diagnosed with HIES, who presented with cough, fever, sore throat, and leg pain associated with osteopenia. This case underscores the complexities of managing immunodeficiencies with elevated IgE and highlights the importance of early therapeutic interventions to mitigate infectious complications and optimize patient outcomes.
Case presentation
Disclaimer: Ethics committee approval and patient consent were obtained and documented through the Wayne State University Institutional Review Board (approval no: 2024 142).
An 11-year-old female with a history of HIES (Job syndrome), osteopenia, and an extensive orthopedic history presented with a dry cough for three days and a fever of 100.2°F for one day. Her mother noted that the cough resembled previous episodes that progressed to pneumonia, but the patient was breathing without dyspnea or tachypnea. She also reported right leg pain. Her diagnosis of Job syndrome was made based on past immunological testing revealing a pathogenic mutation in the STAT3 gene.
The patient also has a past medical history of pulmonary aspergillosis diagnosed on bronchoalveolar lavage (BAL), recurrent pneumonia with a recent Pseudomonas infection, and a right lower lobe lobectomy. Additionally, she also has a history of multiple extremity fractures. Physical examination revealed right leg pain with deep tenderness to palpation, a full range of motion, and weight-bearing without a limp. Her knee was stable with no ligamentous laxity. X-rays showed a healed fracture of the fibula with no new acute fractures or obvious deformities (Figure 1). A possible occult fracture not visible on X-ray was considered, and an MRI was recommended if the pain persisted.
Frontal and lateral radiographs of the tibia and fibulaX-ray reveals a subacute fracture at the proximal fibula diaphysis with early healing signs, chronic osteopenia, and multiple growth arrest lines. Osseous structures are normally aligned, and joints are stable with no acute soft tissue abnormalities.
The X-ray also revealed persistent osteopenia, indicating reduced bone density. This condition is likely due to constant infections and the associated chronic inflammation that negatively impacts bone metabolism. Inflammatory cytokines can promote bone resorption and inhibit bone formation, leading to decreased bone density. The X-ray showed a transverse lucent line at the proximal fibula diaphysis, with mild sclerotic changes and a subtle periosteal reaction, suggesting a subacute fracture with early signs of healing. The bones were normally aligned with no abnormal angulation or displacement, and there was no soft tissue swelling, indicating no significant acute inflammatory response or injury. The knee joint was well-aligned with no dislocations or subluxations. Multiple growth arrest lines in the femur and proximal and distal tibia and fibula indicated periods of interrupted growth and recovery. Overall, the osseous structures were normally aligned, and the joints were stable with no acute soft tissue abnormalities.
The patient was admitted for the management of pneumonia. A chest X-ray is provided below (Figure 2). The X-ray reveals patchy airspace opacities in the right lower lung, indicating lung consolidation typical of pneumonia. The lungs are hypo-inflated, especially on the right side, which aligns with the patient's history of right lower lobectomy. There are new areas of patchy opacities in the right middle lobe. No pleural effusion or pneumothorax is observed. The cardiovascular silhouette appears normal in shape and size. Additionally, there is a curvature in the thoracolumbar spine, suggesting possible scoliosis or another spinal abnormality. In summary, the X-ray shows pneumonia in the right middle lobe, hypo-inflated lungs with post-surgical changes, no acute pleural effusion or pneumothorax, and a normal heart and mediastinum.
Radiograph of the chestX-ray indicates pneumonia in the right middle lobe, hypo-inflated lungs with post-surgical changes, no acute abnormalities like pleural effusion or pneumothorax, and a normal heart and mediastinum. Patchy airspace opacities in the right lower lung are outlined in a red circle.
During the hospital course, she was monitored for fevers and respiratory status. She received four days of IV cefepime 2000 mg every 12 hours and four days of IV clindamycin 600 mg every eight hours for empiric coverage of gram-negative and gram-positive organisms, respectively. Itraconazole 200 mg daily was continued for fungal prophylaxis for four days as well, along with Bactrim prophylaxis as recommended by neurology. A serum galactomannan screen was sent to monitor for aspergillus infection, and a blood culture showed no growth for one day (Table 1). The comprehensive test results from the patient's recent assessment show a generally healthy profile with several notable findings. The patient tested negative for various respiratory viruses including Flu A, Flu B, RSV, and SARS-CoV-2, indicating an absence of some of the more common virus infections (Table 1 shows a list of pathogens tested).
Key blood chemistry markers such as sodium, glucose, and calcium were within normal ranges. However, there were findings of low potassium levels and slightly elevated alkaline phosphatase and total protein levels. The patient received IV cefepime and IV clindamycin. Certain antibiotics can cause renal potassium loss or gastrointestinal loss, leading to hypokalemia. The patient was counseled on oral potassium supplementation in the future to offset this electrolyte abnormality. Hematological parameters revealed a low red blood cell count but a normal white blood cell count with balanced differential counts. These results collectively suggest a stable health condition with mild deviations in electrolytes and hematological indices that may warrant monitoring and follow-up.
Discussion
In this case study, we presented an 11-year-old female with HIES, osteopenia, and a significant orthopedic history, who was admitted with symptoms of pneumonia and leg pain. The patient’s management included empiric antibiotic therapy, antifungal prophylaxis, and close monitoring, highlighting the complexities of treating patients with HIES.
Our key findings indicate that the patient's recurrent infections and osteopenia are significant challenges in managing HIES. These results align with the existing literature, which identifies recurrent staphylococcal infections and skeletal abnormalities as hallmark features of HIES [3-5]. The imaging studies confirmed pneumonia and a subacute fibular fracture, consistent with the expected complications in HIES patients [4].
Compared to previous studies, our findings underscore the necessity of a multidisciplinary approach to managing HIES. The combination of antibiotic and antifungal therapies, along with orthopedic and pulmonary consultations, was crucial in stabilizing the patient. This comprehensive care strategy is supported by similar approaches in other case studies, emphasizing the importance of addressing both infectious and non-infectious complications in HIES [4,7].
However, there are discrepancies in the frequency and severity of infections reported in different studies. Some studies report more frequent respiratory infections and severe immunodeficiency, while our patient exhibited a manageable condition with appropriate prophylaxis and treatment. These differences could be attributed to genetic variations, environmental factors, or differences in healthcare access and quality [8,9].
For this particular case, the use of a comprehensive antibiotics course was meant to ensure broad-spectrum coverage that would protect the patient from the multitude of bacterial pathogens that she is susceptible to due to her condition. Furthermore, the use of prophylactic antifungal therapy, as shown in our patient and her positive response to itraconazole, is essential to preventing opportunistic infections like aspergillosis. This approach is consistent with the literature recommendations, especially given the patient’s history of aspergillosis and the established guidelines on the use of antifungal therapy in immunocompromised patients [7,8]. Effective pain management is also critical to prevent complications such as respiratory atelectasis due to chest wall immobility from uncontrolled pain [9]. Atelectasis is a complication we wish to avoid in patients with respiratory symptoms like this, especially in those who are immunocompromised and prone to such infections. In regard to the patient's osteopenia and her frequent orthopedic problems, the administration of bisphosphonates may be considered in the future to minimize bone loss and reformation [10].
The implications of our findings for clinical practice are significant. They suggest that early diagnosis and a comprehensive, multidisciplinary treatment approach can effectively manage HIES, reduce the frequency of severe infections, and improve overall patient outcomes. Regular monitoring and proactive management of bone health are also critical to prevent and address osteopenia-related complications [5]. Additionally, the heightened allergic responses and chronic inflammatory state observed in these patients underscore the importance of comprehensive care [6].
For policy and further research, our findings highlight the need for guidelines on the multidisciplinary management of HIES. Future studies should focus on the long-term outcomes of different treatment regimens and the impact of early intervention on the quality of life in HIES patients. Additionally, research into the genetic and molecular basis of HIES could provide insights into targeted therapies and personalized treatment plans [2,5]. Our study adds to the understanding of HIES management by demonstrating the effectiveness of a multidisciplinary approach. These findings could influence current practices by promoting comprehensive care strategies and informing future research directions in the field of immunodeficiency disorders.
Conclusions
This case highlights the intricacies of caring for pediatric patients with HIES. In this particular case, the syndrome was complicated by osteopenia and a history of orthopedic issues. Our patient was an 11-year-old female who presented with symptoms of pneumonia and right leg pain. Chest and lower extremity X-rays demonstrated bacterial pneumonia and a subacute fracture of the proximal fibula, respectively. Our treatment plan included empiric antibiotic therapy, antifungal prophylaxis, and close monitoring. A multidisciplinary approach, including pulmonary and orthopedic management, proved beneficial in stabilizing this patient’s condition. We strongly believe that this approach can certainly help other patients with rare immunodeficiencies such as Job syndrome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Role of Ig E in autoimmunity J Allergy Clin Immunol Sanjuan MA Sagar D Kolbeck R 1651166113720162726400010.1016/j.jaci.2016.04.007 · doi ↗ · pubmed ↗
- 2Hyper-Ig E syndrome, 2021 update Allergol Int Minegishi Y 4074147020213441935510.1016/j.alit.2021.07.007 · doi ↗ · pubmed ↗
- 3Staphylococcus aureus and hyper-Ig E syndrome Int J Mol Sci Park B Liu GY 91522120203327176310.3390/ijms 21239152 PMC 7729741 · doi ↗ · pubmed ↗
- 4Hyper Ig E syndromes Curr Pediatr Rev 6 2024 Gracci S Novelli T D'Elios S Bernardini R Peroni D 2532642020243770216710.2174/1573396320666230912103124 · doi ↗ · pubmed ↗
- 5Hyper Ig E syndromes: clinical and molecular characteristics Immunol Cell Biol 6 2024 Al-Shaikhly T Ochs HD 3683799720193026449610.1111/imcb.12209 · doi ↗ · pubmed ↗
- 6Pediatric anaphylaxis and hyper Ig E syndrome J Asthma Allergy Dosanjh A 31331020172828037210.2147/JAA.S 129160 PMC 5338956 · doi ↗ · pubmed ↗
- 7Pulmonary aspergillosis: diagnosis and treatment Eur Respir Rev Lamoth F Calandra T 2201143120223645037210.1183/16000617.0114-2022 PMC 9724826 · doi ↗ · pubmed ↗
- 8Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management Eur Respir J Denning DW Cadranel J Beigelman-Aubry C 45684720162669972310.1183/13993003.00583-2015 · doi ↗ · pubmed ↗