Ping pong fracture
Boumeriem Khaoula, Bourekba Iliass, Ait Belhaj El Mahdi, Allali Nazik, Chat Latifa, El Haddad Siham

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
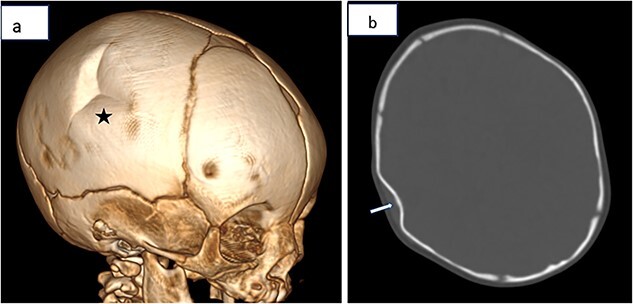 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation
A two-months infant, with no particular medical history, admitted to the emergency department for suspicion of cranial trauma, the physical examination revealed a deformation of the right parietal bone, he then underwent a brain CT scan that showed a depression in the right parietal bone consistent with a typical ping-pong fracture (Figure 1).
A ping-pong ball fracture is an inward depression of the calvarium occurring in newborns and infants due to the malleability of the skull at this age, generally resulting from cranial trauma or traumatic events occurring during the in utero phase or labor [1].
There are two main forms: congenital and acquired. Congenital fractures can occur either before birth or during delivery. Acquired fractures are related to obstetric interventions or postnatal trauma [1].
The diagnosis of a ping-pong ball fracture in a newborn is generally evident during physical examination, presenting as a unilateral depression, most often at the parietal vault, occasionally at the frontal region, and more rarely at the occipital region [2].
Radiological examinations confirm this diagnosis. A simple radiograph can show a focal deformation of the skull with inward indentation. Computed tomography (CT) is the reference examination to assess the extent and shape of the fracture and to exclude associated injuries; it reveals a cranial indentation without a clearly visible fracture line. CT is more sensitive than conventional radiography, reducing errors in interpreting sutures and vascular impressions. Transfontanellar ultrasound is sometimes useful for detecting parenchymal injuries or post-traumatic collections, while MRI is generally limited to cases with uncertain intracranial findings [3].
The therapeutic approach depend on the severity of the depression and the presence of any associated intracranial injury. Small fractures can resolve spontaneously or be treated with non-invasive techniques such as digital manipulation and vacuum devices. However, significant fractures generally require intervention [4].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ilhan O , Bor M, Yukkaldiran P. Spontaneous resolution of a ‘ping-pong’ fracture at birth. BMJ Case Rep 2018;2018:bcr 2018226264.10.1136/bcr-2018-226264 PMC 615749930249736 · doi ↗ · pubmed ↗
- 2Silva JB , João A, Miranda N. Ping-pong fracture in newborn: a rare diagnosis. Acta Medica Port 2019;32:549.10.20344/amp.1072631445537 · doi ↗ · pubmed ↗
- 3Riethmuller D , Forey PL, Equy V. et al. Fracture spontanée «en balle de ping pong» au cours d’un accouchement voie basse. Gynécol Obstét Fertil Sénol 2021;49:706–8.33631393 10.1016/j.gofs.2021.02.004 · doi ↗ · pubmed ↗
- 4Monterrubio RA , González SR, Frías AA. et al. Newborn ping-pong skull fracture and its surgical treatment: a case report. Arch Invest Materno Infantil 2018;9:60–3.