Adult Onset Acute Flaccid Myelitis: A Case Report
Ahmad Peeran, Sameeha Fallatah, Ameera Akour, Ali Alanazi

TL;DR
A 23-year-old man developed severe neurological symptoms consistent with acute flaccid myelitis, but no clear cause or effective treatment was found.
Contribution
This case report highlights adult-onset acute flaccid myelitis to raise awareness among medical professionals.
Findings
The patient's symptoms met CDC criteria for acute flaccid myelitis despite negative tests for common causes.
Multiple treatments failed to reverse the patient's disability, which persisted at discharge.
The case underscores the lack of understanding about the condition's pathophysiology and treatment.
Abstract
We report a 23-year-old male who presented with acute dysarthria, dysphagia, and quadriparesis. These symptoms were preceded by fever and headache. His neurological symptoms were progressive and rendered him quadriplegic over three weeks. Extensive workup for infectious, inflammatory, and neoplastic etiologies was negative; however, the clinical course and magnetic resonance imaging of the brain and spinal cord were consistent with the United States Centres for Disease Control and Prevention (CDC) criteria of acute flaccid myelitis. The patient had various lines of therapy, including antimicrobial agents, intravenous immunoglobulin, plasma exchange, and corticosteroids but he was discharged with significant disability. Despite the increasing number of reported cases worldwide, many aspects of this condition remain unknown including its pathophysiology and optimal treatment regimen. In…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
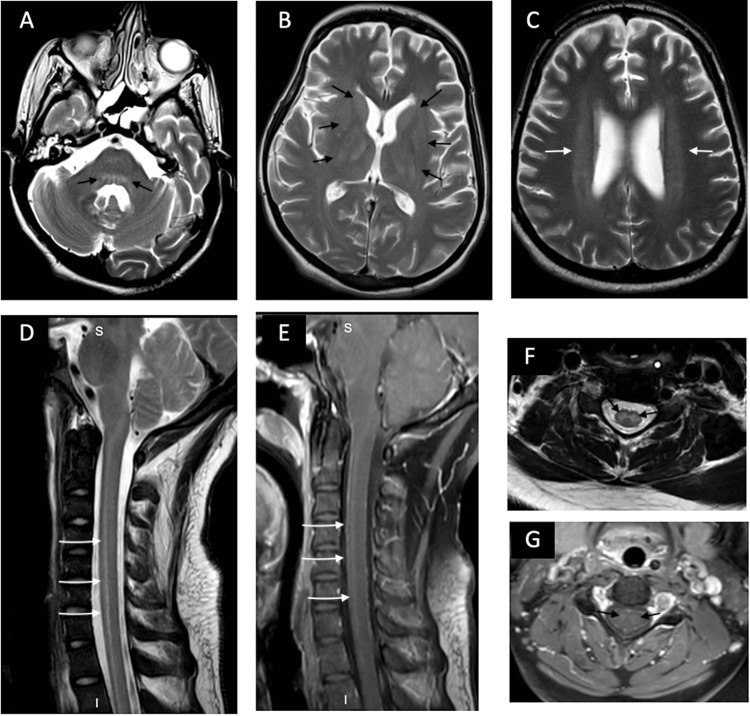 Figure 1
Figure 1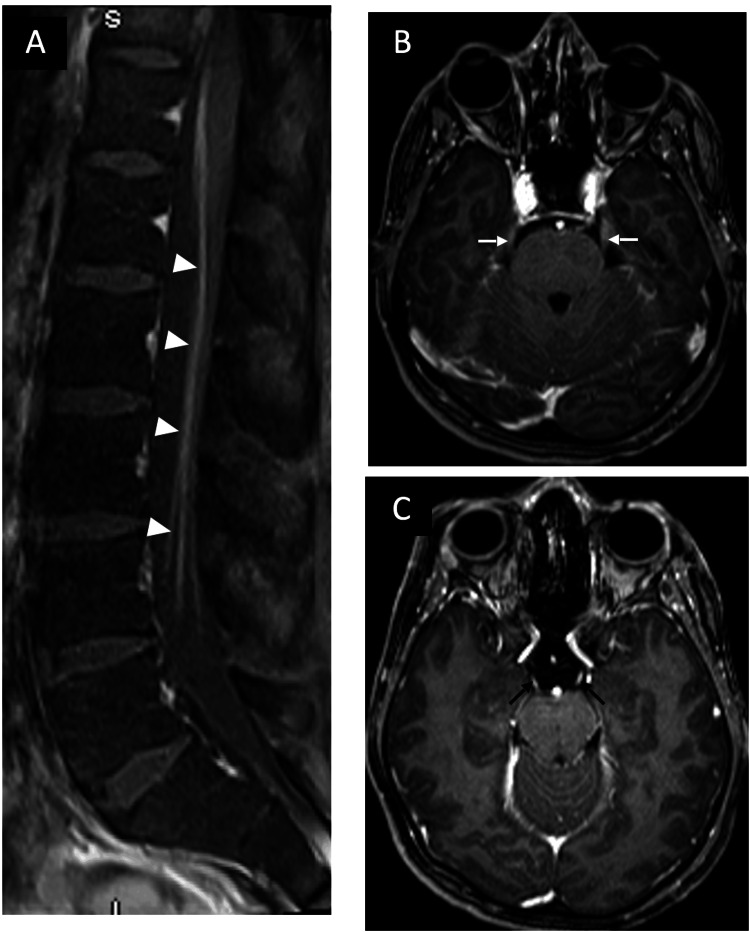 Figure 2
Figure 2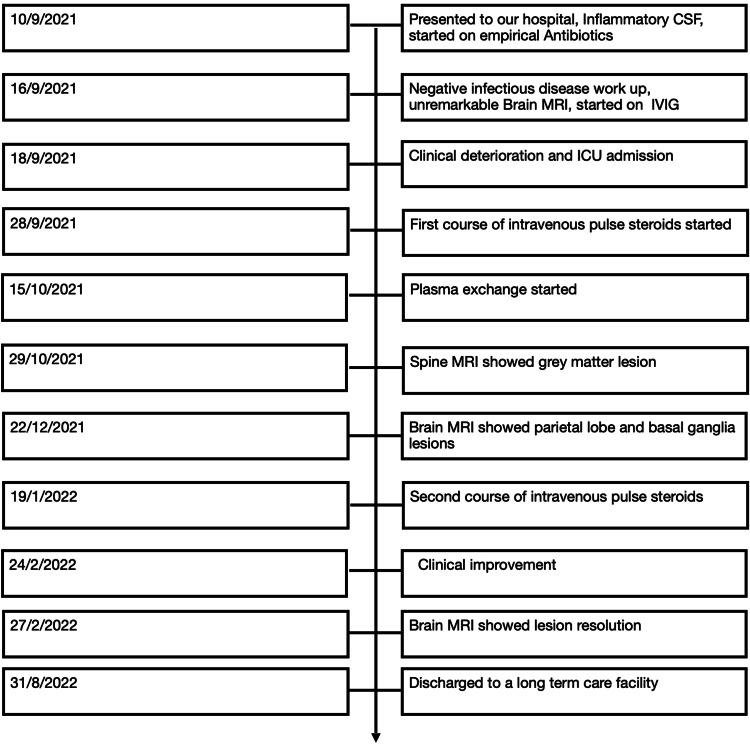 Figure 3
Figure 3| Date | White Cells | Red cells | Protein | Glucose |
| 11/9/2021 | 53 | 2 | 1.04 | 3.6 |
| 14/9/2021 | 18 | 3 | 1.21 | 4.2 |
| 3/10/2021 | 16 | 2803 | 0.47 | 6.1 |
| 29/12/2021 | 2 | 2 | 1.9 | 3.2 |
| 17/1/2022 | <1 | <1 | 1.68 | 3 |
| Serum | Respiratory | Cerebrospinal Fluid |
| Japan Encephalitis virus IgG and IgM | Mycoplasma pneumonia | Human herpes virus 1 |
| Tick born disease (FSME antibodies) | Severe acute respiratory syndrome coronavirus 2 (SARS- COV-2) | Human herpes virus 2 |
| Extractable nuclear antigen antibodies | Bordetella Pertussis | Varicella zoster virus |
| Epstein-Barr Virus-Early antigen | Bordetella Parapertussis | Human Herpeesvirus-6 |
| Epstein-Barr Virus-|gG | Influenza A | Hyman parechoviruse RY |
| Epstein-Barr Virus-IGM | Influenza B | Cytomegalovirus |
| Cytomegalovirus-IgM | Human metapneumovirus | Enterovirus |
| Cytomegalovirus-IgG | Middle east respiratory syndrome coronavirus | Listeria monocytogenes |
| West Nile Virus (IgM, IgG) | Respiratory synctial virus | Syphilis - VDRL |
| Polio virus antibody type 1-3 neutralizing antibody | Human coronavirus NL63 | Escherichia Coli K1 |
| Toxoplasmosis Gondi DNA PCR | Human adenovirus | Hemophilus influenza |
| Human T-Lymphotropic Virus 1 and 2 | Parainfluenza virus 1-4 | Neisseria Meningitides |
| Brucella | Rhinovirus/enterovirus | Streptococcus Agalactiae |
| Syphilis | Human coronavirus 229e | Streptococcus pneumonia |
| Tuberculosis Polymerase chain reaction (PCR) | Human coronavirus 0C43 | Tuberculosis PCR |
| Quantiferon | Human coronavirus HKU1 | Cryptococcus neoformans/gattil |
| Schistosoma antibody | Chlamydophila pneumonia | |
| Herpes Simplex Virus 1 and 2 v Anti-Nuclear Antibody | ||
| Anti-Smooth Muscle Antibody | ||
| Anti-Mitochondrial Antibodv | ||
| Anti Myelin oligodendrocyte glycoprotein antibodies | ||
| Anti-aquaporin 4 antibodies |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Eosinophilic Disorders and Syndromes · Cardiac Structural Anomalies and Repair
Introduction
Acute flaccid myelitis (AFM) is a clinical syndrome characterized by acute flaccid paralysis associated with spinal cord gray matter lesions. The onset of AFM is usually preceded by symptoms that resemble an upper respiratory tract or gastrointestinal infection. After this, patients develop flaccid limb paralysis, which may progress to involve all limbs and cranial motor nerves, leading to oculomotor dysfunction, facial palsy, and/or pharyngeal dysphagia. Magnetic resonance imaging (MRI) characteristically reveals a longitudinal hyper-intense lesion involving the anterior horn of the spinal cord's gray matter on T-2 sequences. Clinical and laboratory/imaging criteria were introduced by the American Centers for Disease Control and Prevention (CDC) to aid the diagnosis and reporting of these cases [1-3]. Since then, numerous cases have been reported from all over the world, including the United States, Europe, and Japan [1,4,5]. Due to the increasing worldwide prevalence of AFM, the prompt recognition and reporting of patients with this condition is crucial to better characterize the disorder and provide research guidance to help establish effective treatment protocols. In this article, we report the case of a 23-year-old male diagnosed with AFM to bring the attention of physicians working in our region to this clinical entity which will facilitate early diagnosis and avoid unnecessary investigations.
Case presentation
A 23-year-old, previously healthy Saudi male presented to a regional hospital in Buraydah with a one-week history of progressive neurological symptoms that started with fever, holocephalic headache, and blurred vision. Then, he developed dysarthria, dysphagia, and quadriparesis, which was more prominent on the left side. The systems review was remarkable for abdominal pain that started a few days before the onset of neurological symptoms. He was initially admitted to a hospital in Buraydah for three days. Brain computed tomography (CT) and Magnetic Resonance Imaging (MRI) scans were done and were unremarkable. Two days after his discharge, he presented to our hospital. On the initial examination, the patient was alert and oriented to the person, place, and time. Comprehension was intact but he had dysarthric speech. Vitals were within normal ranges. He had bilateral ophthalmoparesis with bilateral conjugate gaze-evoked nystagmus and bilateral facial weakness. Power examination revealed 2/5 on the left side and 4/5 on the right side, based on the Modified Medical Research Council scale for muscle strength. Deep tendon reflexes were absent in all limbs. The sensory examination was normal. He was admitted, and over the following eight days, the patient's clinical condition deteriorated gradually; he had a fever, developed flaccid quadriplegia, and became mute. On the eighth day, he was transferred to the ICU and intubated.
Initial serum laboratory investigations showed that the complete blood cell count, electrolytes, renal function, and coagulation profile were all within the normal ranges. Cerebrospinal fluid analysis was done several times, and it initially showed lymphocytic pleocytosis, which improved over the course of the disease (Table 1). Infectious causes and autoimmune etiologies were investigated, and all tests were non-revealing (Table 2).
Furthermore, 16s rRNA sequencing for bacteria and fungi was done on the patient's CSF, and it revealed no trace of microbial DNA. Motor nerve conduction study (NCS) showed normal velocity and severely decreased compound muscle action potentials in all limbs. Sensory NCS was normal. Brain CT and MRI were repeated in our center, and they were initially unremarkable. However, spinal cord MRI showed a T2 hyper-intense signal involving the gray matter of the cervical and thoracic spinal cord. Subsequent brain and spine MRI showed basal ganglia and brainstem lesions, along with post-contrast enhancement in the cauda equina (Figures 1, 2). Also, whole body imaging with PET/CT scan was done, and it was negative for signs of neoplastic or autoimmune conditions.
Brain and spinal cord MRIA, B, and C axial T2-weighted images of the head show bilateral symmetrical hyperintensity in the dorsal pons, deep gray matter, and deep white matter (black arrows in A and B, white arrows in C). D and F are sagittal and axial T2-weighted images that show longitudinal hyperintensity mostly involving the central cord, where the gray matter is situated (White arrows in D, black arrows in F). E and G sagittal and axial post-contrast T1-weighted images demonstrate faint contrast enhancement of the same abnormality (White arrows in E, black arrows in F).
Cranial nerve and nerve root enhancementA, sagittal post-contrast T1-weighted image of the lumbar spine demonstrates anterior cauda equina nerve root enhancement (arrowheads). B and C, axial post-contrast T1-weighted images demonstrate trigeminal (white arrows) and oculomotor (black arrows) nerve enhancement, respectively.
The patient was treated empirically for possible bacterial and viral causes of meningoencephalitis with meningeal doses of ceftriaxone, vancomycin, and acyclovir. However, there was no improvement in his condition and his extensive infectious disease workup was negative. Due to this, treatment for autoimmune conditions was started empirically with intravenous immunoglobulins (IVIG) for five days, but there was no improvement in his condition. One week later, a trial of intravenous methylprednisolone at a dose of 1000 mg was given for three days, after which it was switched to 40 mg for a total duration of 14 days. Also, he was started on plasma exchange but no improvement in his clinical condition was noted. A second trial of steroids was started two months later with methylprednisolone 1000 mg IV for six days, followed by oral prednisone 60 mg.
One month after the second course of steroid treatment, he was able to move his tongue in and out of his mouth and to move his head up and down, which made him able to answer simple questions by nodding his head for yes and staying still for no. Upon discharge, the patient was quadriplegic, on percutaneous gastrostomy tube feeding, and requiring mechanical ventilation via tracheostomy. A complete timeline of the patient's hospital course can be reviewed in Figure 3.
Timeline of patients hospital course
Discussion
The patient presented to our hospital with fever, rapidly progressive flaccid paralysis, and CSF lymphocytic pleocytosis. So, he was started on empirical meningoencephalitis antimicrobial agents. However, the infectious disease workup did not yield any positive results and the patient's clinical condition continued to deteriorate. This raised the possibility of an immune-mediated disease process. Therefore, he received intravenous immunoglobulins (IVIG), plasma exchange, and two courses of pulse steroid therapy. However, his clinical condition did not improve, and the workup for immune-related myelitis, such as anti-aquaporin-4 antibodies and anti-myelin oligodendrocyte glycoprotein (MOG) antibodies, also, showed negative results. Bearing in mind his clinical course, the predominant involvement of the gray matter in the spinal cord, and negative extensive workup, AFM was considered as a diagnosis.
According to the CDC, AFM is characterized by rapid-onset flaccid weakness associated with distinct abnormalities of the spinal cord gray matter on MR imaging. A confirmed case of AFM should meet both clinical and radiological criteria. It is defined clinically as an acute-onset flaccid weakness of at least one limb that cannot be attributed to any other diagnosis. The radiological criteria stipulate the presence of a spinal cord lesion that mainly affects the gray matter and involves more than one segment. Also, spinal cord lesions due to neoplastic, vascular, or anatomic abnormalities must be excluded [1]. Our patient's clinical picture of acute flaccid paralysis, along with MRI findings of longitudinally extensive myelopathy that involves gray matter, is consistent with the CDC's criteria for a confirmed case of AFM.
AFM, in its current case definition, was first observed in 2012, but it came to public attention in the summer of 2014 after an outbreak of flaccid weakness cases in children in the United States. It was linked to Enterovirus D-68 (EV-D68), as the outbreak coincided with a rise in respiratory infection caused by EV-D68. Also, a mouse-model study showed that neonatal mice developed flaccid paralysis after they were infected by the virus. Nevertheless, the causative relationship has not been confirmed in humans [6-9]. Moreover, other viruses, such as enterovirus 71, West Nile virus, and Japanese encephalitis virus, are known to cause clinical manifestations and radiological features that are similar to AFM, which makes heterogeneity of causes for this clinical syndrome a possibility [3]. In the following years, similar cases were reported from other countries on different continents, including Turkey, Japan, Argentina, and Australia, and many of these cases have been linked to infection with EV-D68 [4,5]. The majority of patients with AFM were children or young adults, so the initial case definition restricted the age to less than 21 years. However, this restriction was removed in 2015 [2]. In addition to the typical presentation of flaccid weakness and gray matter involvement of the spinal cord, patients with AFM may have ophthalmoparesis, facial weakness, and evidence of dorsal pons and basal ganglia involvement in brain MRI [5,10]. The management of AFM is mainly supportive. Intravenous immunoglobulins, steroids, plasma exchange, and antiviral agents were used but without evidence of efficacy. Also, extensive rehabilitation and nerve transfer surgery may be useful in selected cases.
Nonetheless, prognosis is generally poor, and full recovery was reported in less than 10% of cases [2,11,12]. In Saudi Arabia and the other countries in the Arabian Peninsula, there are no reported cases of respiratory infection caused by EV-D68. However, EV-D68 was discovered in the sewage system and archived biological samples of children with respiratory symptoms in Israel [13,14]. In our patient, all the tests for viruses known to cause polio-like syndromes were negative, but many of the tests were sent after the acute phase of the illness had resolved, which decreased the tests' sensitivity.
In this case, we have many unanswered questions. However, answering them is possible only with vigilant reporting of suspicious cases and active surveillance of the disease and these viruses. This will reveal the actual incidence of this disease. Also, it may lead to confirming the disease's causes, which would help in developing disease prevention methods and improving the therapeutic care provided to these patients.
Conclusions
Acute flaccid myelitis is a rare emerging neurological disorder that leads to significant disability. Although it has been initially reported in the pediatric population, it can affect patients at any age. The disorder's pathogenesis is not fully understood but is possibly related to a viral infection. There is no proven curative treatment for the disease but early rehabilitation may help. In addition, increasing awareness about this entity in the medical community will shorten the diagnostic process and may help develop preventive measures in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1AFM Case Definitions 5 2023 2022 https://www.cdc.gov/acute-flaccid-myelitis/hcp/case-definitions.html
- 2Acute flaccid myelitis Phys Med Rehabil Clin N Am Ide W Melicosta M Trovato MK 4774913220213417500810.1016/j.pmr.2021.02.004 · doi ↗ · pubmed ↗
- 3Acute flaccid myelitis: cause, diagnosis, and management Lancet Murphy OC Messacar K Benson L 33434639720213335746910.1016/S 0140-6736(20)32723-9PMC 7909727 · doi ↗ · pubmed ↗
- 4Acute flaccid myelitis outbreak through 2016-2018: a multicenter experience from Turkey Eur J Paediatr Neurol Ünver O Türkdoğan D Güler S 1131203020213321888310.1016/j.ejpn.2020.10.011 · doi ↗ · pubmed ↗
- 5Serial MRI findings of acute flaccid myelitis during an outbreak of enterovirus D 68 infection in Japan Brain Dev Okumura A Mori H Fee Chong P 4434514120193059435310.1016/j.braindev.2018.12.001 · doi ↗ · pubmed ↗
- 6Acute flaccid myelitis of unknown etiology in California, 2012-2015 JAMA Van Haren K Ayscue P Waubant E 2663267131420152672002710.1001/jama.2015.17275 · doi ↗ · pubmed ↗
- 7Acute flaccid myelitis in the United States, August-December 2014: results of nationwide surveillance Clin Infect Dis Sejvar JJ Lopez AS Cortese MM 7377456320162731833210.1093/cid/ciw 372PMC 5709818 · doi ↗ · pubmed ↗
- 8A mouse model of paralytic myelitis caused by enterovirus D 68P Lo S Pathog Hixon AM Yu G Leser JS Yagi S Clarke P Chiu CY Tyler KL 013201710.1371/journal.ppat.1006199 PMC 532287528231269 · doi ↗ · pubmed ↗