Effects of Different Agents of the Lubrication of i-gel Airway on the Incidence of Postoperative Sore Throat: A Prospective Randomised Controlled Trial
Pavithra Balachandran, Ramamurthy Balaji, Dheepak Kumaran, Balasubramaniam Gayathri

TL;DR
This study compared different lubricants used with an airway device and found no difference in sore throat, but lignocaine jelly caused more hoarseness and swallowing discomfort.
Contribution
The study provides new clinical evidence on the effects of lubricants on postoperative outcomes with the i-gel airway.
Findings
Lubricants did not affect the incidence of postoperative sore throat.
Lignocaine jelly caused significantly more hoarseness and swallowing discomfort.
Airway insertion time and success rates were similar across all groups.
Abstract
Background and aim: The aim of this study is to compare the effect of different lubricating agents used with the i-gel® laryngeal mask airway on the incidence of postoperative sore throat. Materials and methods: After obtaining institutional ethics approval, this prospective trial was conducted on 150 patients who were scheduled for minor surgical procedures. The study population was placed in three groups of 50 each, after randomization with computer-generated random numbers, based on the lubricant used (Group LJ: with lignocaine jelly as the lubricant, Group WJ: with water-based jelly as a lubricant, Group NS: with 0.9% normal saline as a lubricant). The time taken to secure the airway (from insertion to the first end-tidal carbon dioxide (ETCO2) tracing and five-point auscultation) and the number of attempts were noted. During extubation, blood staining was noted. In the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
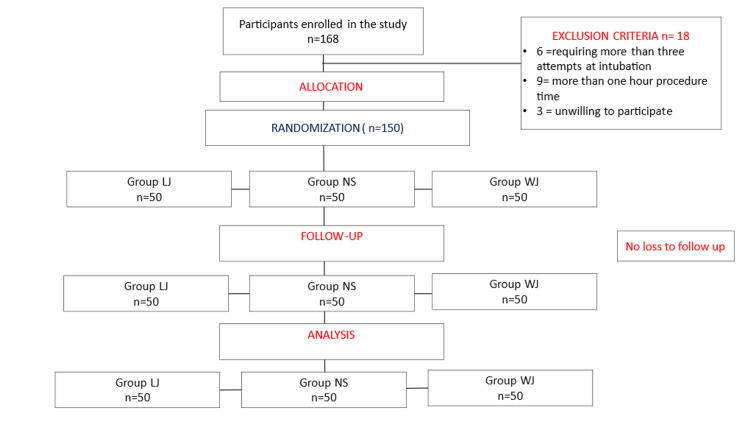 Figure 1
Figure 1| Demography | Group | p-value | ||||||
| Group LJ | Group NS | Group WJ | ||||||
| Count | Column N % | Count | Column N % | Count | Column N % | |||
| Sex | Male | 27 | 54.0% | 22 | 44.0% | 23 | 46.0% | 0.164* |
| Female | 23 | 46.0% | 28 | 56.0% | 27 | 54.0% | ||
| MPC | Class I | 21 | 42.0% | 20 | 40.0% | 22 | 44.0% | 0.921* |
| Class II | 29 | 58.0% | 30 | 60.0% | 28 | 56.0% | ||
| ASA PS | Class I | 24 | 48.0% | 25 | 50.0% | 25 | 50.0% | 0.974* |
| Class 2 | 26 | 52.0% | 25 | 50.0% | 25 | 50.0% | ||
| Size of LMA | Size 3 | 10 | 20.0% | 9 | 18.0% | 11 | 22.0% | 0.882* |
| Size 4 | 40 | 80.0% | 41 | 82.0% | 39 | 78.0% | ||
| Attempts at insertion | 1 | 41 | 82.0% | 43 | 86.0% | 43 | 86.0% | 0.853* |
| 2 | 8 | 16.0% | 7 | 14.0% | 6 | 12.0% | ||
| 3 | 1 | 2.0% | 0 | 0.0% | 1 | 2.0% | ||
| Group | F | p-value | ||||||
| Group LJ | Group NS | Group WJ | ||||||
| Mean | Standard Deviation | Mean | Standard Deviation | Mean | Standard Deviation | |||
| Age (years) | 42.54 | 12.64 | 44.06 | 12.42 | 43.20 | 10.50 | 0.174 | 0.840* |
| Height (cm) | 167.12 | 5.84 | 167.04 | 5.92 | 166.04 | 6.61 | 0.481 | 0.618* |
| Weight (Kg) | 65.82 | 6.52 | 66.62 | 6.11 | 64.60 | 6.53 | 1.267 | 0.284* |
| BMI | 23.50 | 1.06 | 23.83 | 0.98 | 23.38 | 1.16 | 2.338 | 0.100* |
| Duration of procedure (min) | 27.56 | 8.89 | 29.50 | 8.65 | 28.00 | 7.49 | 0.739 | 0.479* |
| Time taken for securing airway (sec) | 16.94 | 6.16 | 15.80 | 3.87 | 16.38 | 5.61 | 0.577 | 0.562* |
| Numerical Rating score at every four hour Interval for the first 24 hours | Average score | GROUPS | p-value | |||||
| GROUP LJ | GROUP NS | GROUP WJ | ||||||
| Count | Column N % | Count | Column N % | Count | Column N % | |||
| NRS 0 | 0 | 40 | 80.0% | 41 | 82.0% | 42 | 84.0% | 0.681* |
| 2 | 8 | 16.0% | 9 | 18.0% | 7 | 14.0% | ||
| 4 | 2 | 4.0% | 0 | 0.0% | 1 | 2.0% | ||
| NRS 4 | 0 | 45 | 90.0% | 45 | 90.0% | 44 | 88.0% | 0.664* |
| 2 | 4 | 8.0% | 5 | 10.0% | 6 | 12.0% | ||
| 4 | 1 | 2.0% | 0 | 0.0% | 0 | 0.0% | ||
| NRS 8 | 0 | 46 | 92.0% | 50 | 100.0% | 49 | 98.0% | 0.224* |
| 2 | 3 | 6.0% | 0 | 0.0% | 1 | 2.0% | ||
| 4 | 1 | 2.0% | 0 | 0.0% | 0 | 0.0% | ||
| NRS 12 | 0 | 48 | 96.0% | 50 | 100.0% | 50 | 100.0% | 0.132* |
| 2 | 2 | 4.0% | 0 | 0.0% | 0 | 0.0% | ||
| NRS 16 | 0 | 48 | 96.0% | 50 | 100.0% | 50 | 100.0% | 0.132* |
| 2 | 2 | 4.0% | 0 | 0.0% | 0 | 0.0% | ||
| NRS 20 | 0 | 49 | 98.0% | 50 | 100.0% | 50 | 100.0% | 0.365* |
| 2 | 1 | 2.0% | 0 | 0.0% | 0 | 0.0% | ||
| NRS 24 | 0 | 49 | 98.0% | 50 | 100.0% | 50 | 100.0% | 0.365* |
| 2 | 1 | 2.0% | 0 | 0.0% | 0 | 0.0% | ||
| Postoperative complications | Group | P-value | ||||||
| Group LJ | Group NS | Group WJ | ||||||
| Count | Column N % | Count | Column N % | Count | Column N % | |||
| Sore throat | Yes | 9 | 18.0% | 10 | 20.0% | 7 | 14.0% | 0.722* |
| No | 41 | 82.0% | 40 | 80.0% | 43 | 86.0% | ||
| Cough | Grade 0 | 44 | 88.0% | 39 | 78.0% | 41 | 82.0% | 0.413* |
| Grade 1 | 6 | 12.0% | 11 | 22.0% | 9 | 18.0% | ||
| Hoarseness | Grade 0 | 32 | 64.0% | 47 | 94.0% | 49 | 98.0% | <0.0001+ |
| Grade 1 | 14 | 28.0% | 3 | 6.0% | 1 | 2.0% | ||
| Grade 2 | 4 | 8.0% | 0 | 0.0% | 0 | 0.0% | ||
| Blood staining | No | 49 | 98.0% | 50 | 100.0% | 49 | 98.0% | 0.602* |
| Yes | 1 | 2.0% | 0 | 0.0% | 1 | 2.0% | ||
| Swallowing discomfort | No | 28 | 56.0% | 46 | 92.0% | 48 | 96.0% | <0.0001+ |
| Yes | 22 | 44.0% | 4 | 8.0% | 2 | 4.0% | ||
| PONV | No | 40 | 80.0% | 46 | 92.0% | 50 | 100.0% | 0.003+ |
| Yes | 10 | 20.0% | 4 | 8.0% | 0 | 0.0% | ||
| Water-based jelly | Normal saline | 2% lignocaine jelly | Saliva | |
| Lubricant manufacturer | Lubic (NEON)™ | NS (Fresenius Kabi)™ | LOX 2% (NEON)™ | 98.5 % water mucin enzymes, 1% organic substances, 0.5% inorganic substances |
| Composition | Glycerin propylene glycol gluconolactone, methylparaben propylparaben water-soluble gel base in purified water | Each 100 ml contains 154 mmol/litre sodium 154 mmol/litre chloride 308 mmol/l osmolality. | Lignocaine hydrochloride 2% w/v, Each ml 20 mg lignocaine, methylparaben 0.061% w/v, propyl paraben 0.027% w/v, water-soluble gel base | |
| pH | pH 4.5 | pH 5.5 | pH 6-7 | pH 6.02- 7.05 |
| Price | INR 5.6/g | INR 39.04 | INR 1.25/g |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAirway Management and Intubation Techniques · Tracheal and airway disorders · Voice and Speech Disorders
Introduction
Laryngeal mask airways are an important part of the airway management protocol, widely used in both emergency situations and the operating room [1]. Being a device made of synthetic material, most supraglottic airway devices require some form of lubrication for their adequate placement without causing injury to the oropharynx [2]. This is crucial, especially in the operating room, where the effects of general anaesthesia and gas flow through circuits affect the function of salivary glands [3]. The i-gel® is a second-generation laryngeal mask airway that is known for its design to aid in quicker insertion and ensure a better seal over the larynx [4]. The recommended lubricant for the i-gel is the K-Y® Jelly, which is a water-based lubricant. However, due to easy availability in the setting of an operating room, lignocaine jelly is used in its place in many institutions. Hence, we designed this study to compare the effect of different lubricating agents on the incidence of sore throat, a common postoperative event with laryngeal mask airways [5].
Materials and methods
This double-blind trial was registered with the Clinical Trial Registry of India (CTRI/2023/02/049480) and conducted over a six-month period at SRM Medical College and Hospital, from July 2023 to December 2023. After obtaining consent, 168 patients undergoing minor elective surgery requiring general anaesthesia at SRM Medical College and Hospital were initially enrolled in the study. The participants were aged between 18 and 70, belonged to both sexes, belonged to the American Society of Anesthesiologists Physical Status I and II and had Mallampati score grades 1 and 2. Patients with a history of sore throat within two weeks of the procedure, with known chronic obstructive airway disease or reactive airway diseases, with a diagnosis of gastro-oesophagal reflux disease or hiatus hernia, with an anticipated difficult airway with a restricted mouth opening (less than two fingers), a short neck and a body mass index of >30 kilograms per squared meter were excluded from the study.
Upon enrolment, the participants were allocated into three groups with 50 patients in each, through computer-generated random numbers based on the lubricant to be used: Group LJ with lignocaine jelly (LOX 2%: NEON ™), Group NS with normal saline (Fresenius Kabi™) and Group WJ with water-based jelly (Lubic: NEON™). Fasting guidelines and premedication were standardized for the three groups. On the day of the procedure, on arriving at the operating room, standard monitors were placed and preoxygenation was done. The opioid of choice was injection of fentanyl given at a dose of 2 micrograms per kilogram of body weight, while the induction agent of choice was injection propofol given at a dose of 2 milligrams per kilogram of body weight, while the induction agent of choice was injection propofol, given at a dose of 2 mg per kilogram of body weight, titrated to patient requirements. On attaining sufficient intubating conditions, an expert anaesthesiologist, with an experience of more than three years or who has had experience with more than 50 LMA insertions, placed the i-gel LMA coated immediately before insertion with the appropriate lubricating agent into the oropharynx of the patient based on the group to which they belonged. The parameter measured was the time to secure the airway that began with holding the i-gel LMA to its successful placement, confirmed by the first end-tidal carbon dioxide tracing on the monitor and five-point auscultation. A gaseous mixture of 2% weight by volume sevoflurane with 1 liter oxygen and 1 liter nitrous oxide was used for maintenance, and the patients were allowed spontaneous ventilation.
Patients requiring more than three attempts at insertion were considered failures, and standard general anaesthesia with endotracheal intubation was planned in the protocol in such a scenario. Patients undergoing procedures that lasted more than one hour were excluded from the study. At the end of the procedure, on removing the LMA, blood staining on the device surface was observed and made note of. The patients were then observed for a 24-hour period in the post-anesthetic care unit. A periodic re-evaluation was done every fourth hour, monitoring for sore throat measured through the numerical rating score (NRS), a scale of zero through 10 offered to the patient to mark. If the NRS was marked at more than six, injection fentanyl at one microgram per kilogram of body weight was administered. Any event of hoarseness of voice was measured on a scale of zero through three (0 - no hoarseness, 1 - minimal change in the quality of voice/affirmation on enquiry, 2 - moderate change in the quality of voice/patient complained on his own, 3 - gross change in quality of speech), and any complaints of cough were rated on a scale of zero through three (0 - no cough since surgery, 1 - minimal cough, 2 - moderate cough, 3 - severe cough [6]. Patients were also enquired and monitored for any event of swallowing discomfort and retching in the postoperative period.
Any other adverse events such as laryngospasm and bronchospasm were also noted. All the data were collected and compiled in a standard Excel sheet (MS Excel 2019, Microsoft Corporation, United States). Statistical analysis was done using the Chi-square and one-way ANOVA test using the IBM SPSS Statistics for Windows, Version 29.0 (released 2023, IBM Corp., Armonk, NY). Significance was taken when the p-value was <0.05
The consolidated standards of reporting trials are mentioned in Figure 1.
Consolidated Standards of Reporting Trialsn = population in each group, NS = normal saline , LJ = lignocaine jelly, WJ = water-based jelly
Results
In the present study, the patient characteristics and duration of surgery were comparable between the three groups (Tables 1, 2). In 127 patients, the i-gel was successfully placed at the first attempt (41 in Group LJ, 43 in Group NS and 43 in Group WJ), while 22 (eight in Group LJ, seven in Group NS and six in Group WJ ) required a second attempt for the successful placement of the i-gel. Two patients (one from the lignocaine jelly group and one from the water-based jelly group) required three attempts at intubation. This was not statistically significant. There was no incidence of insertion failure in all three groups (Table 1).
Table 1: Comparing qualitative patient characteristics amongst the three groups.LMA: laryngeal mask airway, ASA PS: American Society of Anesthesiologists Physical Status, n%: number percentage of the total population, MPC: Mallampati classification of airway.Group NS = group receiving normal saline as the lubricant, Group WJ = group receiving water-based jelly as lubricant, Group LJ = group receiving lignocaine jelly as the lubricant.Statistical analysis was done using the chi-squared test and p < 0.05 was considered significant. * - insignificant p-value. + - significant p-value
Table 2: Comparing the quantitative patient characteristics and time taken to insert and secure the airway amongst the three groups.BMI: body mass Index, CM: centimeter, KG: kilogram, Min: minutes, Sec: secondsGroup NS = group receiving normal saline as the lubricant, Group WJ = group receiving water-based jelly as a lubricant, Group LJ = group receiving lignocaine jelly as the lubricant, F = critical value.Statistical analysis was done using the one-way ANOVA test and p < 0.05 was considered significant. * - insignificant p-value. + - significant p-value
The time taken for securing the airway was not significantly different in the three groups: 16.94 ± 6.16 seconds vs. 15.80 ± 3.87 seconds vs. 16.38 ± 5.61 seconds in Group LJ, Group NS and Group WJ, respectively (p-value = 0.562) (Table 2).
Evaluation of sore throat in the postoperative period was done using the Numerical Rating Score. The patients were evaluated four hours once, till the first 24 hours. The incidence and severity of sore throat were similar between the groups and were statistically insignificant (p > 0.05). This shows that the three lubricants did not differ in terms of the incidence of sore throat (Table 3).
Table 3: Comparing the Numerical Rating Scores of patients between the three groups over a 24-hour period, at four-hour intervals.NRS: Numerical Rating ScoreGroup NS = group receiving normal saline as the lubricant, Group WJ = group receiving water-based jelly as the lubricant, Group LJ = group receiving lignocaine jelly as the lubricant.Statistical analysis was done using the chi-square test and p < 0.05 was considered significant * - insignificant p-value. + - significant p-valueNRS 0 signifies the baseline numerical rating score on the immediate removal of the i-gel device. NRS followed by the subsequent numbers suggests the hour at which the next score analysis was taken.
Other parameters monitored for were hoarseness of voice, swallowing discomfort and cough. The number of patients with no complaints of hoarseness of voice was 47 (94%) in Group NS, 49 (98%) in Group WJ and 32 (64%) patients in Group LJ. This was found to be significant (p < 0.05). In terms of severity, three patients from Group NS (6%), one patient from Group WJ (2%) and fourteen patients (28%) in Group LJ group had complaints of mild hoarseness of voice. Around four patients (8%) in Group LJ had moderate hoarseness of voice, while there were no such complaints in Groups NS and WJ. This difference in the severity of hoarseness was found to be statistically significant with a p-value < 0.05 (Table 4).
Table 4: Comparing the postoperative complications between the three groups.The values were recorded in the immediate postoperative period on removing the i-gel device.PONV: postoperative nausea and vomiting. Comparing the postoperative complications between the three groups: Group NS = group receiving normal saline as the lubricant, Group WJ = group receiving water-based jelly as the lubricant, Group LJ = group receiving lignocaine jelly as the lubricant.Statistical analysis was done using the chi-square test and p < 0.05 was considered significant * - insignificant p-value. + - significant p-value.Grades of hoarseness: three (0 – no hoarseness, 1 – minimal change in the quality of voice, 2 – moderate change in the quality of voice, 3 – gross change in the quality of speech). Grades of cough: (0 – no cough since surgery, 1 – minimal cough, 2 – moderate cough, 3 – severe cough)
On assessing swallowing in these patients, 22 (44%) patients in Group LJ complained of discomfort, while only four (8%) patients in Group NS and two (4%) patients in Group WJ had such complaints. This was significant with a p < 0.001 (Table 4).
On comparing any event of blood staining on the surface of the i-gel LMA at the end of procedure, one patient in Group LJ and one patient in Group WJ had trace staining during the LMA removal. This did not carry any statistical significance, i.e., p > 0.05 (Table 4).
Around six patients in Group LJ, 11 patients in Group NS and nine patients in Group WJ had complaints of cough in the postoperative period. This was insignificant with a p-value > 0.05 (Table 4).
Discussion
As the predecessor to all supraglottic airway devices, the laryngeal mask airway (LMA) is an important tool in the armamentarium of airway equipment, serving as a bridge between the endotracheal tubes and face masks [7]. While they offer several advantages over traditional endotracheal tubes, the morbidity associated with such LMA devices is seen in the form of minor complications such as sore throat, soft tissue injury during insertion, hoarseness and dysphagia. Lubricants are essential prior to placement of LMAs. This is because routine anticholinergic use and the high flow rates of anaesthetic gases tend to decrease salivary gland function [8,9]. Numerous LMAs have been developed over the years to enable ease of insertion while tackling the many disadvantages. The i-gel LMA® developed by Intersurgical™ is a second-generation true anatomic, pre-shaped, single-use device that exactly mirrors the laryngeal architecture. The i-gel is made of a medical-grade thermoplastic elastomer. The tacky nature of the material requires the i-gel LMA to be adequately lubricated before placing into the oral cavity. The recommended lubricant is the K-Y® water-based jelly. However, due to its limited availability, 2% lignocaine jelly is commonly used, given that it is invariably present in all operating rooms (Table 5).
Lignocaine jelly is a commonly used topical local anaesthetic. Keeping its anaesthetic properties in mind, this study was conducted to see if this would benefit in the postoperative period with decreased incidences of sore throat, hoarseness of voice, swallowing discomfort and cough [8,9]. However, we observed that the incidence of postoperative sore throat was similar between the three groups of lubricating agents. The results of our study were comparable to those of the study by Park et al., where normal saline was compared to lignocaine jelly and the incidence of sore throat did not vary [10]. Similarly, a study by Keller et al. also showed that the lubricants did not have an advantage over each other in producing sore throats [11].
We found that the incidence of hoarseness of voice and swallowing discomfort was significantly higher in the patients where lignocaine jelly was used as a lubricating agent than in patients in whom water-based jelly or normal saline was used. While aerosolized lignocaine is found to have more episodes of hoarseness of voice, the effect of lignocaine jelly has not been assessed clearly to date [12]. This study shows that patients receiving lignocaine jelly as a lubricant had mild hoarseness of voice in the immediate postoperative period, which did not require any intervention. The results of our study are similar to those of Sumathi et al., who suggest that better agents of lubrication, such as betamethasone jelly, might prove to have better benefits [13]. This suggests that lignocaine jelly, due to its bitter nature, density and anaesthetic properties, causes a numbing effect on the laryngopharynx that could account for the hoarseness of voice and swallowing discomfort [14,15].
Complaints of cough in the immediate post-surgery period were comparable amongst the three groups. This implies that even though there is a theoretical probability of the loss of the cough reflex on applying lignocaine jelly to the oropharynx, the effect was not potent enough to completely obscure the cough reflex [16,17].
The incidence of blood staining on the surface of the supraglottic airway device was similar between the three groups, which suggests that other factors like the attempts at insertion or an unanticipated difficult airway could contribute to this particular side effect [18,19].
Our study shows that lignocaine jelly does not offer any advantage as a lubricating agent over the recommended water-based jelly. Our study shows similar results to a study by Doukumo et al., who studied the effect of different lubricating agents on endotracheal intubation [20].
One patient in Group WJ and two patients in Group NS had an episode of vomiting. Injection ondansetron 4 milligrams was given after re-assuring the patients.
Limitations
Although the degree of hoarseness of voice and presence of swallowing discomfort were evaluated in the immediate postoperative period by us, we did not follow through the entire 24 hours to check its resolution. Furthermore, the postoperative changes in the pharyngeal mucosa through endoscopic view could not be assessed by us. This can be a prospect in future studies.
Conclusions
We conclude that the three lubricating agents, namely, lignocaine jelly, water-based jelly and normal saline, did not have an advantage over one another in reducing the incidence of postoperative sorethroat. On screening these patients for other side effects , we noticed higher rates of hoarseness of voice and swallowing discomfort with patients who received lignocaine jelly as the lubricant of choice . Further studies with a larger sample size can aim at understanding the effect that different agents have on the oral mucosa , especially at finding the most suitable agent for lubrication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Supraglottic airway devices: current and future uses Br J Hosp Med (Lond) Kwanten LE Madhivathanan P 31357920182931504610.12968/hmed.2018.79.1.31 · doi ↗ · pubmed ↗
- 2Supraglottic airway devices: an overview Med J Cairo Univ El Naggar A Farid D Nasr Y Alarga E 3273338820201
- 3Postoperative sore throat: a systematic review Anaesthesia El-Boghdadly K Bailey CR Wiles MD 7067177120162715898910.1111/anae.13438 · doi ↗ · pubmed ↗
- 4I-Gel and LMA classic in the hands of novice: a comparative study Asian J Med Sci Bhattacharjee I Sarkar S Bhattacharyya C Das D Mandal M 10311012021
- 5A prospective study on the incidence of sore throat after use of laryngeal mask airway during general anesthesia Ann Med Surg (Lond) Farazmehr K Aryafar M Gholami F Dehghanmanshadi G Hosseini SS 1025956820213440112010.1016/j.amsu.2021.102595 PMC 8353405 · doi ↗ · pubmed ↗
- 6Postoperative sore throat, hoarseness and cough following use of two different supraglottic airway devices: a comparison of Baska mask versus i-gel J Clin Res Pain Anaesthesia Rajan S 18001212019 https://www.researchgate.net/publication/338216450_Citation_Sunil_Rajan_et_al_Postoperative_Sore_Throat_Hoarseness_and_Cough_Following_Use_of_Two_Different_Supraglottic_Airway_Devices_A_Comparison_of_Baska_Mask_versus_I-_Postoperative_Sore_Throat_Hoar
- 7Supraglottic airway devices: a review in a new era of airway management J Anesth Clin Res Almeida G 72016
- 8Lignocaine gel and the laryngeal mask airway Anaesthesia Edwards ND 74674750199510.1111/j.1365-2044.1995.tb 06120.x 7645722 · doi ↗ · pubmed ↗