Case Report: Modified endoscopic hook for extracting magnetic esophageal foreign bodies in a rural area
Hamsu Kadriyan, Ika Primayanti, Syamsidar Syamsidar, Lalu Fauzan Fakhrussiam, Moh Fahrur Rozi, Hijrinelly Hijrinelly, Dian Adi Syahputra, hamsu kadriyan, Mingyan Cai, hamsu kadriyan

TL;DR
A modified endoscopic hook successfully extracted a magnetic foreign body from a child's esophagus in a rural area.
Contribution
A modified hook attachment for endoscopes is proposed for extracting magnetic foreign bodies in resource-limited settings.
Findings
A magnetic foreign body was successfully extracted from a three-year-old boy's esophagus using a modified hook.
The modified hook is a practical innovation for rural areas with limited medical resources.
The method could be scaled industrially for broader use in otolaryngology.
Abstract
Foreign bodies (FB) in the aerodigestive tract are common, especially in children. The type of foreign body in the esophagus can vary and include magnets. A magnet that lodges in the esophagus should be extracted within 24 hours to prevent complications due to associated chemical reactions. In rural areas, there are several limitations to extracting FBs from the esophagus. We report a case of a magnetic FB that lodged in the esophagus of a three-year-old boy. The extraction was successfully done by esophagoscopy with the modification of a hook that was attached to the endoscope. This innovation may help otolaryngologists all over the world, especially in rural areas. In the future, this innovation could be produced on an industrial scale.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
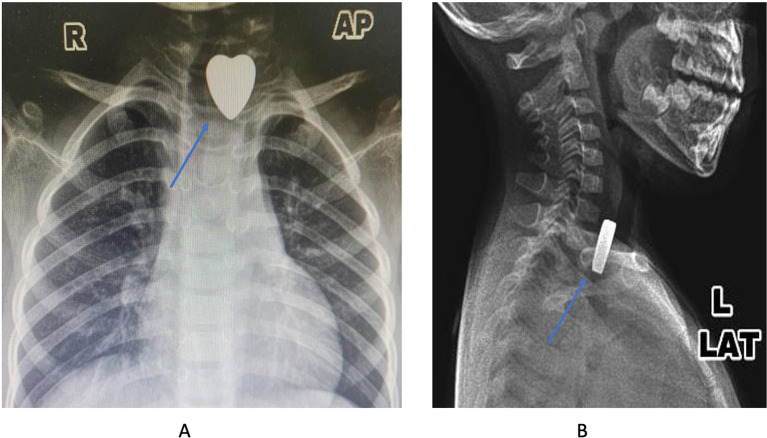 Figure 1
Figure 1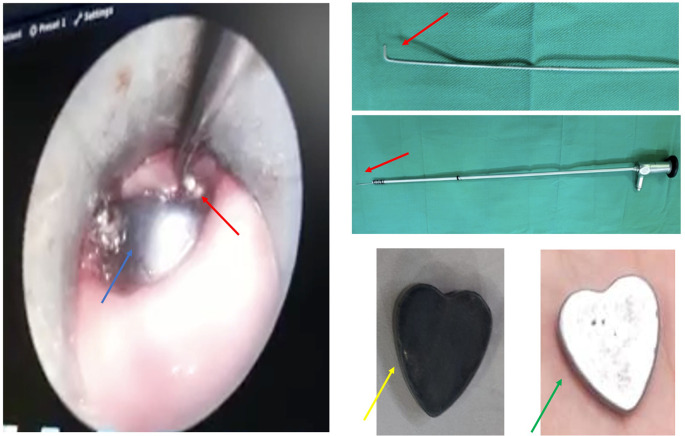 Figure 2
Figure 2- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Esophageal and GI Pathology · Airway Management and Intubation Techniques
Introduction
Although a warning regarding choking risk has been included on every toy by the factory, ^ 1 ^ cases of foreign body (FB) in the upper aerodigestive tract remain frequently found in the clinical setting. Several types of FBs can be found in the upper aerodigestive tract, including coins, magnets, batteries, pins, and organic substances such as peanuts, meat, among others. ^ 2 ^ ^–^ ^ 4 ^ The effect of FBs in the aerodigestive tract varies, depending on its location. If the FB is lodged in the esophagus, it will cause dysphagia, while in the bronchus it may cause airway obstruction and lead to mortality. ^ 2 ^ ^,^ ^ 3 ^
The part of a toy such as a magnet can usually found in children and may cause perforation or fistula on the esophagus. This complication occurs because of the effect of the chemical reaction between the magnet with the esophagus tissue. Therefore, a magnet FB in the esophagus should be extracted within 24 hours of the finding. ^ 3 ^ ^,^ ^ 4 ^
The extraction of FBs from the esophagus may be challenging, especially in a rural area with limited equipment. An endoscope or esophagoscope, and a forceps or extractor are not complete or do not fit with the type or shape of the FBs. Therefore, in rural areas, the physician should try to do their best to help the patient with those limitations. In this report, the authors would like to share the modification of the hook that is attached to the rigid endoscope. This modification successfully extracted a big and thick heart-shaped magnet in the esophagus.
Case presentation
A three-year-old boy was referred from the primary hospital with FBs lodged in the esophagus 1 hour prior to the hospitalization. He accidentally ingested the magnet toys while playing with his sister. After the incident, the boy was crying and his sister told their mother that her brother had ingested the toy part. His sister showed the shape of FB that was ingested to their mother. Therefore, the boy was then brought to the hospital to see whether the FB was lodged somewhere or not. There was no sign of coughing or dyspnea in this patient.
An x-ray examination was done to know the location of the FBs in the upper aerodigestive tract. The result showed the radiopaque metallic object with a heart shape was lodged in the upper esophagus ( Figure 1A and B). After the diagnosis was established, the patient was scheduled for an esophagoscopy to extract the FB under general anesthesia.
The X-ray images showed the metallic density with the heart shape (blue arrow) (A: anterior-posterior projection; B: lateral projection).
During the esophagoscopy, several forceps and baskets were tried to extract the FB, however, the FB was moving down to the middle part. After several attempts, the authors then tried to modify the endoscope by placing the additional hook on the tip of the rigid scope ( Figure 2, red arrow). Finally, the FB could be extracted without any complications, however, the color of the FB has changed ( Figure 2, yellow arrow) from its original color ( Figure 2, green arrow).
The FB extraction under endoscope view (blue arrow: the FB; red arrow: the hook; green arrow: original magnet).
Follow-up after surgery was done after two (2) days, and no complications occurred. The patient was then released from the ward. A week after the surgery, the patient came to the outpatient clinic. No difficulties in swallowing were found, and the patient could eat all kinds of food.
Discussion
The constraints in managing certain cases in rural areas may be unexpected; therefore, some physicians may refer the patient to a bigger/higher hospital if they encounter difficulties. ^ 5 ^ However, in some archipelago countries, the transportation between the islands may become a problem. Some small islands may only have boating infrastructure; on the other hand, larger islands may have a more complete transportation infrastructure. In some cases, the patient or their family may not agree to be referred to another hospital on other islands. Another patient may delay the treatment time for another reason, for instance, costs considerations and low awareness of disease symptoms. ^ 6 ^ ^,^ ^ 7 ^ Therefore, the physician should apply their best competencies to manage the cases. One of the general constraints faced in rural areas is inadequate equipment. The other constraint is manpower. ^ 7 ^
The modification of this hook was inspired by the cerumen hook that is routinely used by the otolaryngologist to remove the hard wax or FB in the ear canal. ^ 8 ^ Therefore, the principle is alike to a cerumen hook. To make it visible, the hook was attached to the rigid scope. Therefore, the FB extraction could be done safely with direct vision. The other concern is the hook should be in a safe mode for the esophagus, with non-sharp tip for example.
The extraction itself started with the insertion of a rigid esophagoscope into the esophagus until it was close to the FB location. Then, the hook attached to the scope was inserted through the lumen of the esophagoscope. The hook insertion should be done smoothly in a similar direction to the FB position and esophagus wall ( Figure 2) to prevent a wound that may provoke a perforation. After passing the edge of the FB, the hook direction was then rotated to the body of FB and extracted slowly. If it does not work on the first attempt, the procedure could be repeated until the FB is successfully removed.
The application of a hook is suitable for a quadrangle- or triangle-shape FB with a certain thickness (thicker than a coin). According to a previous publication, a hook for extracting FB in the esophagus is not available. ^ 4 ^ Therefore, this modification is the first innovation of the kind published in a journal. Hopefully, this innovation could help otolaryngologists globally, especially in rural areas. This innovation may also be used as an inspiration to modify incomplete equipment in a rural area. However, advanced research should be done to prove it’s efficacy. Therefore, in the future, this modification could be produced on an industrial scale.
Conclusions
The modified endoscopic hook is an innovation that is suitable and safe for extracting quadrangle or triangle FB shapes in the esophagus with a certain thickness.
Consent of the patient’s parents
The written consent for using the images and publishing this case report has been given by the parent of the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Child Safety Central: Consumer Product Safety Commission: Child Safety Protection Act Fact Sheet. 2006. Reference Source Reference Source
- 2Gezer HO Ezer SS Temiz A : Ingested foreign bodies in children: Do they really pass spontaneously from the gastrointestinal tract? A single-centre experience with 1000 cases. Ulus. Travma Acil Cerrahi Derg. 2020;26:247–254. 10.14744/tjtes.2019.40350 32185763 · doi ↗ · pubmed ↗
- 3Altokhais TI Al-Saleem A Gado A : Esophageal foreign bodies in children: Emphasis on complicated cases. Asian J. Surg. 2017;40:362–366. 10.1016/j.asjsur.2015.12.008 26922630 · doi ↗ · pubmed ↗
- 4Magalhães-Costa P Carvalho L Rodrigues JP : Endoscopic Management of Foreign Bodies in the Upper Gastrointestinal Tract: An Evidence-Based Review Article. GE Port. J. Gastroenterol. 2016;23(3):142–152. 10.1016/j.jpge.2015.09.002 28868450 PMC 5580008 · doi ↗ · pubmed ↗
- 5Kadriyan H Sulaksana MA Yudhanto D : Subcutaneous hemangioma on nasal dorsum: A case report. J. Med. Case Rep. 2020;14:1–6. 10.1186/s 13256-020-02443-4 32787966 PMC 7425069 · doi ↗ · pubmed ↗
- 6Kadriyan H Endriani E Andiwijaya FR : Upper airway obstruction due to bilateral laryngeal polyp: A challenge of treatment in rural area. Crit. Care Shock. 2021;2021(July):212–217.
- 7Soepardi EA : Problem in managing foreign bodies in upper aerodigestive tract. Med. J. Indones. 2002;11(1):15–18. 10.13181/mji.v 11i 1.50 · doi ↗
- 8Watkins C Mc Calla CD : Foreign bodies of the head and neck. Pediatr. Emerg. Med. Rep. 2016;21(7):1–15.