A case of adnexal cutaneous leishmaniasis in Washington DC
Sinan Akosman, Heeyah Song, Paul Sheils, Tamer Mansour, Keith J. Wroblewski, Lamise Rajjoub

TL;DR
A 68-year-old woman in Washington DC was diagnosed with a rare case of cutaneous leishmaniasis caused by Leishmania aethiopica after initial treatments failed.
Contribution
This paper reports a rare non-endemic case of Leishmania aethiopica in the US, emphasizing the need for broad differential diagnosis in urban settings.
Findings
The patient's symptoms were initially misdiagnosed as viral or autoimmune, leading to ineffective treatments.
A delayed punch biopsy confirmed leishmaniasis, and oral miltefosine resolved the symptoms completely.
The case highlights the importance of considering non-endemic diseases in patients with travel histories.
Abstract
To report a rare non-endemic case of Leishmania aethiopica in Washington DC. A 68-year-old female presented for a routine examination with a complaint of right upper eyelid lesions for the past 5 months. On examination, a cluster of elevated and erythematous lesions extending from the medial canthus to the brow area of the right eye were seen. Initial treatment with Valtrex based on a suspected viral etiology failed. Although a biopsy was recommended at this time, the patient declined, and subsequent workup included nasolacrimal duct irrigation, blood work to rule out autoimmune etiology, a course of doxycycline, and an MRI, which yielded no improvement. Upon progression of the lesions into persistent plaques on the eyelids, a punch biopsy was performed, confirming leishmaniasis. The patient was then started on a 28-day course of oral miltefosine which led to complete resolution of her…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1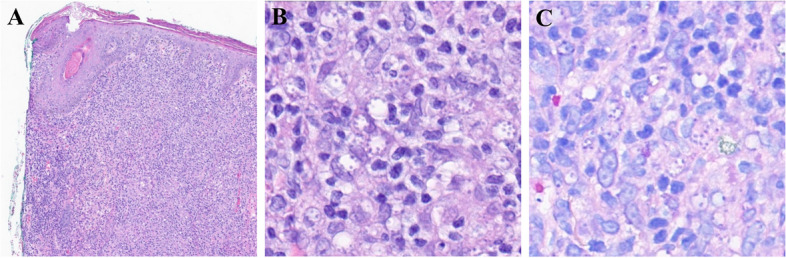 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsResearch on Leishmaniasis Studies · Bartonella species infections research · Syphilis Diagnosis and Treatment
Introduction
Leishmaniasis is an infectious disease caused by the protozoan parasites of the Leishmania genus. Leishmania are transmitted by the bite of infected female phlebotomine sandflies, and known reservoirs of this parasite can be humans as well as animals [1]. The World Health Organization (WHO) estimates between 700,000 to 1,000,000 new cases of leishmaniasis worldwide annually, with several endemic regions in the Americas, Mediterranean, Europe, and South-East Asia [2].
The clinical manifestations of leishmaniasis are largely categorized into cutaneous leishmaniasis (CL), mucocutaneous leishmaniasis, or visceral leishmaniasis. CL is the most common form of leishmaniasis and typically presents with skin lesions or ulcers on extremities. Facial lesions are typical in CL, yet eyelid and periorbital involvement is relatively rare, accounting for only about 2% of all CL cases [1, 3, 4].
Diagnosing adnexal leishmaniasis poses a challenge due to its similarity to more common lesions, such as preseptal cellulitis, orbital pseudotumor, sarcoidosis, ophthalmic zoster, allergic reactions, edema due to hypoproteinemia, and thyroid-associated ophthalmopathy [4–6]. In this report, we describe the clinical features, diagnosis, and treatment of a patient with CL presenting with right upper eyelid lesions.
Case report
A 68-year-old female presented for a routine examination with a complaint of right upper eyelid lesions for the past 5 months. The patient was of Ethiopian origin and reported recent travel to Ethiopia within the last year. On examination, a cluster of elevated lesions measuring 7 mm × 13 mm near the medial canthus of the right eye were seen extending up to the brow area (Fig. 1). The lesions were erythematous with associated soft tissue edema and non-tender to the touch. The lesions were only limited to the right eye. Suspecting a viral or shingles-related cause, a two-week course of Valtrex was prescribed, but it yielded no improvement. In a subsequent evaluation two months later, the lesions worsened with increased erythema, size, and edema, infiltrating deeper in the periocular area. Although biopsy was offered multiple times, the patient repeatedly declined despite multiple counseling attempts. Subsequently the patient was then referred to oculoplastic clinic for further evaluation. Nasolacrimal duct was irrigated to rule out any lacrimal involvement which was negative. Patient was subsequently started on a course of doxycycline and extensive blood work including angiotensin converting enzyme (ACE), immunoglobulin G4 (IgG4), C1 esterase, rheumatoid factor (RF) and antineutrophil cytoplasmic antibodies (ANCA) was done to rule out any autoimmune etiology without much yield. Concerned for possible neoplastic etiology, the MRI face/orbit was completed, which showed soft tissue swelling in the right preseptal and pre-maxillary region extending across the nasion with enhancement of levator palpebrae muscle, right lacrimal gland and nasolacrimal duct. The MRI findings were highly suggestive of inflammatory or infectious etiology. Unfortunately, the lesions persisted. Differentials considered at this juncture included sarcoid/orbital and pseudotumor, with cellulitis being less likely.Fig. 1. Shows an external photograph of her right eye which demonstrates erythematous, infiltrative plaques that extend across the medial canthal region up toward the brow
The patient was then referred to dermatology. During the evaluation, persistent plaques on the right eyelids now involving the bridge of the nose were seen. At this point, patient agreed to a punch biopsy, which showed intracytoplasmic infection most consistent with leishmaniasis. Subsequently, the patient was referred to the National Institutes of Health (NIH). A second biopsy of the right periorbital lesion was done at NIH which was PCR positive for Leishmenia aethiopica. Patient was offered IV amphotericin and a 28-day course of oral miltefosine; our patient elected to proceed with miltefosine, resulting in complete resolution of her lesions without any reported adverse events.
Pathology
The skin biopsy from the right root of the nose demonstrated a dense pan-dermal infiltrate composed of primarily lymphocytes and histiocytes with scattered other inflammatory cells on low magnification (Fig. 2, panel A).Fig. 2. Histopathologic features consistent with intracellular infection. A Dense pan-dermal infiltrate (hematoxylin–eosin staining, original magnification × 4); B Parasitized histiocytes with staining of Leishmania amastigotes (PAS, original magnification × 40); and C Parasitized histiocytes with staining of Leishmania amastigotes (Giemsa, original magnification × 40)
On PAS (Fig. 2, panel B) and Giemsa (Fig. 2, panel C) special staining, within the lymphocytes, vacuoles are identified with small organisms arranged around the periphery of the vacuoles. No gelatinous capsule is identified. These organisms were not visualized on GMS special staining.
Taken together, the findings are consistent with an intracellular infection, such as leishmaniasis or histoplasmosis, among others, in the correct clinical context. Correlation with serologic study and deep tissue culture, if indicated, is recommended. The case was discussed with dermatopathology, who agreed with the diagnosis as above.
Discussion
This case highlights the growing challenge and significance of considering leishmaniasis in physicians' diagnostic considerations in non-endemic regions, including the United States. In the recent years, CL has a rising global prevalence due to increasing migration from endemic areas, which requires healthcare professionals around the world to be able to effectively recognize leishmaniasis and its complications [7].
In our case, the unusual location of the lesions led to a delay in diagnosis and management. Periorbital lesions in cutaneous leishmaniasis are thought to be rare due to the movement of the eyelids which deters the bite of the fly vector [8, 9]. In a study of over 1,700 CL lesions of patients in Turkey, only 1.93% of lesions were located on the eyelid and the periorbital region [3]. Additionally, adnexal Leishmaniasis commonly presents as a chalazion-like lesion which can often bear resemblance to a multitude of other cutaneous lesions such as those from recurrent chalazion, ulcerative basal cell carcinoma, granulomatous blepharitis, and infected infundibular cysts [3, 10–12].
The diagnosis of cutaneous leishmaniasis is classically made with a tissue biopsy, which allows for the identification of the microorganisms through staining or culture [13]. In recent years, PCR has also emerged as a critical tool in diagnosis, offering the option for molecular analysis of specimens, which can be pivotal in guiding treatment strategies [14]. The effectiveness of these diagnostic methods was particularly significant in this case, as they led to the identification of the causative agent as L. aethiopica.
L. aethiopica, one of the most understudied species of Leishmania, is the predominant strain endemic to Ethiopia [15], where up to 65% of the population in affected areas is reported to have either an active or past infection of leishmaniasis [16]. The identification of this species was crucial, as L. aethiopica is known for its slower healing time and reduced sensitivity to conventional treatment regimens [17]. This knowledge underscores the importance of accurate diagnosis and species identification in the effective management of leishmaniasis cases.
In selecting treatment regimens for Leishmaniasis, it's crucial to consider the specific Leishmania species, patient toxicity risk, and local medication availability. Historically, pentavalent antimonials were the standard first-line treatment. However, due to rising resistance concerns, the WHO has updated its standard of care to recommend liposomal amphotericin B [18]. Recently, systemic oral miltefosine has emerged as an alternative treatment. It is often better tolerated than amphotericin B, which is associated with renal insufficiency and other serious side effects. Initially developed for cancer therapy, miltefosine has since received Food and Drug Administration (FDA) approval for treating three specific species of New World leishmaniasis and has been shown to be effective against L. aethiopica in several small clinical trials [19–21]. In this case, our patient's successful treatment involved a 28-day course of miltefosine.
Lastly, this case highlights the diagnostic value of a prompt skin biopsy, which would have undoubtedly led to a sooner diagnosis and treatment for the patient, as well as avoided unnecessary laboratory tests, diagnostic images, and healthcare expenses. Patient education and clear communication of risks and benefits of such procedures must be effectively achieved in order to achieve optimal outcome for all parties.