Withdrawal Dyskinesia Associated With Aripiprazole in a Child: A Case Report
Haruo Nishijima, Miyuki Nishijima, Chikyo Oyama, Masahiko Tomiyama

TL;DR
A child with autism developed movement disorders after stopping aripiprazole, showing the need for caution when adjusting antipsychotic medications in children.
Contribution
Reports a rare case of withdrawal dyskinesia in a child after aripiprazole discontinuation, highlighting under-recognized risks in pediatric patients.
Findings
Oral dyskinesia occurred after aripiprazole discontinuation and reappeared after dose reduction.
Dyskinesia resolved upon reinitiation of aripiprazole and gradually disappeared over months.
Withdrawal dyskinesia may be underreported in children and could impact quality of life.
Abstract
Atypical antipsychotics are considered to be better tolerated than typical antipsychotics; however, the risk of drug-induced movement disorders needs to be considered. Aripiprazole, a dopamine partial agonist, is one of the most frequently used atypical antipsychotics in children. In this report, we describe withdrawal dyskinesia after aripiprazole discontinuation in a child with autism spectrum disorder. The patient presented with oral dyskinesia after discontinuation of aripiprazole when he was 13 years old. Dyskinetic movements disappeared after reinitiation of aripiprazole. He developed oral dyskinesia again after a reduction of the aripiprazole dose when he was 14 years old. Dyskinesia gradually disappeared within a few months. Withdrawal dyskinesia associated with aripiprazole has been rarely reported in children. Moreover, there is no large study on the prevalence of dyskinesia…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
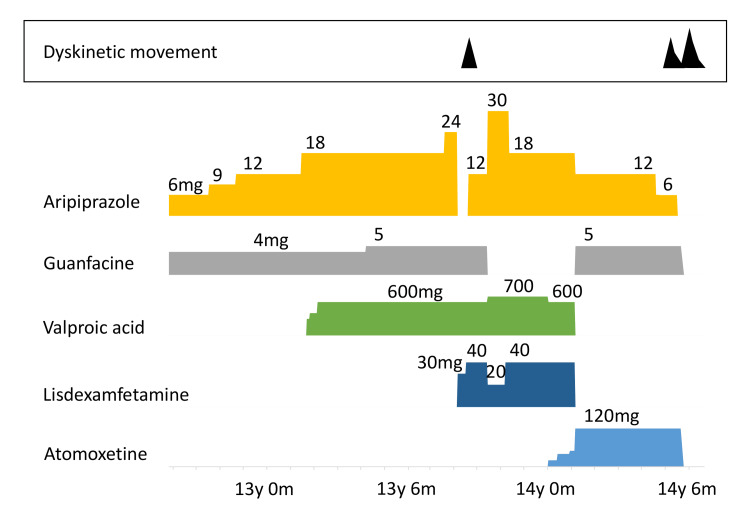 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutism Spectrum Disorder Research · Attention Deficit Hyperactivity Disorder · Pharmaceutical studies and practices
Introduction
In recent years, the use of second- or third-generation (atypical) antipsychotics has increased, compared with that of first-generation (typical) antipsychotics [1]. Atypical antipsychotics, with a lower rate of drug-induced movement disorders such as parkinsonism and dyskinesia, are better tolerated. However, the risk of such disabling side effects exists. The prevalence of tardive dyskinesia in patients taking atypical antipsychotics is approximately 20% [2]. Moreover, apart from adults, antipsychotics are widely prescribed for children and adolescents. Haloperidol, a first-generation antipsychotic, reportedly induced dyskinesia in 40 of 118 (33.9%) children with autism [3]. Conversely, it is unclear how often dyskinesia develops in children undergoing atypical antipsychotic treatment. Aripiprazole, a partial dopamine agonist [4], is one of the most frequently used atypical antipsychotics in children with autism [5]. This report describes the withdrawal dyskinesia after aripiprazole discontinuation in a child with autism spectrum disorder (ASD).
Case presentation
A boy, aged 11 years and 11 months, diagnosed with ASD and attention-deficit hyperactivity disorder (ADHD) by his pediatrician was referred to our hospital. His irritability and roughness were causing difficulties at school. Computed tomography of the brain and blood tests did not reveal anything significant. He did not exhibit abnormal involuntary movements.
At the age of 13 years and eight months, he was treated with aripiprazole (24 mg/d, in two divided doses of 12 mg), guanfacine (5 mg/d, once a day), and valproic acid (600 mg/d, in two divided doses). Aripiprazole had been gradually increased to this dose with the consent of his parents, because hyperactivity, impulsivity, hyperlogia, and stalking behavior were causing several troubles in his school life. Subsequently, aripiprazole was abruptly discontinued as it did not address his symptoms effectively, and lisdexamfetamine (30 mg/d, once a day) was administered instead. Four days after aripiprazole discontinuation, he presented with abnormal orolingual movements, that is vacuous chewing, tongue writhing, and lip licking (Figure 1). The total score of the abnormal involuntary movement scale score (AIMS) (items 1-7, score range 0-28) [6] was 5. After several days, he developed truncal choreic movement (AIMS: 8). His irritability worsened and daily activities became difficult. Therefore, treatment with aripiprazole (12 mg/d) was resumed. We chose a dose lower than the initial one because aripiprazole was re-started only as a diagnostic treatment for involuntary movements. Abnormal movements of the jaw, lip, tongue, and trunk reduced and then disappeared within two weeks (Figure 1).
Clinical course and drug treatment during the first and second episodes of withdrawal dyskinesia associated with aripiprazole discontinuationWhen the patient was 13 years and eight months old, aripiprazole was discontinued and lisdexamfetamine was administered instead, then he presented with dyskinesia. Treatment with aripiprazole was resumed and the dyskinesia disappeared within two weeks. When he was 14 years and five months old, the aripiprazole dose was decreased, and then he developed dyskinesia again. When aripiprazole treatment was discontinued, the dyskinesia significantly worsened. Then atomoxetine and guanfacine were also discontinued, and the dyskinetic movement gradually disappeared within a month.y: years; m: months
At the age of 14 years and five months, he was receiving aripiprazole (12 mg/d), guanfacine (5 mg/d), and atomoxetine (120 mg/d, in two divided doses). Subsequently, the aripiprazole dose was decreased to 6 mg/d because of frequent wandering, which was considered akathisia. Seven days after the decrement, he developed orolingual dyskinesia again (Figure 1) (AIMS: 4). The dyskinesia gradually subsided within a few weeks (AIMS: 2). Subsequently, aripiprazole treatment was discontinued. Four days after discontinuation, oral dyskinetic movements worsened significantly. Apart from orolingual movements, wide opening of eyes, facial grimacing, and lower limb choreic movements also appeared on the following days (AIMS: 11). His dyskinesia improved on the day he did not take atomoxetine, whereas it worsened after taking atomoxetine. Therefore, atomoxetine and guanfacine were discontinued. The dyskinetic movement gradually disappeared within a month (AIMS: 0) (Figure 1).
The patient is currently 15 years and 10 months old, does not take any antipsychotics, and has no abnormal involuntary movements.
Discussion
Antipsychotics-induced dyskinesia is divided into three types: tardive, covert, and withdrawal dyskinesia [7,8]. Tardive dyskinesia occurs during treatment with dopamine-blocking agents. Covert dyskinesia is disguised as dyskinesia during active antipsychotic treatment; it appears after dose reduction or discontinuation, does not remit spontaneously, and is usually permanent. Withdrawal dyskinesia initially occurs after the discontinuation of an antipsychotic agent and is self-limiting, with complete remission expected. This is considered a result of a temporary hyperdopaminergic state in the basal ganglia caused by the discontinuation of dopamine-blocking agents [7].
The majority of antipsychotics-induced dyskinesia in children involve withdrawal dyskinesia [3,9]. Only a few studies have reported dyskinesia after aripiprazole discontinuation in adults [8,10]. In children and adolescents, we could find only one case of dyskinesia associated with aripiprazole discontinuation involving a 17-year-old White male with bipolar disorder [11], which might be covert dyskinesia because the dyskinesia persisted at the last reported follow-up. The present case is perhaps the first report of the apparent withdrawal dyskinesia associated with aripiprazole discontinuation in a child. However, no large-scale studies have been conducted on the prevalence of dyskinesia associated with aripiprazole discontinuation in adults or children. Additionally, relevant cases might have been unreported, pretermitted, or regarded as akathisia or symptoms of ADHD. Thus, the prevalence of withdrawal dyskinesia associated with aripiprazole, especially in children, may be higher than previously estimated.
Our patient presented two episodes of withdrawal dyskinesia; in the first episode, aripiprazole was abruptly discontinued from a high dose, whereas in the second episode, aripiprazole was tapered. In the previous reports of dyskinesia associated with aripiprazole discontinuation, the aripiprazole dose was tapered in all the cases [8,10,11]. Moseley et al. reported an adult case with tapering of the dose from 15 mg/day over four weeks [8]. Urbano et al. reported two adult cases, in both of which the aripiprazole dose was gradually decreased from 5 mg/day to zero [10]. Even in Kafantaris et al.’s case of a 17-year-old boy, aripiprazole was tapered [11]. Thus, dyskinesia associated with aripiprazole discontinuation may occur not only with abrupt discontinuation after a high dose but also despite a cautious tapering of the dose.
The mechanisms underlying the withdrawal dyskinesia following aripiprazole discontinuation are unclear. It may be explained by the dopaminergic hypersensitivity hypothesis proposed for haloperidol-induced tardive dyskinesia [12]. In the current case, chronic administration of aripiprazole, a partial dopamine agonist, may have induced brain dopamine receptor hypersensitivity. When aripiprazole was discontinued, the antagonistic effect on dopamine receptors disappeared, and excessive dopaminergic stimulation may have induced hyperkinetic movement disorders. Moreover, drugs that enhance the dopaminergic or noradrenergic effects may enhance dyskinesia. In this case, lisdexamfetamine, atomoxetine, and guanfacine were co-administered when aripiprazole was discontinued. Lisdexamfetamine blocks dopamine and noradrenaline transporters and increases their levels in the brain [13]. Atomoxetine blocks noradrenaline transporters and increases noradrenaline levels in the brain [14]. Additionally, in the prefrontal cortex, noradrenaline transporters take up noradrenaline and dopamine [15]. In a basic animal study, atomoxetine increased dopamine levels in the prefrontal cortex [16]. Guanfacine also facilitates noradrenergic neural transmission [17]. These drugs may have worsened the dyskinesia in this case. This is supported by the fact that atomoxetine appeared to enhance dyskinetic movement in the second episode. Moreover, covert dyskinesia associated with aripiprazole discontinuation was reported in patients [8] receiving serotonin and noradrenaline reuptake inhibitors duloxetine and venlafaxine [18,19], or the dopamine and noradrenaline reuptake inhibitor methylphenidate [20]. These drugs may also have the potential to exacerbate dyskinesia.
Conclusions
Although withdrawal dyskinesia disappears within a certain period, children and adolescents affected by it may refuse to go to school or interact with other children, risking irreversible effects. Thus, physicians must monitor for dyskinesia occurrence while changing, reducing, or discontinuing antipsychotics in children. Careful drug adjustment is imperative to avoid severe influences on patients’ lives.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tardive dyskinesia: therapeutic options for an increasingly common disorder Neurotherapeutics Cloud LJ Zutshi D Factor SA 1661761120142431060310.1007/s 13311-013-0222-5PMC 3899488 · doi ↗ · pubmed ↗
- 2Antipsychotic-related movement disorders: drug-induced parkinsonism vs. tardive dyskinesia-key differences in pathophysiology and clinical management Neurol Ther Ward KM Citrome L 233248720183002745710.1007/s 40120-018-0105-0PMC 6283785 · doi ↗ · pubmed ↗
- 3Neuroleptic-related dyskinesias in autistic children: a prospective, longitudinal study J Am Acad Child Adolesc Psychiatry Campbell M Armenteros JL Malone RP Adams PB Eisenberg ZW Overall JE 835843361997918314010.1097/00004583-199706000-00022 · doi ↗ · pubmed ↗
- 4Aripiprazole: from pharmacological profile to clinical use Neuropsychiatr Dis Treat Di Sciascio G Riva MA 263526471120152650885910.2147/NDT.S 88117 PMC 4610784 · doi ↗ · pubmed ↗
- 5Aripiprazole for autism spectrum disorders (ASD)Cochrane Database Syst Rev Hirsch LE Pringsheim T 02016201610.1002/14651858.CD 009043.pub 3PMC 712022027344135 · doi ↗ · pubmed ↗
- 6ECDEU Assessment Manual for Psychopharmacology ECDEU Assessment Manual for Psychopharmacology 534537 Rockville, MDUS Department of Health, Education, and Welfare Publication NIMH 1976 https://ia 600200.us.archive.org/19/items/ecdeuassessmentm 1933 guyw/ecdeuassessmentm 1933 guyw.pdf
- 7Withdrawal syndromes associated with antipsychotic drugs Am J Psychiatry Gardos G Cole JO Tarsy D 1321132413519783028710.1176/ajp.135.11.1321 · doi ↗ · pubmed ↗
- 8Covert dyskinesia associated with aripiprazole: a case report and review of the literature Clin Neuropharmacol Moseley CN Simpson-Khanna HA Catalano G Catalano MC 1281303620132386034610.1097/WNF.0b 013e 31829 b 99d 9 · doi ↗ · pubmed ↗