Validation and cultural translation for the Brazilian Portuguese version of the Estro-Androgenic- Symptom Questionnaire in Women
Cássia Raquel Teatin Juliato, Ana Aline Coelho Oswaldo, Camila Carvalho de Araújo, Marina Rotoli, Lúcia Costa-Paiva, Rossella Nappi, Luiz Gustavo Oliveira Brito

TL;DR
This study translated and validated a questionnaire for hormonal symptoms in menopause for use in Brazilian Portuguese, showing it is reliable and consistent.
Contribution
The paper provides a culturally adapted and validated version of the EASQ-W for Brazilian Portuguese-speaking women.
Findings
The EASQ-W showed satisfactory internal consistency in both groups (Cronbach’s alpha ≥ 0.70).
Test-retest reliability was strong (ICC 0.787-0.977) over 4 weeks.
The questionnaire demonstrated responsiveness to hormonal treatment (p < 0.001).
Abstract
This study aimed to translate and validate the Estro-Androgenic-Symptom Questionnaire in Women (EASQ-W) into Brazilian Portuguese language, as we hypothesized that this tool would be consistent for addressing the specific context of hormonal symptoms in menopause. In a cross-sectional study, a total of 119 women with Genitourinary Syndrome of Menopause (GSM) and 119 climacteric women without GSM were included. The EASQ-W was translated, and its psychometric properties were rigorously examined. Participants completed questionnaires covering sociodemographic details, the EASQ-W, and the Menopause Rating Scale (MRS). A subgroup of 173 women was re-invited after 4 weeks for test-retest analysis of the EASQ-W. Additionally, the responsiveness of the questionnaire was evaluated in 30 women who underwent oral hormonal treatment. The internal consistency of the EASQ-W was found to be…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
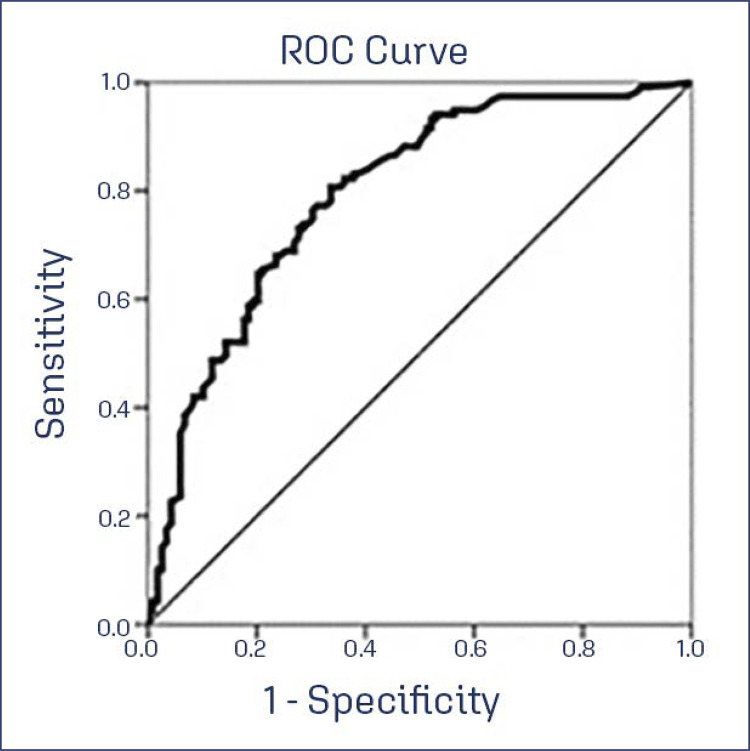 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal and reproductive studies · Sexual function and dysfunction studies · Menopause: Health Impacts and Treatments
Introduction
Menopause signifies a significant juncture in a woman’s life, marked by a cascade of physiological and psychological transformations. As life expectancy continues to rise, it is projected that approximately one-third of a woman’s lifespan will be experienced in the postmenopausal period.^(1)^The array of prevalent menopausal symptoms encompasses vasomotor manifestations, including hot flashes and night sweats, afflicting 57% of women, sexual dysfunction affecting 60%, and joint discomfort experienced by 62%.^(2)^In tandem, psychological symptoms such as irritability, anxiety, sleep disturbances, and urinary issues^(3)^ often accompany this life stage.
A distinctive facet of menopausal experience, the genitourinary syndrome of menopause (GSM), is characterized by a constellation of symptoms encompassing vaginal dryness, burning sensations, reduced lubrication, and other manifestations within the female genitourinary domain. This syndrome arises from histological, anatomical, and clinical transformations attributed to diminishing ovarian hormones.^(4-6)^Unlike the transient nature of vasomotor symptoms, GSM symptoms frequently exhibit an escalating trajectory over time,^(7)^profoundly affecting women’s quality of life and impinging on their sexual well-being.^(8)^The prevalence of GSM symptoms is notable, with approximately 55% of women reporting vaginal dryness, 44% encountering dyspareunia, 37% experiencing vulvar irritation, and 15% grappling with urinary incontinence.^(9)^
Within this dynamic, androgens assume a pivotal role in a woman’s existence. The life course of androgen production entails a natural decline, a phenomenon that becomes more evident over time. Despite estrogen decline, testosterone levels tend to stabilize, with studies indicating that the ovaries of menopausal women sustain a consistent testosterone output.^(10)^However, age-related factors translate to a diminution in androgen production, with serum DHEA and S-DHEA levels in women of their eighth decade plummeting to about a fifth of levels observed in their third decade.^(11,12)^This phenomenon has led to the conceptualization of androgen deficiency syndrome, denoting a reduction in androgen production post-menopause, giving rise to symptoms encompassing reduced well-being, dysphoric mood, fatigue, and alterations in sexual function.^(13)^
In the realm of clinical research, validated questionnaires serve as indispensable instruments. Regrettably, a dearth of questionnaires exists that comprehensively assess symptoms of estrogen, androgen deficiency, and GSM in peri- and post-menopausal women. Notably, the Estro-Androgenic Symptom Questionnaire in Women^(14)^ was developed and validated to offer enhanced characterization of midlife women experiencing vulvovaginal atrophy and GSM. Motivated by this context, the present study seeks to bridge the gap by translating and culturally validating the EASQ-W questionnaire into Brazilian Portuguese, facilitating its application and utility within this population.
Methods
We conducted a cross-sectional study spanning from June 2022 to July 2023 at the Department of Obstetrics and Gynecology, School of Medical Sciences, University of Campinas (UNICAMP). This investigation adhered to the guidelines for Reporting Reliability and Agreement Studies (GRRAS) concerning projects involving psychometric variables.^(15)^Approval from the Institutional Review Board was obtained, and all participating women provided informed consent after a comprehensive explanation of the study objectives.
We included 119 menopausal women exhibiting vasomotor symptoms (e.g., hot flashes, night sweats), genital atrophy, vaginal dryness, urgency, urinary incontinence, sexual issues (such as reduced libido, orgasmic dysfunction), psychological symptoms (e.g., irritability, discouragement, anxiety, cognitive decline, concentration difficulties, insomnia), and muscle or joint discomfort (group: menopause). Hormone therapy was individualized according to the needs and characteristics of the patient, with continuous combined therapy of low dose estradiol (1 mg oral or 0.75 mg transdermal) associated with to an oral progestogen (norethisterone 0.5 mg or micronized progesterone 100 mg) for women with a uterus or oral or transdermal isolated estrogen only for hysterectomized women. The control group (n=119) encompassed women with regular menstrual cycles (frequency between 28-38 days)^(16)^and devoid of menopausal symptoms. In totality, 238 women were included in the study. Exclusion criteria encompassed women undergoing menopausal symptom treatment (systemic or vaginal hormone therapy with estrogens, progestogens, or androgens), pregnant women, and individuals with reading and/or comprehension impediments.
Following authorization from the questionnaire author (R.E.N.), a meticulous translation process was undertaken. Two native Brazilian translators, proficient in English, translated the questionnaire from English to Brazilian Portuguese, with official authorization for scientific document translation. The synthesis of the translations yielded a common version, which was subsequently back translated into English by a third translator. Concordance between the back-translated instrument and the original version was verified. The Brazilian Portuguese EASQ-W was evaluated by an expert committee (C.R.T.J., L.G.O.B., C.C.A.) for linguistic adaptation to enhance participant comprehension. A pre-test involving an interview-based application of the EASQ-W to 30 women revealed no necessity for further adjustments, leading to approval of the final questionnaire for research use (Supplementary Material - Table 1S).
Before applying the EASQ-W, we collected baseline variables as age, body mass index (BMI), ethnics, parity, comorbidities, menopausal status, and sexual activity. Psychometric variables for analyzing the EASQ-W were internal consistency, floor and/or ceiling effect, test-retest reliability, responsiveness to treatment, and discriminant/construct validity.
The EASQ-W assesses age-related, psychological, anatomical, vasomotor, urogenital, weight gain, and sleep-related symptoms, therefore offering both researchers an easy and reliable method to quantify relative and absolute change in symptom frequency after treatment. The EASQ-W includes the prevalence of symptoms (vasomotor, psychological symptoms, insomnia, muscle and joint discomfort, sexual function, and urogenital symptoms), in addition to being an easy-to-understand and self-administered questionnaire. It contains 32 questions, which are grouped into eight domains: age, psychological, sexual, anatomical, weight, urological, vasomotor symptoms, and sleep. Each question can be answered with “no” or “yes”, and in the case of “yes” a score of 1-10 must be assigned. The total score is obtained by the sum of all scores.
The MRS has 11 questions divided into three domains: somatic-vegetative symptoms, psychological symptoms, and urogenital symptoms. The response to each question is rated on an intensity scale ranging from zero (no symptoms) to four (very intense symptoms). The total MRS score is obtained by adding the scores for each domain, so that the higher the score, the more intense the symptoms and the worse the quality of life. These items are categorized into the following 3 subscales or domains: somatic-vegetative (4 items), psychological (4 items), and urogenital (3 items).
Descriptive statistics entailed frequency tables with percentages for categorical variables and mean and standard deviation for numerical variables. Comparative analysis involved Chi-square or Fisher’s exact tests for categorical variables and the non-parametric Mann-Whitney test for numerical variables. Internal consistency was evaluated using Cronbach’s alpha index, with values of 0.70-0.95 deemed adequate. Test-retest reliability was assessed using mean difference and intraclass correlation coefficient (ICC). Construct validity involved correlation testing between EASQ-W and MRS scores. Floor and ceiling effects were determined by identifying scores exceeding 15% below or above the end value. Responsiveness was assessed through a pre- and post-intervention EASQ-W score comparison using the Wilcoxon test.
The EASQ-W score cutoff point distinguishing case and control groups was obtained via ROC curve analysis. A significance level of 5% was applied, and SAS statistical package (Cary, NC, USA) was utilized for analyses.
The study complied with Brazilian ethical standards involving human beings protocol 4.814.688 (CAAE: 45451521.8.0000.5404).
Results
Baseline characteristics
Table 1 illustrates the distribution of the two study groups based on sociodemographic and obstetric variables. Notably, patients within the Genitourinary Syndrome of Menopause (GSM) group exhibited distinct characteristics compared to the control group, predominantly consisting of women in their reproductive phase. Specifically, individuals in the GSM group were older than those in the control group (32.2 ± 10.4 years versus 57.4 ± 10.9 years, p < 0.001). Additionally, they displayed a lower educational attainment (p < 0.001) and a heightened prevalence of various comorbidities, including arterial hypertension (p < 0.001), diabetes mellitus (p < 0.001), and urinary incontinence (p < 0.001). However, no statistically significant differences were observed in terms of parity, body mass index, ethnicity, smoking habits, and the presence of chronic obstructive pulmonary disease between the two groups. This comprehensive examination of sociodemographic and obstetric variables underscores the distinct profiles of the GSM and control groups, which is instrumental for contextualizing the subsequent findings of the study.
Table 1. Baseline characteristics of the women included in the two study groups (n=238)VariableGSM Group (n= 119)Control Group (n= 119)p-valueAge years (X±SD)57.4±10.932.2±10.4<0.001BMI (X±SD)26.5±5.627.49±4.80.08Schooling years (X±SD)12.8±9.116.9±5.5<0.001Ethnicity n (%) n=231 white78 (68.4)75 (59.1)0.994Not white36 (31.6)52 (40.9) Pregnancy2.8±1.91.1±1.3<0.001Parity vaginal1.6±1.81.07±1.50.09Cesarean section0.8±11.02±1.10.82Sexually Active (yes)70 (59.3)110 (92.4)<0.001Hypertension (yes) n=23757 (48.3)20 (16.83)<0.001Diabetes Mellitus (yes) n=23621 (18)3 (2.5)<0.001COPD (Yes)4 (3.3)4 (3.3)1Smoking(yes) n=22410 (8.5)11 (610.4)0.626Urinary incontinence (yes)66 (55.5)22 (18.5)<0.001**GSM - Genitourinary Syndrome of Menopause; BMI - body mass index; COPD - severe obstructive pulmonary disease; X - mean; SD - standard deviation; *p-value; ** Chi square; ***Fisher’s exact test
Discriminant validity and floor/ceiling effects of EASQ-W and MRS scores
Table 2 presents the outcomes of the EASQ-W and Menopause Rating Scale (MRS) questionnaires among women belonging to the Genitourinary Syndrome of Menopause (GSM) and control groups. Our analysis reveals a substantial contrast in the scores across all domains of the EASQ-W questionnaire between these groups, except for the psychological domain. This noteworthy exception underscores the questionnaire’s excellent discriminant validity, as it effectively discerns between the two distinct groups based on the presence of genitourinary symptoms associated with menopause.
Table 2. Discriminant validity of the EASQ-W and Menopause Rate Scale scores between women with and without genitourinary syndrome of menopause SGM (n=119)Control (n= 119 )p-Value*M±DPMinimumMaximumM±DPMinimumMaximumEASQ-W Age33.8±19.204813.6 ± 16.6073<0.001Psychological16±13.402711.5±11.70500.013Sexual14.8±9.80235.9±8.9030<0.001Anatomical16±12.40253.3±6.6031<0.001Body weight11.2±100206±07030<0.001Urological13.2±10.20225.5±8.4030<0.001Vasomotor6.5±70101.6±3.6018<0.001Sleep9.8±8.40166.1±7.4027<0.001Total120.6±64.8016953.61±55.90254<0.001MRS Somatovegetative5.5±3.90152.65±3011<0.001Psychological5.2±4.70165.5±4.40160.525Urogenital4.4±3.20121.7±2.8012<0.001Total15.2±9.90359.8±8.7035<0.001GSM - genitourinary menopausal syndrome; M - mean; SD - standard deviation; MRS - menopause rate scale questionnaire
Regarding to floor and ceiling effects, control group showed a floor effect in all EASQ-W domains. Women with GSM showed a floor effect in all domains and a floor and ceiling effect in the sexual domain (Table 3).
Table 3. Ceiling and floor effect analysis of questionnaire scores EASQ-WEASQ-WGSM GroupControl GroupFrequencyPercentFrequencyPercentAge Floor 0-122117.6 (Floor effect)7260.5 (Floor Effect)13-679689.74638.7Ceiling 68-8021.710.8Psychological Floor 0-74134.5 (Floor effect)5344.5 (Floor Effect)8-427462.26352.9Ceiling 43-5040.332.6Sexual Floor 0-42218.5(Floor effect)7260.5 (Foor Effect)5-257764.73932.8Ceiling 26-302016.8 (Ceiling effect)86.7Anatomical Floor 0-73731.1 (Floor effect)10084.3 (Floor Effect)8-427966.4 Ceiling 43-5032.51915.7Body Weight Floor 0-43831.9 (Floor effect)6453.8 (Floor effect)5-256655.45243.7Ceiling 26-301512.732.5Urological Floor 0-43327.7 (Floor effect)7966.4 (Floor effect)5-2569583630.3Ceiling 26-301714.343.3Vasomotor Floor 0-35446.2 (Floor effect)9983.2(Floor effect)4-164740.21916Ceiling 17-201613.610.8Sleep Floor 0-43630.3 (Floor effect)6151.3 (Floor effect)5-257663.95344.5Ceiling 26-3075.854.2Total Floor 0-482117.6 (Floor effect)6151.3 (Floor effect)49-2719781.55344.5Ceiling 272-32010.954.2
Internal consistency of the EASQ-W questionnaire can be evaluated in table 4. Cronbach’s Alpha values show the reliability of the questionnaire, that is, how much the partial measures are consistent with each other. The anatomical, vasomotor and sleep domains showed values below 0.70, but above 0.5, which shows good agreement. The other domains showed better agreement, with values above 0.70.
Table 4. Internal consistency of the EASQ-W questionnaire by study groupEASQ-WGSM Group (n=119)Control Group (n=119)Cronbach’s alphaCronbach’s alphaAge0.8220.860Psychological0.7930.829Sexual0.7980.896Anatomical0.6970.690Body Weight0.8040.615Urological0.8090.868Vasomotor0.6870.563Sleep0.5930.643Total0.9210.945
Test–retest reliability, construct validity, and responsiveness to treatment
Test-Retest Analysis: Following a 4-week interval, a subset of 173 women (106 from the GSM group and 67 from the control group) were randomly selected for test-retest assessment. During this retest, the questionnaire under investigation was administered. Evaluation of the test-retest data revealed minimal variation across most domains. Notably, the intraclass coefficient (ICC) exhibited values approximating 1, indicating a high level of correlation between the responses during the initial test and the subsequent retest. This outcome underscores the excellent consistency in participant responses over time (Table 5).
Table 5. Test and retest reliability of the EASQ-W questionnaireEASQ-WTest ScoresRetest scorep-valueDifferenceICC95%X ±SDX ±SDX ±SDGSM group (n=106) Age35±1936.3±20.2<0.0011.25±40.9770.964-0.985Psychological16.2±13.416.7±13.40.0410.48±4.40.9450.921-0.962Sexual15.6±9.715.9±10.10.0860.31±2.90.9580.939-0.971Anatomical16.2±12.615.9±10.1<0.0010.6±2.60.9790.968-0.978Body Weight11.3±10.211.5±10.30.2110.26±2.60.9680.954-0.978Urological13.5±10.313.8±10.40.2580.23±3.10.9560.936-0.970Vasomotor6.6±7.17.1±7.30.0230.42±3.40.8920.846-0.925Sleep10±8.79.9±8.40.941-0.10±2.90.9440.919-0.962Total124.9±64.7128.4±67.3<0.0013.4±120.9820.973-0.988Control group (n=67) Age12.2±16.210.8±15.40.019-1.5±5.10.9450.908-0.966Psychological10.8±11.19.5±110.020-1.4±4.60.9080.849-0.944Sexual5.5±95.6±9.20.4230.15±2.20.9720.955-0.982Anatomical2.4±62.4±60.4060.01±0.70.9720.955-0.983Body weight4.9±5.84±6.10.062-0.9±3.40.7870.673-0.864Urological4.7±84.6±8.30.870-0.12±2.60.8700.919-0.968Vasomotors1.5±3.21.5±3.10.9380.03±1.10.9360.898-0.960Sleep5.6±7.55.4±7.40.622-0.18±1.30.9850.977-0.991Total*47.6±52.643.8±53.30.141-3.8±12.70.9690.948-0.981ICC - intraclass coefficient; SD - standard deviation; *p-value between test and retest (Wilcoxon); **p ICC value
Construct Validity: Construct validity was established by comparing the scores of the EASQ-W with those of the Menopause Rating Scale (MRS). This analysis yielded a moderate correlation between the two questionnaires, with a correlation coefficient (r) of 0.64580 (p < 0.001), as depicted in table 6. This finding substantiates the congruence between the EASQ-W and MRS scores in evaluating menopausal symptoms.
Table 6. Construct validity between EASQ-W and MRS questionnairesEASQ-WMRS SomaticMRS PsychologicalMRS UrogenitalMRS TotalAger=0.56628 p<0.001r=0.52308 p<0.001r=0.53708 p<0.001r=0.61657 p<0.001Psychologicalr=0.48301 p<0.001r=0.54563 p<0.001r=0.49810 p<0.001r=0.57943 p<0.001Sexualr=0.33831 p=0.0002r=0.36364 p<0.001r=0.61735 p<0.001r=0.46331 p<0.001Anatomicalr=0.44661 p=0.0002r=0.343104 p=0.0002r=0.57002 p<0.001r=0.54541 p<0.001Body Weightr=0.34013 p=0.0002r=0.30247 p=0.0008r=0.33190 p=0.0002r=0.34402 p=0.0002Urologicalr=0.35050 p<0.0001r=0.32401 p=0.0003r=0.40212 p<0.0001r=0.45851 p<0.0001Vasomotorr=0.28466 p=0.0017r=0.28700 p=0.0016r=0.28466 p=0.0017r=0.31793 p=0.0004Sleepr=0.40329 p<0.001r=0.36989 p<0.001r=0.37929 p<0.001r=0.44199 p<0.001Totalr=0.55068 p<0.001r=0.55900 p<0.001r=0.60322 p<0.001r=0.64580 p<0.001r - Spearman correlation; p-value
Responsiveness Assessment: To gauge responsiveness, a subgroup of women (n=30) from the GSM group underwent a 90-day regimen of oral hormonal therapy for menopause. Subsequent analysis of the scores across all domains and the total score of the EASQ-W demonstrated a noteworthy reduction post-treatment, indicating a favorable response to the therapy. Detailed results are presented in table 7.
Table 7. Responsiveness after 90 days of oral hormonal therapy (n= 30)EASQ-W (X±SD)Pre-treatmentPost treatmentp-valueAge42.3 (17.7)13.6 (18.1)<0.001Psychological23.9 (12.3)7.3 (11.1)<0.001Sexual18.6 (9.3)5.3 (7.5)<0.001Anatomical22.3 (12.3)7.3 (10.7)<0.001Body Weight13.6 (11.8)4.6 (8.4)<0.001Urological15.2 (9.6)4.7 (6.6)<0.001Vasomotor11.9 (7.7)7.1 (6.6)<0.001Sleep12.9 (7.7)4.1 (6.8)<0.001Total160.7 (57.2)51.1 (68.9)<0.001Wilcoxon test
ROC Curve Analysis and Cut-off Point Determination: A Receiver Operating Characteristic (ROC) curve was constructed to ascertain the questionnaire’s cut-off point capable of effectively distinguishing between women with and without GSM. The analysis indicated that a cut-off point exceeding 60 points achieved a sensitivity of 80% (95% CI: 72.2 - 80.1), specificity of 66.4% (95% CI: 57.7 - 74.6), positive predictive value of 70.6% (95% CI: 62.1 - 84.9), and a negative predictive value of 77.5% (95% CI: 67.9 - 84.9) for identifying GSM. This information, depicted in figure 1, underscores the utility of the EASQ-W in effectively discriminating between individuals with and without GSM.
Figure 1ROC curve
Discussion
This study successfully accomplished the cultural translation and psychometric evaluation of the Estro-Androgenic Symptom Questionnaire in Women (EASQ-W) for Brazilian Portuguese. The EASQ-W, a comprehensive 32-item questionnaire encompassing key symptoms associated with estrogen and androgen decline following menopause, was meticulously translated, and culturally validated to ensure its relevance and reliability within this population. Notably, this approach addresses a significant gap in the existing literature, as few questionnaires adopt this comprehensive perspective.
Distinct from vasomotor symptoms, the Genitourinary Syndrome of Menopause (GSM) precipitates chronic histological, anatomical, and clinical changes in the genital and lower urinary tract, attributed to the gradual reduction of ovarian hormones.^(4-6)^This syndrome’s progressive nature underscores the urgency of accurate diagnosis and intervention, especially given the potential for worsening symptoms and complications such as vaginal stenosis.^(1,17,18)^ In light of this complexity and the demand for more advanced survey tools, the translation and cultural validation of the EASQ-W were undertaken.
The psychometric evaluation of the EASQ-W revealed its strong cultural adequacy. Its domain and total scores exhibited significant differences between the case and control groups, indicative of robust discriminant validity. While the psychological domain exhibited no variance between the groups, this can be attributed to the domain’s broader nature encompassing psychological concerns linked to both GSM and symptoms arising from estrogen and androgen decline. Internal consistency, assessed using the Cronbach index, indicated favorable results, with values exceeding 0.70, indicating strong internal coherence. Although the anatomical, vasomotor, and sleep domains presented slightly lower values, their adequacy was still maintained. The test-retest reliability analysis demonstrated the questionnaire’s stability over time, with consistent results after a 4-week interval.
Furthermore, the EASQ-W exhibited a notable and moderate correlation with the Menopause Rating Scale (MRS), which assesses climacteric symptoms and quality of life. Both questionnaires effectively detected postmenopausal syndrome symptoms, with the EASQ-W distinguishing itself by its broader scope and domain-specific questions. The MRS is an excellent and well-known questionnaire applied in clinical studies, but it contains less detail on symptoms and few questions. Some symptoms of menopause overlap with age-related complaints, particularly complaints related to androgen deficiency such as decreased strength, memory problems, decreased energy, signs of aging. The EASQ-W also addresses some more detailed questions about psychological aspects not covered in the MRS such as fear, panic attacks, pleasure of living. One of the main differences in the application of this questionnaire is the detailing of urogenital symptoms, which contains five specific questions about vaginal symptoms and three about urinary incontinence/urinary symptoms. Despite being longer and requiring more interview time, this detail of the EASQ-W can be advantageous when one needs a more adequate characterization of the symptoms arising not only from menopausal hypoestrogenism, but also from factors related to aging and the drop in androgenic levels that is observed with the advancement of age and during post-menopause.
Assessment of the EASQ-W’s responsiveness following treatment underscored its potential as a valuable tool for monitoring treatment outcomes, evidenced by the significant reduction in scores observed 30 days post-treatment. The study also established a cut-off point of 60 for diagnosing GSM and symptoms linked to estrogen and androgen decline, an invaluable addition that was not present in the original version of the questionnaire.
This study’s strengths encompass a robust sample size, comprehensive evaluation of the most important psychometric variables (discriminant and construct validity, ceiling and floor effect, internal consistency, test/retest reliability, responsiveness) into a single study, establishment of a cut-off point for EASQ-W questionnaire, and assessment of responsiveness to pharmacological treatment. However, some baseline differences between the study groups represent a limitation.
Conclusion
In summation, the EASQ-W stands as a valid instrument, adept at discriminating symptoms arising from hormonal decline post-menopause. Its commendable internal consistency, reliability, and responsiveness render it a valuable tool for clinical assessment and treatment evaluation. The newly established cut-off point of 60 contributes to its diagnostic utility for identifying postmenopausal syndrome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The NAMS 2020 GSM Position Statement Editorial Panel The 2020 genitourinary syndrome of menopause position statement of The North American Menopause Society Menopause 202027997699210.1097/GME.000000000000160932852449 · doi ↗ · pubmed ↗
- 2Makara-Studzinska MT Krys-Noszczyk KM Jakiel G Epidemiology of the symptoms of menopause - an intercontinental review Prz Menopauzalny 201413320321110.5114/pm.2014.4382726327856 PMC 4520365 · doi ↗ · pubmed ↗
- 3Lui JF Filho Baccaro LF Fernandes T Conde DM Costa-Paiva L Pinto AM Neto Factors associated with menopausal symptoms in women from a metropolitan region in Southeastern Brazil: a population-based household survey Rev Bras Ginecol Obstet 201537415215810.1590/SO 100-720320150005282 Portuguese 25992497 · doi ↗ · pubmed ↗
- 4Portman DJ Gass ML Vulvovaginal Atrophy Terminology Consensus Conference Panel Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women's Sexual Health and the North American Menopause Society J Sex Med 201411122865287210.1111/jsm.1268625155380 · doi ↗ · pubmed ↗
- 5Daan NM Fauser BC Menopause prediction and potential implications Maturitas 201582325726510.1016/j.maturitas.2015.07.01926278873 · doi ↗ · pubmed ↗
- 6Portman DJ Gass ML Vulvovaginal Atrophy Terminology Consensus Conference Panel Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women's Sexual Health and the North American Menopause Society Menopause 201421101063106810.1097/GME.000000000000032925160739 · doi ↗ · pubmed ↗
- 7Di Boaventura M Luo X Moffat M Bushmakin AG Kumar M Bobula J The association between vulvovaginal atrophy symptoms and quality of life among postmenopausal women in the United States and Western Europe J Womens Health (Larchmt)201524971372210.1089/jwh.2014.517726199981 · doi ↗ · pubmed ↗
- 8Palacios S Mejia A Neyro JL Treatment of the genitourinary syndrome of menopause Climacteric 201518 Suppl 1232910.3109/13697137.2015.107910026366797 · doi ↗ · pubmed ↗