Unveiling the Expected: A Case Report of a Massive Congenital Lung Cyst in a 22-Year-Old Male
Nosagie Ohonba, Devon Thorpe, Yashini Gopal, Kiana Bhola, David Jordanovski

TL;DR
A 22-year-old man with a rare congenital lung cyst experienced symptoms for years before diagnosis and successful surgery.
Contribution
This case report highlights the rare occurrence of adult-onset congenital pulmonary airway malformation.
Findings
A 22-year-old male presented with hemoptysis and dyspnea due to a large congenital lung cyst.
Surgical resection confirmed the diagnosis and led to a full recovery.
Adult-onset CPAM should be considered in young adults with unexplained respiratory symptoms.
Abstract
Congenital pulmonary airway malformations (CPAMs) are predominantly identified prenatally or during infancy, with adult-onset cases being considered extremely rare. This case report describes a 22-year-old male who presented with hemoptysis and exertional dyspnea, leading to the diagnosis of CPAM. The patient had experienced small-volume hemoptysis for four years, which escalated to larger volumes and progressive dyspnea one week before hospital admission. A chest CT scan revealed a large 13.2 cm thin-walled cavitary lesion with an air-fluid level in the left lower lobe. The patient underwent left video-assisted thoracoscopic surgery (VATS) resection, which confirmed a CPAM originating from the left lower lobe. The postoperative recovery was uneventful, and the patient was symptom-free at follow-up. This case highlights the need to consider CPAM in the differential diagnosis of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
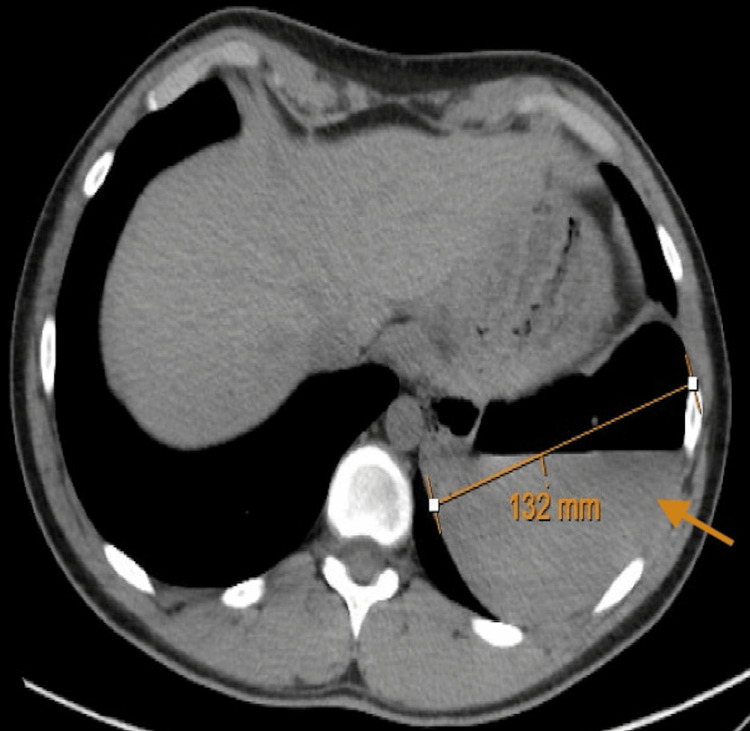 Figure 1
Figure 1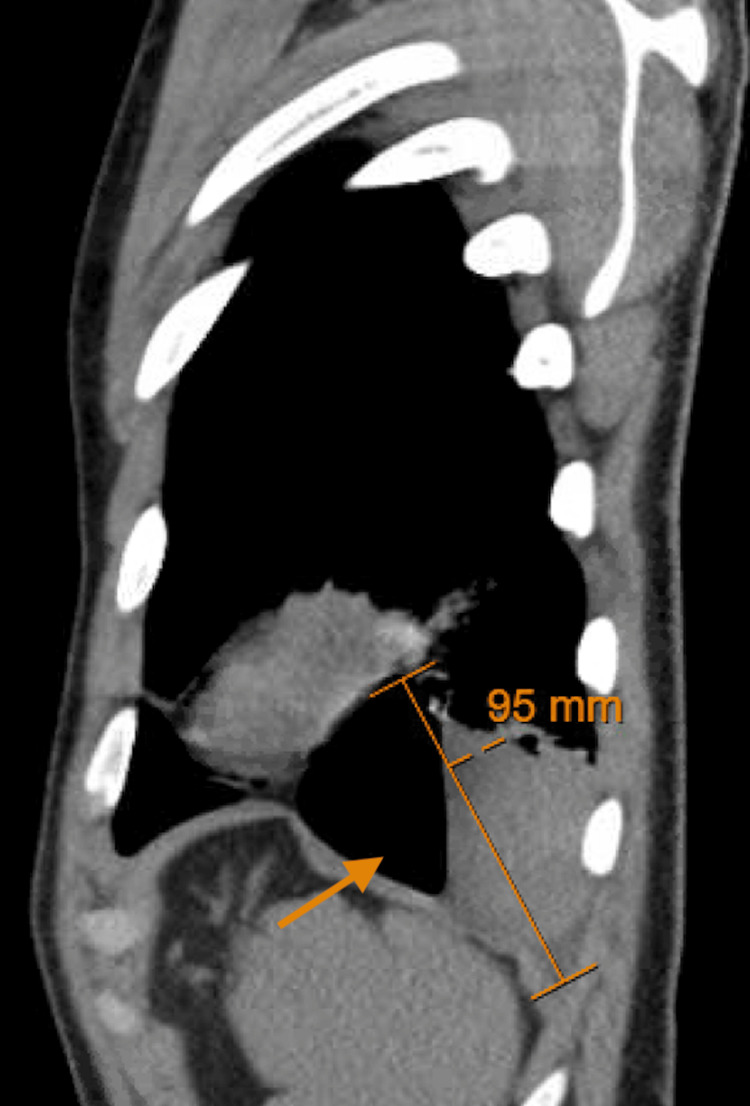 Figure 2
Figure 2| Test | Result | Reference value |
| Hemoglobin | 12.6 g/dl | 14.0-17.0 g/dl |
| WBC | 7.27/nl | 4.5-11.0/nl |
| Absolute neutrophil count | 4.07/nl | 2.00-6.60/nl |
| Absolute lymphocyte count | 2.41/nl | 0.70-3.70/nl |
| Eosinophil count | 0.21/nl | 0.00-0.20/nl |
| Platelets | 260/nl | 150-450/nl |
| CRP | 3.7 mg/l | 0.0-9.0 mg/l |
| ESR | <1 mm/hr | 0-23 mm/hr |
| C3 complement | 103.0 mg/dl | 90-180 mg/dl |
| C4 complement | 25 mg/dl | 10-40 mg/dl |
| D-dimer | <0.30 ug/ml | 0.00-0.49 ug/ml |
| HIV 1/2 antigen and antibodies | Undetectable | Undetectable |
| Procalcitonin | 0.02 ng/ml | 0.00-0.25 ng/ml |
| Cryptococcus antigen | Negative | Negative |
| Coccidioides antibodies (IgG and IgM) | Negative | Negative |
| Urine histoplasma antigen | Negative | Negative |
| Hepatitis B surface antigen | Negative | Negative |
| Hepatitis C viral antibodies | Negative | Negative |
| Respiratory viral panel | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Tracheal and airway disorders · Neonatal Respiratory Health Research
Introduction
Congenital pulmonary airway malformations (CPAMs) are typically identified prenatally or in infancy, with adult-onset cases being exceptionally rare [1]. CPAM results from the cessation of lung development during various stages of embryogenesis. Infants with this diagnosis can exhibit a wide range of severity, from being asymptomatic until later in life to experiencing respiratory distress during the neonatal period. Incidence data from large population registries suggests congenital lung cysts occur at rates ranging from 1 per 8,300 to 35,000 live births [1]. An estimated 80% of the lesions are recognized in the neonatal period; however, there are few case reports highlighting diagnosis in adulthood [2]. Adult patients may either be asymptomatic or exhibit symptoms such as recurrent infections, pneumothorax, shortness of breath, or hemoptysis [3]. We present the case of a 22-year-old male without prior significant medical history who presented with hemoptysis and exertional dyspnea, leading to the unexpected diagnosis of CPAM. The case highlights the unusual presentation of CPAM in adulthood and emphasizes the importance of considering this condition in the differential diagnosis of respiratory symptoms, even in individuals without a history of congenital anomalies.
Case presentation
A 22-year-old male with no past medical history presented to the hospital with a two-day complaint of hemoptysis and exertional dyspnea. He had experienced episodic, small-volume hemoptysis over the previous four years, which was never investigated. However, within the week prior to presentation, he began having larger-volume hemoptysis and progressive dyspnea on exertion. He denied a recent fever, chest pain, respiratory infection, or coryzal symptoms. He had no history of serositis, pleuritis, synovitis, arthritis, or bleeding diathesis. His additional history was negative for recent medication use beyond naproxen, recent sick contacts, recent travel, or trauma. Family history was also negative for bleeding disorders or autoimmune diseases, and the patient did not use recreational drugs.
Upon presentation to the hospital, his vitals remained stable, and he was oxygenating at 98% on room air without accessory muscle use or respiratory distress. His examination was unremarkable, and his chest was clear to auscultation. A chest CT scan with contrast revealed a large 13.2 cm thin-walled cavitary lesion with an associated air-fluid level, replacing most of the inferior segment of the left lower lobe, with atelectatic changes in the subjacent lung (Figure 1, Figure 2).
Axial CT scan of the chest showing a large 13.2 cm thin-walled cavitary lesion with an air-fluid level in the left lower lobe, as indicated by the arrow
Sagittal CT scan of the chest showing a thin-walled cavitary lesion with an air-fluid level in the left lower lobe, as indicated by the arrow
An extensive workup was performed, including tests for CRP, ESR, C3 complement, C4 complement, D-dimer, respiratory viral panel, hepatitis serologies, urine drug screen, *Cryptococcus *antigen, *Coccidioides *antibodies (IgG and IgM), and urine histoplasma antigen. All results were negative, except for mild anemia (Table 1).
A diagnostic and therapeutic left video-assisted thoracoscopic surgery (VATS) resection was performed. Inspection confirmed that the cyst originated from the medial basilar aspect of the left lower lobe. The large hemorrhagic cyst was incised, and the blood was evacuated. The cyst was then decompressed, and a pathology specimen was obtained. An interval chest tube was placed and removed prior to discharge.
The patient fully recovered from the surgical procedure and remained symptom-free. The pathology confirmed the diagnosis of CPAM.
Discussion
CPAM, previously known as congenital cystic adenomatoid malformation (CCAM), is a rare congenital anomaly of the lung characterized by cystic and adenomatous overgrowth of terminal bronchioles. While CPAM is typically diagnosed in utero or during infancy due to associated respiratory distress or infection, cases presenting in adulthood are exceedingly rare, as seen in this 22-year-old male without any significant past medical history [1].
CPAMs stem from aberrations in lung branching morphogenesis during fetal development [4]. These anomalies are believed to arise at various levels of the tracheobronchial tree and at different stages of lung maturation, potentially influenced by factors like in utero airway obstruction or atresia.
Incidence data from large population registries suggests congenital lung cysts occur at rates ranging from 1 per 8,300 to 35,000 live births [1]. Among CPAMs, large-cyst subtypes predominate, constituting approximately 70% of cases, or 2-8 per 100,000 live births [5]. Formerly termed CCAMs, CPAMs were classified into three major types based on cyst size and cellular characteristics, primarily bronchial, bronchiolar, or bronchiolar/alveolar duct cells [6-8].
The clinical presentation of CPAM is diverse. While many are identified through routine prenatal ultrasound, recent advancements have led to the detection of smaller lesions, often asymptomatic at birth. Roughly 25% of newborns with CPAM exhibit symptoms, a notable decrease compared to earlier reports [9]. Approximately three-quarters of infants with a prenatal CPAM diagnosis remain asymptomatic initially, with one-third diagnosed after the neonatal period.
In older children, CPAM may manifest as recurrent pneumonia, cough, dyspnea, cyanosis, or even spontaneous pneumothorax. Physical examination findings commonly include decreased breath sounds over the lesion, hyperresonance, and chest wall asymmetry [9]. In this case, the patient presented with a sudden onset of hemoptysis and exertional dyspnea, symptoms that are not specific to CPAM but rather suggestive of a variety of pulmonary conditions, including infections, neoplasms, or vascular abnormalities.
The definitive diagnosis of CPAM often requires histopathological examination of the resected specimen, as was performed in this case [10]. Surgical resection via VATS is the mainstay of treatment for symptomatic CPAM, aiming to alleviate symptoms, prevent complications such as infection or hemorrhage, and potentially reduce the risk of malignant transformation.
Conclusions
While CPAM is typically diagnosed in infancy, it should be considered in the differential diagnosis of young adults presenting with respiratory symptoms and radiographic evidence of cystic lung lesions. Timely recognition and surgical intervention can lead to favorable outcomes, as demonstrated in this case. Our case highlights the rarity of CPAM presenting in adulthood, particularly with an unusual symptomatology of hemoptysis. Such late presentations underscore the importance of considering CPAM in the differential diagnosis of respiratory complaints, even in individuals without a history of congenital anomalies or predisposing factors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Congenital cystic adenomatoid malformation: accuracy of prenatal diagnosis, prevalence and outcome in a general population Prenat Diagn Gornall AS Budd JL Draper ES Konje JC Kurinczuk JJ 99710022320031466383710.1002/pd.739 · doi ↗ · pubmed ↗
- 2Congenital cystic adenomatoid malformation of lung in adults: 2 rare cases report and review of the literature Diagn Pathol Feng A Cai H Sun Q Zhang Y Chen L Meng F 37720122247236510.1186/1746-1596-7-37PMC 3349468 · doi ↗ · pubmed ↗
- 3Case 59Rare and Interesting Cases in Pulmonary Medicine Ataya A Harman E 215217 Academic Press 2017
- 4Bronchial atresia: the hidden pathology within a spectrum of prenatally diagnosed lung masses J Pediatr Surg Kunisaki SM Fauza DO Nemes LP Barnewolt CE Estroff JA Kozakewich HP Jennings RW 61654120061641010910.1016/j.jpedsurg.2005.10.082 · doi ↗ · pubmed ↗
- 5Pulmonary cysts in early childhood and the risk of malignancy Pediatr Pulmonol Priest JR Williams GM Hill DA Dehner LP JafféA 14304420091906122610.1002/ppul.20917 · doi ↗ · pubmed ↗
- 6Cystic and congenital lung disease in the newborn Perspect Pediatr Pathol Stocker JT Drake RM Madewell JE 9315441978 https://pubmed.ncbi.nlm.nih.gov/366553/366553 · pubmed ↗
- 7Congenital malformations and genetic disorders of the respiratory tract (larynx, trachea, bronchi, and lungs)Am Rev Respir Dis Landing BH Dixon LG 1511851201979 https://pubmed.ncbi.nlm.nih.gov/380420/38042010.1164/arrd.1979.120.1.151 · doi ↗ · pubmed ↗
- 8Congenital cystic adenomatoid malformation of the lung: classification and morphologic spectrum Hum Pathol Stocker JT Madewell JE Drake RM 1551718197785671410.1016/s 0046-8177(77)80078-6 · doi ↗ · pubmed ↗