Intervention to improve adverse event reporting in the emergency department: Protocol of a systematic review and meta-analysis
Collins Atta Poku, Jonathan Bayuo, Atswei Adzo Kwashie, Adelaide Maria Ansah Ofei

TL;DR
This paper outlines a systematic review and meta-analysis protocol to evaluate interventions that improve adverse event reporting in emergency departments for better patient safety.
Contribution
The study introduces a comprehensive protocol to assess the effectiveness of interventions for adverse event reporting in emergency departments.
Findings
The study will summarize interventions to improve adverse event reporting in emergency departments.
It will identify effective approaches to enhance adverse event reporting for patient safety.
A meta-analysis will be conducted if sufficient data is available.
Abstract
Adverse event reporting is crucial for improving patient safety and identifying areas for improvement in the emergency department. Many interventions have been employed in that regard, and have been found to increase adverse event reporting rates in various settings. All published research that studied the various interventions and their effectiveness on adverse event reporting in the Emergency Department will be reviewed in this paper. CINAHL, PubMed, Medline, Cochrane Reviews Library, EMBASE, Scopus, OVID, Science Direct and Web of Science will all be searched. Studies published since January 2000 that investigated the interventions to improve adverse event reporting will be included. Two independent reviewers will execute the selection and extraction process, and we will carry out a qualitative synthesis. A meta-analysis, if possible, will be undertaken. The present study will…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
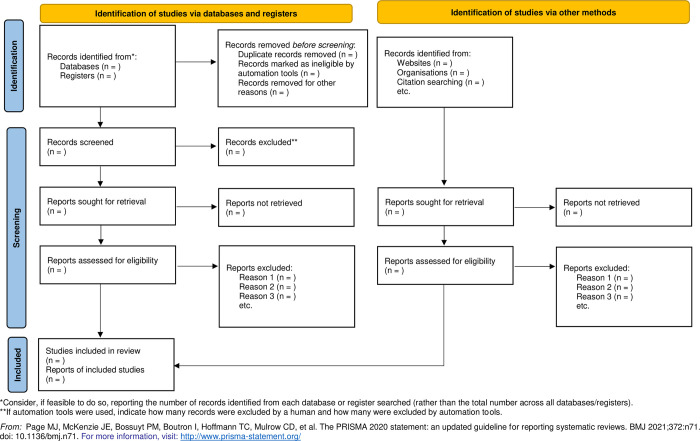 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Malpractice and Liability Issues · Patient Safety and Medication Errors · Clinical Reasoning and Diagnostic Skills
Background
Patient safety has been identified as an important component of quality care [1]. It is a discipline in the healthcare industry concerned with preventing, reducing or eliminating risks, errors, and/or harm to patients during the delivery of healthcare; and encompasses an integrated strategy that includes developing a safety culture, improving communication, minimizing risks, utilizing technology, and standardizing systems and procedures [2].
When discussing ways to enhance patient safety, one of the most difficult parts for both patients and healthcare providers is the healthcare system’s seeming unwillingness to learn from its errors. Too often, healthcare providers and healthcare facilities fail to notify others when an error happens, or to share what they have learned when an investigation is concluded [3]. As a result, the same mistakes or errors are repeated in various settings, and patients continue to suffer injuries as a result of these preventable errors (adverse events [AEs]). Meanwhile, a major key strategy in evaluating and improving patient safety is identifying and reporting AEs in healthcare settings. AE reporting helps to improve organizational learning and quality improvement [2].
Adverse events refer to any unintended harm or injury caused to a patient during medical care, such as medication errors, misdiagnosis, falls, and infections, rather than the being due to the patient’s underlying condition. AEs can occur in any healthcare setting, including emergency care settings. Their consequences for patients are usually serious, including prolonged hospitalization, disability, or even death [4, 5]. Studies have shown that AEs occur frequently in Emergency Departments (EDs), with rates ranging from 5.5% to 27.3% of patient visits. However, many AEs remain unreported, with estimates suggesting that only 2–4% of all AEs are reported [6, 7]. Ways to prevent AEs have been proposed in the past, and the surest way is through protocols and guidelines. These guidelines can ensure that patients receive prompt and suitable care, lowering the chance of AEs [8]. Additionally, emergency care providers are encouraged to prioritize communication and teamwork. This is to ensure everyone on the team communicates effectively to give the patient the highest quality care possible. Communication about errors in the workplace is mostly through formalized adverse event reporting (AER) [9, 10].
In EDs, AER is a vital process as it helps to identify and prevent errors, improve patient safety, and ultimately save patients’ lives. This is due to the chaotic nature of these settings. Furthermore, AER can also be used to identify and correct process inefficiencies and reduce the overall cost of care [11, 12]. The challenge of AER is underreporting caused by a lack of or inadequate awareness among healthcare providers. This is caused by fear of retribution or litigation and a lack of standardized reporting procedures. To improve this phenomenon of underreporting, emergency care providers are, therefore, tasked with taking steps to prevent adverse events from occurring [13].
Among the most important approaches to curtailing AEs is a thorough review of the incident. This is to identify any contributing factors and prevent similar events in the future [14]. These steps may include changes to protocols or guidelines, additional training for staff, or changes to the physical environment of the emergency care setting. Healthcare providers have also received regular education and training on AER, including the importance of reporting, how to recognize AERs, and the steps involved in reporting [15, 16]. Additionally, most EDs have adopted standardized reporting procedures such as electronic reporting systems to ensure all AEs are reported consistently and accurately. These measures have improved non-punitive reporting systems and open communication among healthcare providers and have also helped in identifying trends and areas for improvement in patient care [17, 18].
Despite all these measures, few studies have reported on interventions to improve AER in the literature, and their effectiveness remains largely unknown. Patients have the potential to be an invaluable source of information concerning patient safety incident reporting, but historically, efforts to learn from incident reports have been concentrated on staff-led reporting systems. Some researchers contend that patients are in a unique position to influence the efficacy and safety of their care, and recent studies have shown the viability and benefits of patient reporting safety incidents in healthcare settings [19]. This review will, therefore, review studies that investigated intervention used in improving AER in EDs and their effectiveness, centering on both staff-led reporting systems and patient-led interventions.
Method
Protocol registration and reporting
This protocol has been registered in the Prospective Register of Systematic Review (PROSPERO) database with registration (CRD42023414795). The review will be conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) guidelines [20] as detailed in Table 1. The paper that will present the results from this review will include any modifications to the review strategy.
Table 1: PRISMA 2020 checklist.
Eligibility criteria
Inclusion criteria
The review will be done based on the PICOS strategy. Randomised-controlled Trials (RCTs) and Single-arm trial studies that evaluate interventions or programmes aimed at enhancing AER in the EDs will be included in the review.
Population. Empirical, peer-reviewed studies reporting on interventions targeting the improvement of AER in adults and children treated in the EDs will be considered for inclusion irrespective of the country of origin and/or articles that should have been published in 2000. This is justified by the fact that attention to developing systems, tools or interventions to address the challenges of AEs started around the year 2000 [21].
Interventions. The interventions of interest will be interventions targeting the improvement of the reporting of AEs in the EDs. Articles that describe specific interventions on AER.
Comparison. The comparison group will be EDs without interventions for AER.
Outcomes. The primary outcome of interest will be the number and types of AEs reported in the EDs.
Study design. The review will take into account AER interventions and programme reported in RCTs and single-arm trials.
Exclusion criteria
Books, editorials, commentaries, newspapers, unpublished articles, and theses will be excluded from the study. If the article reports the effect of the intervention outside the ED such as in psychiatric homes, geriatric homes, outpatient departments, intensive care units, medical-surgical management units etc, it will be excluded from the review.
Databases and search strategy
The EMBASE Thesaurus (Emtree), Medical Subject Headings (MeSH), and text words will be used to create literature search techniques. Following a preliminary limited search of CINAHL, EMBASE, and Medline, an analysis of the text words found in the article’s text and abstract as well as its index terms will be conducted. Table 2 is the list of keywords for the search, and it will be categorised into three concepts: emergency department with keywords ‘emergency room’, ‘emergency care setting’, and ’medical crises unit’; adverse events, with terms ‘sentinel events’, ‘errors’, ‘incidents’, ‘medication errors’, ‘patient safety incidents’, ‘adverse effects’, ‘medical errors’; interventions with keywords ‘strategies’, ‘programme’, and ‘best practices’. Keywords in each category will be connected with the following Boolean operators: OR, AND, NOT. This will help us in designing a search strategy specific to each data source. All included databases will be searched using the chosen keywords and index phrases. Additionally, the selected reports and reference lists of identifiable reports will be manually searched for other studies. In addition to CINAHL, EMBASE and Medline, the Cochrane Reviews Library, Scopus, OVID, ScienceDirect and Web of Science will all be included in the complete search sources. To find further papers, reference lists of pertinent articles will also be reviewed. Additionally, previous systematic reviews on a related subject will be investigated to identify potential publications for inclusion.
Table 2: Search strategy for CINAHL.
Study selection
All identified studies will be exported into EndNote X9 reference management software after the initial search is finished, and duplicates will be removed. Two independent reviewers (CAP and JB) will undertake title and abstract screening separately. Full-text studies that meet inclusion criteria will be retrieved and critically reviewed by two authors. Any discrepancies identified at the full-text level will be examined by the third and fourth reviewers (AMAO and AAK).
Data extraction and management
The data extraction form will be designed based on the characteristics of the interventions included in the study. Two independent reviewers (CAP and JB) will extract data from the papers included in the review from the Joanna Briggs Institute’s System for the Unified Management, Assessment and Review of Information (JBI SUMARI) platform. The data extracted will include specific details about the study, methods, nature of the intervention, and outcomes of interest to the review question and specific objectives. The reviewers will discuss any differences to reach a consensus, or with a third and fourth reviewers. Each included RCT and single-arm trial will have its risk of bias determined using the second iteration of the Cochrane risk of bias instrument for randomized trials (RoB 2). Using the RoB 2 tool, six domains will be evaluated: bias resulting from the randomization process, bias resulting from deviations from the intended intervention, bias arising from the lack of outcome data, bias in the measurement of the outcome, bias in the choice of the reported result, and overall bias. Each domain’s assessment of bias risk will be indicated as “low risk”, “high risk”, or “some concerns”. After that, each study’s total bias risk will be determined [22].
Quality assessment/study risk of bias assessment
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) will be used to grade the overall quality of evidence [23, 24]. Four levels of evidence—“very low”, “low”, “moderate”, and “high”—will be offered along with the results to indicate how confident a person should be in the effect estimates. In the GRADE evaluation, terms like “risk of bias”, “inconsistency”, “indirectness”, “impression”, and “publication bias” might decrease the magnitude of an impact, while terms like “large magnitude of effect”, “all residual confounding”, and “dose-response gradient” can increase the level of certainty.
Again, two independent reviewers will critically appraise the RCTs and single-arm trials to evaluate the selected studies [25]. Any disagreement between the reviewers will be first discussed and if consensus is not achieved, a third independent reviewer will be consulted.
Effect measures
The correlation coefficient (r) will be used to compute the effect size index [with a 95% confidence interval (CI)]. When r is not available, other statistics (standardized beta coefficients, t-values) will be used to calculate the effect size using the following formulas:
where λ = 1 when β is nonnegative and 0 when β is negative
Ethics consideration
A review of already published literature will serve as the foundation for the current study, hence institutional review board approval is not necessary.
Data synthesis
The Template for Intervention Description and Replication (TIDieR) checklist according to [26] will be used to present the nature of the AEs reporting interventions. Where possible, papers will be incorporated into a statistical meta-analysis using the JBI SUMARI platform. With 95% confidence intervals surrounding the summary estimate, effect sizes will be shown as a percentage (odd ratios for dichotomous data or weighted mean differences for continuous data). Using methods from Borenstein [27], the appropriate variance, or standard error, will be computed for every study by changing the correlation coefficient to the Fisher’s z scale. Cohen’s recommendations will be used to estimate the effect size correlations and interpret them as r ≤ .10—very small effect size; 0.10 > r < 0.3—small, 0.3 ≤ r < 0.5 –moderate, and r ≥ 0.5—large.
The chi-squared and I^2^ tests, which are widely used in statistics, will be used to evaluate heterogeneity. The greater the heterogeneity between the studies, the higher the I^2^ value/percentage. If I^2^ is 50%, a fixed effects model will be used; if I^2^>50%, a random effects model will be employed to estimate the heterogeneity. Only results with a p<0.05 will be considered statistically significant.
Based on the recommendations made by Tufanaru et al [28] and Munn et al [29], the meta-analysis method and model (random or fixed effects) will be chosen. Where there is enough data to examine variations in settings and AE reporting, subgroup analysis will be performed. Sensitivity studies will be carried out to evaluate choices made concerning incomplete data or limited sample size. The presented results will be used to determine whether there is high heterogeneity. Meta-analysis will not be done if the degree of heterogeneity between studies is too high. The results will be provided in narrative form, with tables and figures where needed to help with data presentation, when statistical pooling is not available.
Fig 1 is the PRISMA 2020 flow diagram for new systematic reviews that will be used to present the study identification, screening and inclusion. The relationship and conclusions both within and between the selected studies will be explored in the narrative synthesis
PRISMA 2020 flow diagram for new systematic reviews.
Reporting bias assessment
If there are ten or more studies available, funnel plots will be used to investigate the possibility of publication bias. The statistical tests for funnel plot asymmetry like the Egger test and Begg test will be run where applicable [30, 31].
Discussion
Adverse event reporting is a critical process in healthcare systems that helps to identify and address potential patient safety issues. However, AEs are often underreported, leading to the potential for preventable harm to patients going unidentified. In the context of emergency care, interventions improve AER by addressing the barriers to reporting and encouraging healthcare professionals to report AEs.
A key intervention that has been shown to improve AER is the implementation of a patient safety culture. A patient safety culture supports the reporting of AEs and the improvement of patient safety. Hospitals with a positive patient safety culture had a higher rate of AER compared to hospitals with a negative culture [32, 33]. Specifically, hospitals with a positive culture had a median of 86.5% of AER, while hospitals with a negative culture had a median of 47.2% of AER.
Additionally, the use of electronic reporting systems has been identified as an intervention that can improve AER. Electronic reporting systems make reporting easier and more efficient for healthcare professionals to report AEs [34]. The use of an electronic reporting system increased AER by 6.2-fold compared to paper-based reporting systems. Specifically, the electronic reporting system was associated with an increase in the reporting of medication errors, falls, and pressure ulcers [35, 36].
Furthermore, education and training of healthcare professionals on the importance of AER and the reporting process can also improve reporting rates. An educational intervention aimed at increasing reporting rates of medication errors resulted in a significant increase by healthcare professionals from 10.7% to 54.9% after the educational intervention [37–39].
The ED presents their challenges of increased workload, over-crowding and chaotic nature of service delivery. More attention is paid to the survival of patients instead of patient safety of the patients [40, 41]. Even though these interventions have helped in improving AER rates and identifying potential safety issues in healthcare in general, interventions in emergency care settings are low. We expect that this study will generate interest regarding the interventions in the emergency care setting, and will contribute to the development of effective interventions to address the challenges of AE reporting to promote organizational learning.
A potential limitation that we foresee relates to the broad nature of the AE concept. The focus on interventions may also imply that qualitative data which could explain the subjective aspect of AER will be lacking. The reviewers will establish specific inclusion and exclusion criteria to narrow the focus. Thus, the reviewers will clearly define the scope and types of AEs included in the review. Another limitation will be potentially reporting only positive results published than negative or null results, potentially skewing the review’s findings. The researchers intend using statistical methods (e.g., funnel plots) to assess and adjust for publication bias. Again, the reviewers will assess the quality of each study using validated tools (e.g., Cochrane risk-of-bias tool) and perform sensitivity analyses to evaluate the study quality and risk of bias on the overall findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. Patient safety incident reporting and learning systems: technical report and guidance. 2020 [cited 2024 May 9]; Available from: https://apps.who.int/iris/bitstream/handle/10665/334323/9789240010338-eng.pdf
- 2WHO. World alliance for patient safety: forward programme 2005. 2004.
- 3WHO. Patient safety: making health care safer. World Health Organization; 2017.
- 4Kakemam E, Kalhor R, Khakdel Z, Khezri A, West S, Visentin D, et al. Occupational stress and cognitive failure of nurses and associations with self-reported adverse events: A national cross-sectional survey. J Adv Nurs. 2019;75(12):3609–18. doi: 10.1111/jan.14201 31531990 · doi ↗ · pubmed ↗
- 5Shojania KG, Marang-van de Mheen PJ. Identifying adverse events: reflections on an imperfect gold standard after 20 years of patient safety research. Vol. 29, BMJ Quality & Safety. BMJ Publishing Group Ltd; 2020. p. 265–70.10.1136/bmjqs-2019-00973132066571 · doi ↗ · pubmed ↗
- 6Regina ML, VecchiéA, Bonaventura A, Prisco D. Patient Safety in Internal Medicine. Textb Patient Saf Clin Risk Manag. 2021;213–52.36315754 · pubmed ↗
- 7Slawomirski L, Klazinga N. The economics of patient safety: from analysis to action. 2022.
- 8Wood C, Chaboyer W, Carr P. How do nurses use early warning scoring systems to detect and act on patient deterioration to ensure patient safety? A scoping review. Int J Nurs Stud. 2019;94:166–78. doi: 10.1016/j.ijnurstu.2019.03.012 31002971 · doi ↗ · pubmed ↗