Diffuse Maculopapular Dermatitis Associated With Leuprorelin Acetate Androgen Deprivation Therapy
Kwabena Boahen Asare, Nirav S Kapadia

TL;DR
An 80-year-old man developed a skin rash after receiving leuprolide acetate for prostate cancer, which was successfully treated with prednisone.
Contribution
This case report highlights a rare dermatological side effect of leuprolide acetate and its successful management.
Findings
The patient developed diffuse maculopapular dermatitis after multiple leuprolide injections.
Prednisone treatment resolved the dermatitis without long-term effects.
The case emphasizes the need for clinicians to recognize and address ADT-related skin reactions.
Abstract
Androgen deprivation therapy (ADT) is one of the effective treatment methods for prostate cancer, often used with radiation therapy. Among the key ADT agents is leuprolide, a synthetic gonadotropin-releasing hormone agonist, which effectively suppresses testosterone production which is a requisite for the growth and division of prostate cancer cells. However, leuprolide is associated with several well-known side effects and less common dermatological reactions. In this case, we present an 80-year-old male patient with stage IIB prostate cancer who developed diffuse maculopapular dermatitis following leuprolide acetate ADT. The patient first experienced mild dermatitis following the fifth monthly 7.5 mg leuprolide injection before it developed into a general body rash after six injections. The dermatitis manifested on the patient’s arms, thighs, calves, dorsum, and back of hands but…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2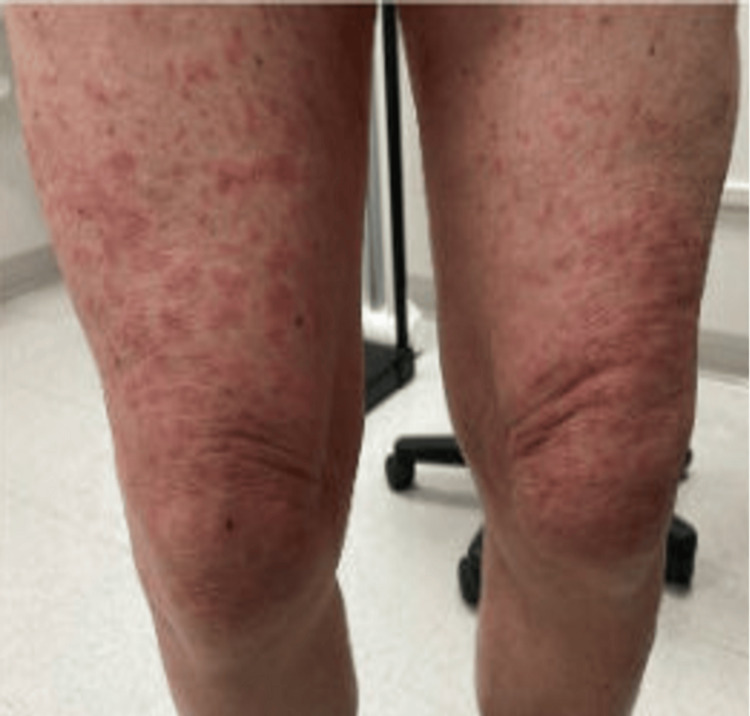 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemotherapy-related skin toxicity · Prostate Cancer Treatment and Research · Cancer Diagnosis and Treatment
Introduction
Androgen deprivation therapy (ADT) is a key treatment method for the treatment of patients with advanced or metastatic prostate cancer and may be used with other treatment methods such as radiotherapy [1-3]. Among the effective ADT agents is leuprolide, also known as leuprorelin acetate, a synthetic agonist analog of gonadotropin-releasing hormone (GnRH). Leuprolide functions by suppressing the production of testosterone, which is crucial for prostate cancer cell growth [4]. By reducing testosterone production, leuprolide stops or slows down the advancement of prostate cancer, particularly in cases where the cancer is hormone-sensitive [5,6]. Common side effects of leuprolide ADT include fatigue, hot flashes, sexual side effects, susceptibility to metabolic disorders, muscle loss, weakness, osteoporosis, and coronary heart disease [7-9]. While cases of dermatological reactions associated with leuprolide have been reported, papular eruptions remain widely underreported [9-20]. Here, we present an unusual case of a patient exhibiting diffuse maculopapular dermatitis associated with leuprorelin acetate ADT.
Case presentation
An 80-year-old patient diagnosed with stage IIB, unfavorable, intermediate-risk prostate cancer underwent leuprorelin acetate ADT, receiving 7.5 mg doses of leuprorelin every month. Following the fifth injection of leuprorelin acetate, the patient developed mild dermatitis on the arms. Given its mild nature, no further management was recommended. Two days following the next injection, however, the rash developed into a diffuse maculopapular dermatitis on the patient’s arms, thighs, calves, dorsum, and back of his hands (Figures 1-4). However, his abdomen, face, and neck were spared.
Photograph of maculopapular dermatitis after the fifth intramuscular injection of 7.5 mg dose of leuprolide. The image shows dermatitis on the patient’s dorsum.
Photograph of maculopapular dermatitis after the fifth intramuscular injection of 7.5 mg dose of leuprolide. The image shows dermatitis on the patient’s calves.
Photograph of maculopapular dermatitis after the fifth intramuscular injection of 7.5 mg dose of leuprolide. The image shows dermatitis on the patient’s thighs.
Photograph of maculopapular dermatitis after the fifth intramuscular injection of 7.5 mg dose of leuprolide. The image shows dermatitis at the back of the patient’s hands.
Given the pruritic nature of the dermatitis, the patient was given prednisone 20 mg, twice daily for three weeks, followed by a rapid taper. Over the course of the steroid treatment, dermatitis and pruritus improved and eventually healed with no long-term visible sequalae. No further injections of leuprorelin acetate were planned or administered.
Discussion
Prostate cancer is one of the most commonly diagnosed tumors and ranks as the sixth leading cause of cancer-related deaths among men [1]. Standard treatment methods for prostate cancer include surgery and radiation therapy, the latter of which is often combined with ADT either in the short (e.g., 4-6 months) or long (12-36 months) term [1,2]. The choice of treatment depends on various factors, including cancer stage, the patient’s overall health and preferences, and potential side effects [3]. In this case, the patient received planned short-term neoadjuvant and concurrent ADT, alongside radiotherapy to his pelvis and prostate.
While the efficacy of leuprorelin acetate in suppressing testosterone production and slowing the progression of prostate cancer is well-established [4-8], its potential dermatological side effects, particularly diffuse maculopapular dermatitis, are less recognized and underreported in clinical practice [9-20].
The onset of dermatitis in our patient following the fifth leuprorelin acetate injection highlights the essence of monitoring patients undergoing ADT for potential adverse reactions. Although the initial rash was mild, its progression to diffuse maculopapular dermatitis necessitated intervention to alleviate symptoms and prevent further complications. Systemic steroidal treatment with prednisone proved effective in managing diffuse dermatitis, leading to significant improvement and eventual resolution of the skin reactions.
This case contributes to the growing body of evidence documenting dermatological manifestations associated with leuprorelin acetate ADT. While previous reports have documented papular eruptions linked to leuprorelin acetate, our case highlights a rare development of diffuse, symptomatic maculopapular dermatitis, expanding the spectrum of dermatological adverse effects attributed to this medication.
The underlying mechanisms behind the development of dermatitis in response to leuprorelin acetate remain unclear and warrant further investigation. It is plausible that immune-mediated processes or hypersensitivity reactions may play a role in the pathogenesis of dermatological side effects associated with this medication or, more likely, one of its components. A previous report, for instance, established that papuloerythroderma, a skin condition related to maculopapular dermatitis, is linked to eosinophil invasion, and mediated by T-helper 2 cells [20].
Conclusions
This case highlights the importance of recognizing and managing dermatological adverse effects associated with drug treatments. Clinicians should remain vigilant for such reactions and be prepared to intervene promptly to optimize patient outcomes. Additionally, systematic reporting of adverse drug reactions and further research are crucial for enhancing patient safety and improving our understanding of drug-related dermatological manifestations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prostate cancer treatment and work: a scoping review Am J Mens Health Yu Ko WF Oliffe JL Bottorff JL 1557988320979257142020 https://doi.org/10.1177/15579883209792573330567810.1177/1557988320979257 PMC 7734520 · doi ↗ · pubmed ↗
- 2Prostate cancer Lancet Sandhu S Moore CM Chiong E Beltran H Bristow RG Williams SG 107510903982021 http://doi:https://doi.org/10.1016/S 0140-6736(21)00950-83437097310.1016/S 0140-6736(21)00950-8 · doi ↗ · pubmed ↗
- 3Intermediate-risk prostate cancer: stratification and management Eur Urol Oncol Preisser F Cooperberg MR Crook J 27028032020 https://doi.org/10.1016/j.euo.2020.03.0023230347810.1016/j.euo.2020.03.002 · doi ↗ · pubmed ↗
- 4Leuprolide: a gonadotropin-releasing hormone analog for the palliative treatment of prostatic cancer Drug Intell Clin Pharm Wojciechowski NJ Carter CA Skoutakis VA Bess DT Falbe WJ Mickle TR 746751201986 https://doi.org/10.1177/106002808602001001242981510.1177/106002808602001001 · doi ↗ · pubmed ↗
- 5Leuprorelin depot injection: patient considerations in the management of prostatic cancer Ther Clin Risk Manag Abouelfadel Z Crawford ED 51352642008 https://doi.org/10.2147/tcrm.s 68631872884710.2147/tcrm.s 6863 PMC 2504071 · doi ↗ · pubmed ↗
- 6Six-month depot formulation of leuprorelin acetate in the treatment of prostate cancer Clin Interv Aging Sethi R Sanfilippo N 25926742009 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 2697591/1955409710.2147/cia.s 4885 PMC 2697591 · doi ↗ · pubmed ↗
- 7Addition of enzalutamide to leuprolide and definitive radiation therapy is tolerable and effective in high-risk localized or regional nonmetastatic prostate cancer: results from a phase 2 trial Adv Radiat Oncol Shee K de la Calle CM Chang AJ 10094172022 https://doi.org/10.1016/j.adro.2022.1009413584755010.1016/j.adro.2022.100941 PMC 9280039 · doi ↗ · pubmed ↗
- 8Testosterone therapy among prostate cancer survivors Sex Med Rev Nguyen TM Pastuszak AW 37638842016 https://doi.org/10.1016/j.sxmr.2016.06.0052747499510.1016/j.sxmr.2016.06.005PMC 5026903 · doi ↗ · pubmed ↗