Incidence of Acute Kidney Injury Post Transcatheter Aortic Valve Implantation (TAVI): A Single-Center Experience
Khalid Makki, Fatemah I Ammar, Jose Andres Fernandez, Muhnnad A AlGhamdi, Abdulkareem M Alturkistani, Rahaf A Hubayni, Elaf I Khahwry

TL;DR
This study reports that 10.7% of patients developed acute kidney injury after a heart valve procedure called TAVI, with risk factors including hyperlipidemia and prior kidney disease.
Contribution
The study provides a single-center analysis of AKI incidence after TAVI, highlighting risk factors specific to this patient population.
Findings
11 out of 103 patients (10.7%) developed AKI within seven days of TAVI.
Patients with hyperlipidemia and prior kidney disease were at higher risk for AKI.
The study had limitations due to its retrospective design and small sample size.
Abstract
Introduction: Transcatheter aortic valve implantation (TAVI) has dramatically changed the approach to treating aortic stenosis, particularly for patients unsuitable for surgical aortic valve replacement. Nevertheless, the possibility of quick deterioration of kidney function, known as acute kidney injury (AKI), post operation is considered one of the complications. Objectives: The study aimed to determine the incidence of AKI in adults post TAVI. Methods: This retrospective cohort study focuses on patients who underwent the TAVI procedure at the King Faisal Cardiac Center at the Ministry of National Guard Health Affairs (MNGHA) in Jeddah, Saudi Arabia, from May 2016 to December 2022. Acute kidney injury post TAVI was defined based on RIFLE (Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease) criteria. Chi-square tests and independent sample t-tests were used…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
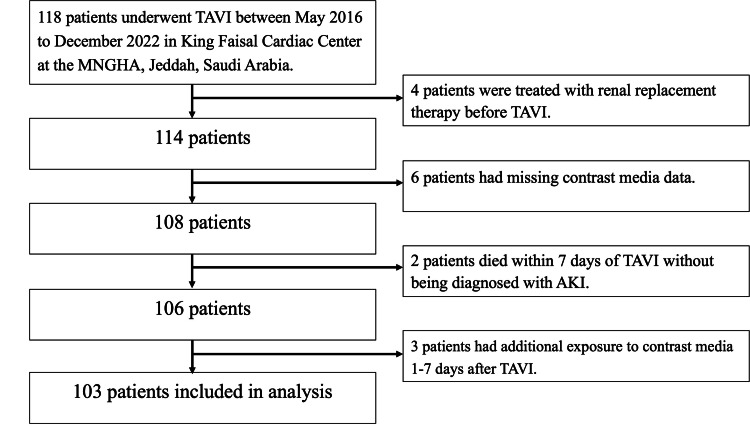 Figure 1
Figure 1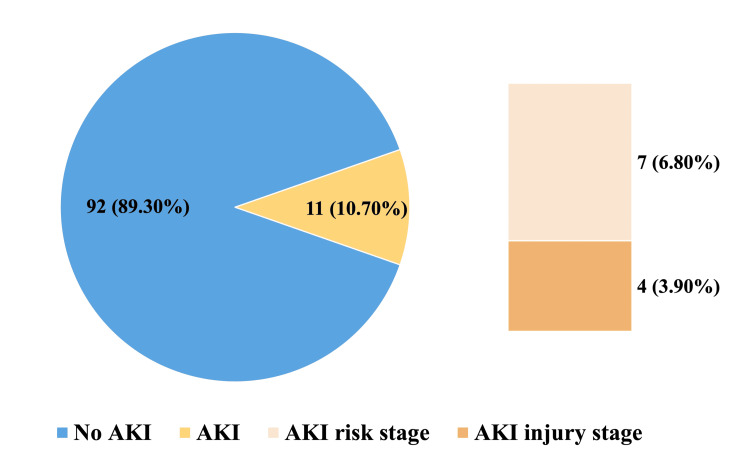 Figure 2
Figure 2| Clinical data | AKI (-); n (%) | AKI (+); n (%) | p-value | |
| 1. Gender | Male | 48 (52.2%) | 4 (36.4%) | 0.322 |
| Female | 44 (47.8%) | 7 (63.6%) | ||
| 2. Age (years) mean ± SD | 78.66 ± 9.24 | 82.18 ± 7.82 | 0.229 | |
| 3. Body mass index (kg/m2) mean ± SD | 30.79 ±7.65 | 32.20 ± 4.99 | 0.421 | |
| 4. Diabetes mellitus | Yes | 59 (64.1%) | 6 (54.5%) | 0.529 |
| No | 33 (35.9%) | 5 (45.5%) | ||
| 5. Hypertension | Yes | 75 (81.5%) | 11 (100.0%) | 0.204 |
| No | 17 (18.5%) | 0 (0.0%) | ||
| 6. Hyperlipidemia | Yes | 66 (71.7%) | 9 (81.8%) | 0.025 |
| No | 23 (25.0%) | 0 (0.00%) | ||
| Not documented | 3 (3.3%) | 2 (18.2%) | ||
| 7. Anemia | Yes | 41 (44.6 %) | 6 (54.5%) | 0.543 |
| No | 51 (55.4%) | 5 (45.5%) | ||
| 8. Smoking | Yes | 7 (7.6%) | 0 (0.0%) | 0.802 |
| No | 51 (55.4%) | 7 (63.6%) | ||
| Not documented | 27 (29.3%) | 3 (27.3%) | ||
| Ex-smoker | 7 (7.6 %) | 1 (9.1%) | ||
| 9. Heart failure | Yes | 26 (28.3%) | 6 (54.5%) | 0.092 |
| No | 66 (71.7%) | 5 (45.5%) | ||
| 10. Kidney disease | None | 73 (79.3%) | 2 (18.2%) | <0.001 |
| History of AKI | 2 (2.2%) | 0 (0.0%) | ||
| CKD | 15 (16.3%) | 9 (81.8%) | ||
| Others | 2 (2.2%) | 0 (0.0%) | ||
| 11. Malignancy | Yes | 14 (15.2%) | 3 (27.3%) | 0.385 |
| No | 77 (84.8%) | 8 (72.7%) | ||
| 12. Infection | Yes | 8 (8.7%) | 2 (18.2%) | 0.289 |
| No | 84 (91.3%) | 9 (81.8%) | ||
| 13. Bleeding | Yes | 2 (2.2%) | 1 (9.1%) | 0.290 |
| No | 89 (97.8%) | 10 (90.9%) | ||
| 14. Multi-organ disease | Yes | 8 (8.7%) | 2 (18.2%) | 0.289 |
| No | 84 (91.3%) | 9 (81.8%) | ||
| 15. Nephrotoxic drugs | None | 35 (38.0%) | 4 (36.4%) | 0.837 |
| NSAIDs | 40 (43.5%) | 4 (36.4%) | ||
| Antimicrobial agents | 4 (4.3%) | 0 (0.0%) | ||
| Chemotherapeutic agents | 4 (4.3%) | 1 (9.1%) | ||
| Antimicrobial and chemotherapeutic agents | 1 (1.1%) | 0 (0.0%) | ||
| Others drugs | 8 (8.7%) | 2 (18.2%) | ||
| Laboratory test | AKI (-) | AKI (+) | p-value | |
| Hemoglobin (gm/dL), mean (SD) | Pre-TAVI | 12.25 (1.74) | 11.93 (1.16) | 0.569 |
| Procedure date | 12.97 (10.64) | 11.60 (1.42) | 0.673 | |
| Post-TAVI | 11.04 (1.74) | 10.56 (1.51) | 0.383 | |
| White blood count (*10^9/L), mean (SD) | Pre-TAVI | 6.91 (1.81) | 7.74 (1.54) | 0.154 |
| Procedure date | 8.18 (3.23) | 10.78 (5.52) | 0.023 | |
| Post-TAVI | 9.10 (2.73) | 12.26 (4.49) | 0.001 | |
| Platelet (*10^9/L), mean (SD) | Pre-TAVI | 241.46 (67.85) | 255.27 (77.12) | 0.531 |
| Procedure date | 235.45 (63.48) | 232.55 (81.15) | 0.890 | |
| Post-TAVI | 206.01 (81.66) | 186.55 (87.00) | 0.460 | |
| Sodium (mmol/L), mean (SD) | Pre-TAVI | 136.17 (3.58) | 136.91 (2.30) | 0.508 |
| Procedure date | 136.16 (3.52) | 136.81 (3.62) | 0.567 | |
| Post-TAVI | 133.86 (12.09) | 135.61 (3.78) | 0.636 | |
| Potassium (mmol/L), mean (SD) | Pre-TAVI | 4.38 (0.47) | 4.64 (0.61) | 0.106 |
| Procedure date | 4.48 (1.96) | 4.49 (0.62) | 0.992 | |
| Post-TAVI | 4.29 (0.48) | 4.49 (1.14) | 0.570 | |
| Albumin (g/L), mean (SD) | Pre-TAVI | 37.14 (4.26) | 36.50 (4.25) | 0.661 |
| Procedure date | 35.42 (3.99) | 35.00 (4.57) | 0.785 | |
| Post-TAVI | 34.32 (3.48) | 30.89 (5.01) | 0.078 | |
| Serum creatinine (umol/L), mean (SD) | Pre-TAVI | 88.52 (28.78) | 116.82 (43.86) | 0.061 |
| Procedure date | 84.83 (26.86) | 115.09 (37.35) | 0.001 | |
| Post-TAVI | 83.91 (29.10) | 164.36 (77.28) | 0.006 | |
| Blood urea nitrogen (mmol/L), mean (SD) | Pre-TAVI | 9.06 (14.73) | 10.04 (3.55) | 0.828 |
| Procedure date | 7.29 (3.75) | 9.95 (2.82) | 0.025 | |
| Post-TAVI | 8.06 (4.92) | 13.01 (4.94) | 0.002 | |
| Estimated glomerular filtration rate (eGFR), mean (SD) | Pre-TAVI | 69.87 (18.83) | 59.09 (20.30) | 0.078 |
| Procedure date | 71.18 (18.34) | 48.64 (17.81) | < 0.001 | |
| Post-TAVI | 73.72 (19.04) | 34.64 (14.81) | < 0.001 | |
| Prothrombin time (PT) (s), mean (SD) | Pre-TAVI | 12.77 (1.52) | 13.82 (2.56) | 0.212 |
| Procedure date | 13.27 (1.86) | 14.09 (1.51) | 0.164 | |
| Post-TAVI | 13.64 (3.93) | 16.91 (12.68) | 0.415 | |
| Partial thromboplastin time (PTT) (s), mean (SD) | Pre-TAVI | 31.99 (5.51) | 34.82 (5.76) | 0.112 |
| Procedure date | 37.37 (23.05) | 51.18 (35.72) | 0.081 | |
| Post-TAVI | 32.87 (7.86) | 34.00 (7.94) | 0.654 | |
| International normalised ratio (INR), mean (SD) | Pre-TAVI | 1.13 (0.16) | 1.23 (0.16) | 0.013 |
| Procedure date | 1.09 (0.13) | 1.21 (0.24) | 0.072 | |
| Post-TAVI | 1.17 (0.33) | 1.49 (1.17) | 0.389 | |
| AKI (-); n (%) | AKI (+); n (%) | p-value | ||
| Hydration type | Oral | 8 (100.0 %) | 0 (0.0%) | 0.795 |
| Intravenous (IV) | 33 (86.8 %) | 5 (13.2%) | ||
| Both | 51 (89.5 %) | 6 (10.5 %) | ||
| Intravenous hydration type | None | 2 (100 %) | 0 (0.0 %) | 0.231 |
| 0.9% sodium chloride (NaCl) | 3 (75.0 %) | 1 (25.0 % | ||
| Isotonic saline administered 12 hours before the procedure | 64 (92.8 %) | 5 (7.2 %) | ||
| Others | 23 (82.1 %) | 5 (17.9 %) | ||
| Hydration time | Pre-TAVI | 64 (92.8 %) | 5 (7.2 %) | 0.121 |
| Post-TAVI | 15 (88.2 %) | 2 (11.8%) | ||
| Both | 13 (76.5 %) | 4 (23.5 %) | ||
| Contrast media volume administered, mean± SD | 192.62 ± 82.20 | 209.36 ± 87.75 | 0.527 | |
| Mehran score | Low risk (0 to 5) | 21 (100.0%) | 0 (0.0%) | 0.120 |
| Moderate risk (6 to 10) | 33 (91.7 %) | 3 (8.3 %) | ||
| High risk (11 to 15) | 26 (83. 9%) | 5 (16.1 %) | ||
| Very high risk (≥16) | 12 (80.0 %) | 3 (20.0 %) | ||
| Procedural Data | AKI (-); n (%) | AKI (+); n (%) | p-value | |
| Indication of TAVI | Severe aortic valve stenosis | 77 (88.5%) | 10 (11.5 %) | 1.00 |
| Severe symptomatic aortic valve stenosis | 13 (92.9%) | 1 (7.1 %) | ||
| Severe symptomatic aortic valve prosthesis degenerative | 2 (100.0 %) | 0 (0.0 %) | ||
| Type of anesthesia | General anesthesia | 83(88.3%) | 11 (11.7%) | 0.592 |
| Local anesthesia with sedation | 9 (100.0%) | 0 (0.0 %) | ||
| Type of valve | Evolut-R™(Medtronic) | 79 (94.0%) | 5 (6.0%) | 0.005 |
| SAPIEN-3™ (Edwards Lifesciences) | 10 (71.4 %) | 4 (28.6 %) | ||
| ACURATE-Neo™ (Boston Scientific) | 3 (60.0 %) | 2 (40.0 %) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Imaging and Diagnostics · Atrial Fibrillation Management and Outcomes
Introduction
Acute kidney injury (AKI) is a condition characterized by the rapid deterioration of kidney function, leading to electrolyte and volume imbalances [1]. Alongside AKI, another common condition in the elderly population is aortic valve stenosis. Aortic stenosis, characterized by the narrowing of the aortic valve, typically occurs as a result of the aging process. However, it can also result from congenital defects or, rarely, rheumatic fever [2]. Recently, transcatheter aortic valve implantation (TAVI) has emerged as a viable alternative for patients with severe aortic stenosis who are considered ineligible for conventional surgical aortic valve replacement [3]. The American Heart Association defines TAVI as a minimally invasive percutaneous procedure that helps to improve a damaged aortic valve by replacing it through an endovascular technique [4]. However, it is crucial to note that AKI following TAVI is a recognized complication [5]. Post-contrast AKI (PC-AKI) is a well-established risk following procedures involving contrast, such as TAVI. The variation in the reported incidences of AKI post TAVI is influenced by factors such as the absence of a standardized definition, different routes of access, investigation tools, and comorbidities. The reported incidence of AKI post TAVI varies widely due to different definitions and patient factors [6, 7]. These causes influence the variation in the reported incidence of AKI, which ranges between 8.3% and 58% [7]. Another study by Alassar et al. [8] found an AKI incidence rate after TAVI of 12.3% that resolved before patients’ discharge from the hospital. Also, AKI occurred in 13.8% of TAVI patients in Haase-Fielitz et al. [9]. Given the common occurrence and severe consequences of AKI complicating TAVI, a standardized PC-AKI definition is crucial [10]. The RIFLE (Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease) criteria use estimated glomerular filtration rate (eGFR) changes, adjusted for age and gender, to estimate AKI incidence and identify early-stage patients [11]. The Kidney Disease Improving Global Outcomes (KDIGO) criteria define AKI as a 0.3 mg/dL or 1.5-1.9 times increase in serum creatinine (sCr) from baseline, providing reliable incidence and outcome estimates [12-14].
Predictive factors for AKI following TAVI include age, diabetes mellitus, heart failure, atherosclerotic burden, previous stroke, and chronic kidney disease (CKD) [6]. Acute kidney injury post TAVI can lead to serious complications such as permanent renal dysfunction requiring renal replacement therapy, heart attack, life-threatening hemorrhage, and mortality [15,16]. Despite the risks, certain studies have found TAVI to be safe when specific techniques are employed [17, 18]. Procedure-related factors that increase the risk of PC-AKI include the type, volume, and route of contrast administration, as well as the frequency of injections. Peri-procedural intravenous hydration remains a key preventive strategy [19]. Effective prevention involves identifying at-risk patients and administering rigorous hydration with non-ionic contrast [20]. Healthcare practitioners should evaluate each patient's risk to determine the appropriate hydration approach [20, 21]. This research aimed to estimate the occurrence of AKI in adult patients who underwent the TAVI procedure.
Materials and methods
Study population
This study utilized a retrospective cohort design to estimate the incidence of AKI in adult patients post TAVI procedure in the King Faisal Cardiac Center in the Ministry of National Guard Health Affairs (MNGHA) at King Abdulaziz Medical City (KAMC), Jeddah, Saudi Arabia. The study included 103 adult patients. The patient selection flowchart is shown in Figure 1.
Patient selection flowchartTAVI: transcatheter aortic valve implantation; AKI: acute kidney injury; MNGHA: Ministry of National Guard Health Affairs
Inclusion and exclusion criteria
This study included adult patients from the King Faisal Cardiac Center at MNGHA who were 14 years of age or older and had undergone the TAVI procedure during the designated study period. At MNGHA, patients who are 14 years old or older are considered adults. Patients were excluded if they had a history of exposure to contrast medium within the first seven days post TAVI if any pre- or postoperative measurement of sCr or contrast medium volume was missing, or if they had died within the first seven days. Additionally, patients who had a kidney transplant were on maintenance hemodialysis or peritoneal dialysis or had preexisting moderate to severe kidney damage stage 3b CKD and further, defined as a decreased eGFR of less than 30 mL/min/1.73 m^2^ were also excluded [22].
Data collection
Data were collected from the medical records department through the Best Care system for all patients in the cardiology department who underwent the TAVI procedure from May 2016 to December 2022. Demographic data and sCr levels of each participant were used to calculate eGFR using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation (2021) [23]. Acute kidney injury post TAVI was defined based on the RIFLE criteria: the risk stage as sCr increased to 1.5-fold or GFR decreased by >25% from baseline; the injury stage as sCr increased to 2.0-fold or GFR decreased by >50% from baseline; and the failure stage as sCr increased to 3.0-fold or GFR decreased by >75% from baseline, within two to seven days post TAVI [11, 24]. Laboratory data were measured one day before the procedure (pre-TAVI), on the procedure day (procedure date), and seven days after the procedure (post-TAVI). The RIFLE urine output criteria were excluded from defining AKI due to the use of diuretic medication, which may affect the results [11]. Additionally, according to hospital protocol, patients with heart failure received prophylactic hydration with isotonic saline 12 hours before TAVI, while the remaining patients received individualized prophylactic hydration. The Mehran score was used to further classify the risk of contrast-induced nephropathy after TAVI [25].
Statistical analysis
Categorical variables were reported as absolute numbers and percentages and compared using the chi-square test. Continuous data with a normal distribution were reported as the mean and standard deviation (SD) and compared using an independent sample t-test. A p-value lower than 0.05 was considered statistically significant; data were managed and analyzed in IBM SPSS Statistics software for Windows, version 29.0 (IBM Corporation, Armonk, NY).
Results
The study included 103 adult patients, with 92 (89.3%) patients in the AKI (-) group and 11 (10.7%) in the AKI (+) group. Out of the 11 patients with AKI (+), seven (6.8%) patients were in the risk stage, and four (3.9%) patients were in the injury stage. Figure 2 displays the distribution of patients with and without AKI according to the RIFLE criteria.
Distribution of patients with and without AKI according to the RIFLE criteriaAKI: acute kidney injury; RIFLE: Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease
Equations
The calculation of the incidence proportion of patients who are diagnosed with AKI following TAVI procedures is shown below.
\begin{document}\large Incidence\, proportion=\tfrac{Number\, of\, new\, cases\, of\, the\, disease}{Population\, at\, risk\, over\, a\, specified\, time\, period}\times 100\end{document}
\begin{document}\large Incidence\, proportion=\tfrac{AKI\, cases\, (11)}{Total\, population\, at\, risk\, (103)}\times 100=10.7\%\end{document} %
Baseline characteristics
The study included 103 patients, of whom 52 were male and 51 were female. Among the male patients, four (7.7%) out of 52 male patients and seven (13.7%) out of 51 female patients developed AKI. The mean age of patients who developed AKI was 82.18 ± 7.82 years, while the mean age of patients who did not develop AKI was 78.66 ± 9.24 years. The average body mass index (BMI) was 32.20 ±4.99 kg/m^2^ for patients who developed AKI and 30.79 ±7.65 kg/m^2^ for patients who did not develop AKI. In terms of comorbidities, type 2 diabetes mellitus was present in 54.5% of the patients who developed AKI post TAVI; hypertension was present in all patients who developed AKI post TAVI, and dyslipidemia was seen in 81.8%. Six (54.5%) patients had heart failure, and CKD was described in nine (81.8%) patients who developed AKI. The baseline characteristics (Table 1) showed no statistically significant differences between the AKI (-) and AKI (+) groups in terms of gender, age, BMI, diabetes mellitus, hypertension, anemia, smoking, heart failure, malignancy, infection, bleeding, multi-organ disease, and nephrotoxic drugs. However, patients with hyperlipidemia and a history of kidney disease had a significantly higher risk of developing AKI following TAVI. Therefore, those with hyperlipidemia or prior kidney disease are more at risk of developing AKI following TAVI.
Laboratory data
Laboratory data analysis (Table 2) indicated no significant differences in pre-TAVI laboratory tests. However, significant changes were observed in sCr, eGFR, and blood urea nitrogen (BUN) levels on the procedural date and post TAVI. On the TAVI day, sCr (p=0.001), eGFR (p<0.001), and BUN (p=0.025) were significantly affected, and post TAVI, the significance persisted for sCr (p=0.006), eGFR (p<0.001), and BUN (p=0.002). These results suggest that contrast media significantly impacted kidney function, particularly in patients with a history of kidney diseases.
Prophylaxis methods and contrast media data
All patients who underwent TAVI received prophylaxis to prevent kidney damage (Table 3). This involved hydration administered orally, intravenously, or both. The findings indicate that the type of hydration did not significantly affect outcomes for either the AKI (-) or AKI (+) groups (p = 0.795). Additionally, hydration administered before and after contrast media exposure also showed no significant impact on outcomes (p = 0.121). Furthermore, all patients received iodinated iso-osmolar and isotonic contrast media administered intraarterially in the contrast media data. The volume of contrast media administered did not yield a significant outcome (p = 0.527). Also, analyzing the Mehran score for patients categorized as low-risk, moderate-risk, high-risk, and very high-risk showed no significant difference (p = 0.120). Therefore, no significant association was found between the volume of contrast media administered, the Mehran score, and the occurrence of AKI.
Procedural data
The analysis in Table 4 shows that the indication for TAVI in both the AKI (-) and AKI (+) groups did not result in significant differences (p = 1.00). Furthermore, the study determined that the type of anesthesia used had no significant impact on outcomes. The types of valves utilized during the TAVI procedures in our study included the Evolut-R™ (Medtronic, Minneapolis, MN), the ACURATE-Neo™ (Boston Scientific, Marlborough, MA), and the SAPIEN-3™ (Edwards Lifesciences, Irvine, CA). The Evolut-R™ and ACURATE-Neo™ are self-expanding valves, while the SAPIEN-3™ is a balloon-expandable valve. Notably, the type of valve used demonstrated a significant relationship with the occurrence of AKI (P= 0.005).
Discussion
A combination of procedural and patient-related factors makes AKI a significant complication following TAVI. This underscores the criticality of monitoring and managing renal function in TAVI patients. Knowledge about the incidence of AKI allows healthcare providers to take preventive action against it and improve outcomes for these patients. In our study, the development of AKI within seven days after the procedure was seen in 11 (10.7%) patients. This finding is similar to that obtained by Julien et al. [26], who reported that out of 107,814 individuals from the United States who underwent TAVI, 11,566 (10.7%) experienced AKI. According to another study conducted in Germany, there were cases of AKI among 111 (13.8%) out of 804 patients who underwent TAVI [10]. On the other hand, a higher incidence conducted in a local study to determine the occurrence of AKI following TAVI found that 14 (17.3%) out of 80 patients with AKI were reported by Alatawi et al. [27]. Additionally, Alhamad et al. [28] elucidated that preexisting chronic kidney conditions significantly contribute to the incidence of AKI post TAVI. Echoing this, our research further identifies existing renal conditions, specifically CKD, as crucial determinants. We also found a significant association between hyperlipidemia and the development of AKI post TAVI. This may be due to the link between hyperlipidemia and degenerative aortic valve stenosis [29] or as suggested by Scherner et al. [7] it may be due to the formation of atherosclerotic emboli generated during valvuloplasty when the passage of the catheter through the aorta and deployment of the valve prosthesis may play a role in decreasing the eGFR following TAVI. Recognizing these risk factors is imperative for enhancing patient care protocols and robust postoperative monitoring frameworks, thereby mitigating the associated risks of TAVI.
Secondly, some laboratory tests such as hemoglobin, white blood cell count, platelet count, and electrolyte levels showed no significant differences between patients with and without AKI, suggesting their limited role in AKI development post TAVI. Conversely, the study demonstrates that specific laboratory parameters, specifically sCr, eGFR, and BUN, significantly impacted patient outcomes on the procedure date and post TAVI. This is expected since these tests are reliable indicators of kidney function and can be used to assess the impact of contrast media on the kidneys. Similarly, Sudarsky et al. and Molen et al. identified eGFR as a significant predictor of AKI [5, 20]. Moreover, our research identified a significant association between the type of valve used and the occurrence of AKI. This finding correlates with the study by Loizzi et al. [30], which reported a higher incidence of AKI in patients undergoing TAVI with a specific type of valve, which is self-expanding prostheses. The increased AKI risk may be attributed to the extended periods of extreme hypotension required for the deployment of self-expanding valves compared to balloon-expandable valves. However, further clinical studies are necessary to confirm this association [30].
Thirdly, although there is an ongoing debate about the ideal hydration protocol, Molen et al.'s [20] study emphasized hydration with normal saline or sodium bicarbonate as the primary method of preventing PC-AKI. Nevertheless, our evaluation of preventative measures such as hydration did not significantly affect the occurrence of AKI. This discrepancy might be due to different protocol strategies used to hydrate the patients, which will prompt further research into optimizing preventive measures to reduce the risk of AKI post TAVI. Furthermore, neither the dose of contrast media administered nor the Mehran score significantly correlated with AKI. This lack of significant correlation could be attributed to the small sample size. Overall, the study's findings stress the need for personalized risk assessment and management strategies to reduce the risk of AKI following TAVI, particularly in patients with hyperlipidemia and preexisting kidney conditions.
Limitations
This study has some limitations. Firstly, the retrospective design limits the ability to establish causality between the analyzed factors and the development of AKI. Secondly, the sample size is relatively small, which may limit the generalizability of the findings. Additionally, the study relied on data collected from medical records, which may be subject to incomplete or inaccurate documentation. Finally, the study focused on a specific population undergoing TAVI, which may limit the generalizability of the findings to other patient populations.
Conclusions
Acute kidney injury remains a common and concerning complication following TAVI. The study found that 11 (10.7%) patients who underwent TAVI experienced AKI seven days after the TAVI procedure. The study also highlights the significance of identifying patients with hyperlipidemia and pre-existing kidney conditions and closely monitoring renal function. Though some preventive methods did not significantly affect the occurrence of AKI, further research may be needed to refine the preventive strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute Kidney Injury In: Stat Pearls [Internet] Goyal A Daneshpajouhnejad P Hashmi MF Bashir K Treasure Island, FL Stat Pearls [Internet], Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 441896/28722925 · pubmed ↗
- 2Aortic Valve Disease Stat Pearls 2 2023 Wenn P Zeltser R Treasure Island, FL Stat Pearls [Internet], Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 542205/
- 3Acute kidney injury after transcatheter aortic valve implantation and mortality risk-long-term follow-up Nephrol Dial Transplant Kliuk-Ben Bassat O Finkelstein A Bazan S 433438352020 https://doi.org/10.1093/ndt/gfy 2643016985710.1093/ndt/gfy 264 · doi ↗ · pubmed ↗
- 4What is TAVR? (TAVI) 4 2022 American Heart Association 2022 https://www.heart.org/en/health-topics/heart-valve-problems-and-disease/understanding-your-heart-valve-treatment-options/what-is-tavr
- 5Acute kidney injury following transcatheter aortic valve implantation: association with contrast media dosage and contrast media based risk predication models J Clin Med Sudarsky D Drutin Y Kusniec F 1181112022 https://doi.org/10.3390/jcm 110511813526827110.3390/jcm 11051181 PMC 8911230 · doi ↗ · pubmed ↗
- 6Acute kidney injury after transcatheter aortic valve replacement in the elderly: outcomes and risk management Clin Interv Aging Zaleska-Kociecka M Dabrowski M Stepinska J 1952011420193071894610.2147/CIA.S 149916 PMC 6345183 · doi ↗ · pubmed ↗
- 7Meta-analysis of predictors of all-cause mortality after transcatheter aortic valve implantation Am J Cardiol Giordana F D'Ascenzo F Nijhoff F 1447145511420142521745610.1016/j.amjcard.2014.07.081 · doi ↗ · pubmed ↗
- 8Acute kidney injury after transcatheter aortic valve implantation J Thorac Dis Scherner M Wahlers T 1527153572015 https://doi.org/10.3978/j.issn.2072-1439.2015.06.142654359810.3978/j.issn.2072-1439.2015.06.14PMC 4598516 · doi ↗ · pubmed ↗