Acute Decompensated Heart Failure Secondary to Left Atrial Myxoma: A Case Report Highlighting Diagnostic Challenges and Multidisciplinary Management
Vasileios Leivaditis, Eleftherios T Beltsios, Athanasios Papatriantafyllou, Kostas Grapatsas, Francesk Mulita, Manfred Dahm

TL;DR
A 68-year-old woman with acute heart failure was found to have a rare heart tumor, which was successfully treated through surgery and recovery.
Contribution
This case report emphasizes the diagnostic challenges and multidisciplinary management of left atrial myxoma presenting as acute heart failure.
Findings
Left atrial myxoma can present as acute decompensated heart failure and cause significant valve obstruction.
Emergency surgery followed by valve replacement and extracorporeal life support led to significant patient recovery.
The patient remained asymptomatic at follow-up with no cardiac decompensation.
Abstract
Cardiac myxomas are the most common benign tumors of the heart, with clinical manifestations varying significantly based on tumor size. Symptoms can range from asymptomatic and mild non-specific presentations to severe obstructive cardiac and systemic findings. This case report describes a 68-year-old female patient who presented with acute decompensated heart failure. Diagnostic evaluation revealed a left atrial myxoma causing significant mitral valve obstruction. The patient underwent emergency cardiac surgery for tumor removal, complicated by severe mitral and tricuspid valve regurgitation. Following valve replacement and repair, the patient required extracorporeal life support. Despite these complexities, she achieved significant recovery and was discharged in good condition. At follow-up, she remained asymptomatic with no signs of cardiac decompensation. This case highlights the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
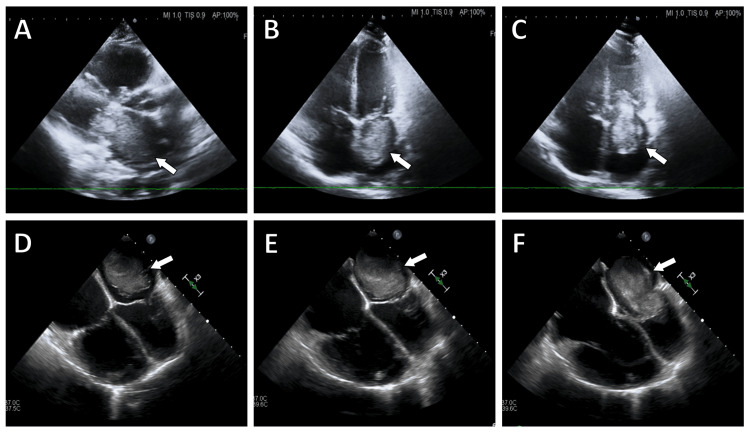 Figure 1
Figure 1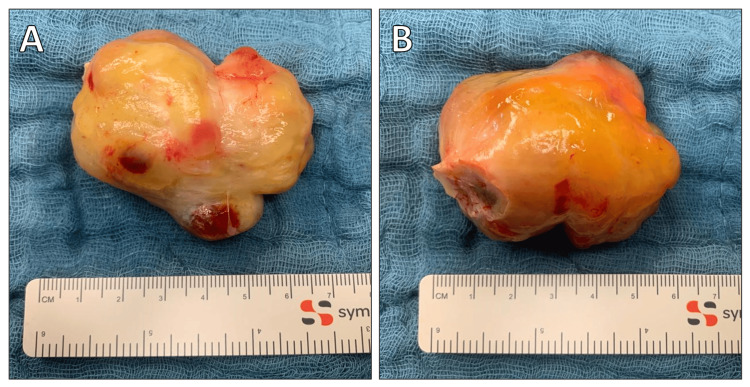 Figure 2
Figure 2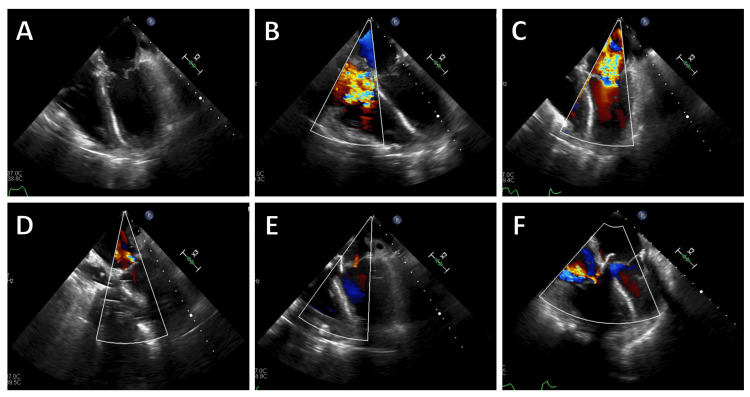 Figure 3
Figure 3| Parameter | Obtained value | Reference ranges | International units |
| Blood pressure | 136/92 | 120/80 | mmHg |
| SpO2 | 92 | 95-98.5 | % |
| Respiratory rate | 21 | 12-18 | Breaths per minute |
| Pulse rate | 122 | 60-100 | Beats per minute |
| Temperature | 37.2 | 36.5–37.5 | °C |
| White blood cell count | 14.26 | 3.8-10.3 | 1000/µL |
| Hemoglobin | 11.7 | 13.5-17.8 | g/dL |
| CRP | 73 | <5 | mg/L |
| Procalcitonin | 0.34 | <0.05 | ng/mL |
| Creatinin | 1.37 | 0.7-1.2 | mg/dL |
| BUN | 67 | 8-23 | mg/dL |
| Troponin T | 362 | 0-14 | pg/mL |
| CPK | 196 | 20-200 | U/L |
| CK-MB | 11 | <25 | U/L |
| NT-proBNP | 1243 | <386 | pg/mL |
| LDH | 291 | <250 | U/L |
| GOT (AST) | 67 | 10-50 | U/L |
| GPT (ALT) | 94 | 10-50 | U/L |
| Sodium | 143 | 136-145 | mmlol/L |
| Potassium | 3.9 | 3.4-4.5 | mmlol/L |
| Lactic acid | 2.8 | 0.5-2.2 | mmol/L |
| pH | 7.38 | 7.37-7.45 |
| Feature | Myxoma | Thrombus | Other tumors (e.g., fibroelastoma) |
| Location | Left atrium, typically at fossa ovalis | Left atrium (appendage), left ventricle (post-MI) | Valvular endocardium or ventricular outflow tract |
| Attachment | Narrow, often pedunculated | Broad-based | Narrow, with a pedicle |
| Mobility | Highly mobile, may prolapse through AV valve | Less mobile | Highly mobile |
| Shape | Lobulated, irregular | Smooth, more uniform | Small, often round or oval |
| Size | Variable, can be large (up to 15 cm) | Typically smaller, variable | Generally small (<1 cm) |
| Echotexture | Heterogeneous | Homogeneous | Homogeneous |
| Borders | Well-defined | Less well-defined | Well-defined |
| Functional Impact | Can obstruct AV valve during diastole | May impair ventricular function | Rarely obstructive, more likely embolic |
| T1 Signal | Heterogeneous intermediate | Homogeneous hypointense | Homogeneous low |
| T2 Signal | Heterogeneous hyperintense | Homogeneous hypointense | Homogeneous high |
| Gadolinium Enhancement | Heterogeneous, variable | Typically no enhancement, unless organized | Uniform enhancement |
| Inversion Time on LGE | 200–300 ms | 550–650 ms | N/A |
| Perfusion | Delayed perfusion, heterogeneous uptake | No perfusion | Homogeneous uptake |
| Calcification | Possible, seen in some cases | Rare, unless chronic | Rare |
| Hemorrhage | Possible, seen in some cases | Rare | Rare |
| Consistency | Soft, gelatinous | Firm, organized if chronic | Firm |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Cardiac Structural Anomalies and Repair · Peptidase Inhibition and Analysis
Introduction
Cardiac myxomas are the most common primary heart tumors in adults, with an incidence of up to 0.2% in autopsy series. Myxomas are more common in women than men, with a 2:1 female-to-male ratio, and can occur at any age [1]. These benign tumors originate from multipotent mesenchyme and typically appear as undifferentiated atrial masses, often pedunculated and attached to the fossa ovalis on the left atrial septum [2,3]. Epidemiologically, myxomas have also been classified into two certain epidemiological types: familial and sporadic. About 75% of myxomas are located in the left atrium, 23% in the right atrium, and 2% in the ventricles. Rarely, they can be present in multiple chambers. These tumors most commonly range in size from 1 to 15 cm in diameter.
Symptoms vary widely, from mild, non-specific symptoms to severe conditions, such as heart failure, stroke, and sudden death. The classic symptom triad includes constitutional, embolic, and obstructive or cardiac manifestations. Due to the vague nature of these symptoms, diagnosis can be challenging, requiring a high level of clinical suspicion [2,4]. Echocardiography is the first-line imaging technique for diagnosis, although it presents limitations. CT scans or cardiac MRI may be needed for detailed evaluation. Histopathological assessment confirms the diagnosis [2].
Timely surgical resection greatly improves prognosis, with postsurgical survival rates similar to the general population. However, tumor recurrences can occur, often due to incomplete resection [3]. This report details the presentation, diagnosis, surgical intervention, and recovery of a patient with a left atrial myxoma causing acute decompensated heart failure.
Case presentation
Patient background
A 68-year-old female patient with a medical history of hypertension, dyslipidemia, and hypothyroidism presented to the emergency department with severe worsening dyspnea and bilateral peripheral edema. Physical examination revealed signs consistent with acute decompensated heart failure, including jugular venous distention, pulmonary rales, and peripheral edema.
Diagnostic workup
Initial laboratory tests indicated elevated B-type natriuretic peptide (BNP) levels (Table 1). An urgent echocardiogram revealed a large left atrial mass with a pedunculated attachment to the interatrial septum, prolapsing into the mitral valve orifice during diastole, causing functional mitral valve stenosis (Figure 1). Coronary angiography did not show any significant coronary artery disease.
Echocardiographic images showing the left atrial myxoma. Echocardiographic images showing the left atrial myxoma (arrow). Transthoracic echocardiography (TTE) short-axis view (A) and four-chamber view in the systolic (B) and diastolic (C) phases. Transesophageal echocardiography (TEE) images demonstrating the movement of the myxoma in the systolic (D, E) and diastolic phases (E).
Surgical intervention
Due to the acute obstruction caused by the left atrial myxoma, the patient was referred for emergency cardiac surgery. The operation involved complete cardiopulmonary bypass and removal of the myxoma (Figure 2) through the right atrium. The cardiopulmonary bypass time was 156 minutes, and the total aortic cross-clamp time was 92 minutes. Intraoperatively, severe mitral and tricuspid valve regurgitation was noted during weaning from cardiopulmonary bypass, likely masked preoperatively by the myxoma (Figure 3). Attempts at mitral valve repair were unsuccessful, necessitating replacement with a biological prosthesis and tricuspid valve repair using the DeVega annuloplasty technique.
Intraoperative image of the left atrial myxoma after its excision.
Intraoperative transesophageal echocardiography (TEE) images. (A) After removal of the myxoma, (B) severe tricuspid regurgitation, (C) severe mitral regurgitation, (D) persistent significant regurgitation after mitral valve repair, (E) result after mitral valve replacement, (F) residual less significant tricuspid regurgitation after tricuspid valve annuloplasty.
Postoperative course
The patient experienced severe right heart failure and problematic ventilation, requiring extracorporeal life support via the right femoral vein and ascending aorta. Despite aggressive management, the patient exhibited prolonged ventilator dependence, which prompted the decision to perform a tracheotomy on the seventh postoperative day. The tracheotomy facilitated prolonged mechanical ventilation, enhanced pulmonary hygiene, and improved patient comfort. Gradual weaning from extracorporeal support was achieved in the ICU over the following weeks. Continuous echocardiographic monitoring showed significant improvement in cardiac function. By the 11th postoperative day, the patient was successfully weaned from ECLS, and by the 15th postoperative day, she was gradually weaned off the ventilator. Histopathological examination confirmed the diagnosis of cardiac myxoma. Follow-up echocardiography showed significant improvement in cardiac function. The patient was transferred to the regular ward on the 17th postoperative day, where she continued to show marked improvement. Physical therapy and rehabilitation were initiated to enhance her recovery.
Outcome and follow-up
The patient was discharged ambulatory and asymptomatic on the 28th postoperative day. Follow-up visits at one and six months post-surgery revealed an asymptomatic patient with no signs of cardiac decompensation or recurrent myxoma.
Discussion
Atrial myxomas, the most common benign cardiac tumors, often present with symptoms similar to mitral valve disease or embolic phenomena [5]. This case highlights the need to consider cardiac myxomas in the differential diagnosis of acute decompensated heart failure. The patient’s rapid deterioration required immediate surgical intervention, showcasing the challenges in managing severe valvular regurgitation. Extracorporeal life support postoperatively was crucial for her recovery.
An accurate diagnosis of cardiac myxomas may be challenging with various confounding factors delaying it. Despite their rarity, with an incidence of 0.5 per million annually, they can present with nonspecific symptoms like syncope, dyspnea, or positional breathlessness [4,6,7]. In this case, the patient’s acute heart failure symptoms were due to the myxoma’s obstruction of the mitral valve, mimicking severe mitral stenosis and hiding severe mitral valve regurgitation. This underlines the importance of advanced imaging and timely surgery.
Due to their multifaceted nonspecific clinical presentation that varies from asymptomatic to life-threatening conditions like obstruction, embolization, and stroke [8], myxomas are initially suspected in only 5.7% of patients. Left atrial tumors pose a risk of systemic embolization, while their position can obstruct blood flow, mimicking mitral stenosis and leading to heart failure or sudden death if untreated [9]. In the present case, the large-sized myxoma caused significant obstruction, necessitating urgent surgery.
Depending on their location and morphology, cardiac tumors can produce four main types of clinical manifestations: (i) systemic-constitutional, (ii) embolic, (iii) cardiac, and (iv) secondary metastatic effects [10]. Cardiovascular symptoms such as chest pain, syncope, dyspnea, and angina occur in about 67% of patients, with 28% presenting acute decompensated heart failure. Constitutional symptoms affect 34%, and embolic symptoms are present in 29% of these patients [1,10]. Left-sided myxomas often cause systemic embolization, while right-sided tumors typically embolize to the pulmonary circulation. Pleural effusion is an unusual manifestation and has been reported in a few case studies [5,11]. The increase in LA pressure may cause transudative pleural effusion due to the mitral valve obstruction [5]. Asymptomatic myxomas are often discovered incidentally on imaging [1].
Sudden cardiac death amongst myxoma patients is rare, occurring in about 0.005-0.01% of all sudden deaths, often due to severe acute disturbances in hemodynamics or coronary embolization [1]. This highlights the need for a high index of suspicion in cases with unexplained symptoms.
EKG findings can be nonspecific in 20-40% of patients. The most common EKG finding is left atrial hypertrophy [6]. Echocardiography, both transthoracic (TTE) and transesophageal (TEE), is essential for visualizing and better characterizing cardiac tumors [4]. TEE offers superior image resolution; it is crucial for accurate diagnosis and detailed evaluation and is therefore considered the gold standard for investigating cardiac tumors. It provides crucial information regarding the size, location, and attachment points of tumors, which are critical for planning appropriate surgical interventions and ensuring optimal patient outcomes [4,12]. Crucial factors include the type and location of attachment (whether sessile or pedunculated), surface features (smooth and bosselated versus irregular and fimbriated), and echotexture (identifying hemorrhagic areas and calcification with varying echotextures, homogeneous versus heterogeneous) [13]. Cardiac MRI and CT may provide additional structural and hemodynamic information, complementing the echocardiographic findings [10,14].
While echocardiography is typically the initial imaging modality for cardiac tumors, it can be challenging to distinguish myxomas from other cardiac masses, such as thrombi. Cardiac MRI (CMR) has emerged as a superior imaging modality due to its excellent tissue characterization capability, enabling differentiation between myxomas and thrombi [15] Myxomas often appear as well-defined, smooth, oval or lobular lesions with a narrow pedunculated attachment, frequently at the fossa ovalis. They are typically very mobile and can prolapse through the atrioventricular valves during diastole, causing temporary obstruction to blood flow. Myxomas display heterogeneous intermediate T1 and hyperintense T2 signals due to their mixed tissue composition, and they show a characteristic heterogeneous enhancement pattern on gadolinium-enhanced sequences. In contrast, thrombi are usually broad-based, less mobile, and typically show homogeneous hypointense signals on both T1- and T2-weighted sequences, with no enhancement unless highly organized and fibrous. Other cardiac tumors, such as papillary fibroelastomas, are smaller, highly mobile, and often show uniform enhancement on imaging [16-17]. Table 2 summarizes the key imaging features that help differentiate myxomas from thrombi based on cardiac CMR findings.
Surgical removal is the primary treatment for atrial myxomas, aiming for complete excision to restore cardiac function. Post-surgery, patients typically experience symptom resolution. Although recurrence is reported to be relatively rare. with rates raging 2-13%, follow-up with ongoing monitoring is necessary, especially in cases with a family history or incomplete excision [6]. Effective management involves a multidisciplinary approach, integrating cardiologists, cardiothoracic surgeons, radiologists, and pathologists, with providing adequate information to the patient regarding the condition and surgery rationale [4,18].
In summary, this case demonstrates the complexity of the diagnosis and management of atrial myxomas, especially when they present with severe symptoms mimicking or hiding other cardiac conditions. In our case, an underlying severe mitral valve regurgitation was masked through the presence of the myxoma. Advanced imaging and prompt surgical intervention are essential for favorable outcomes.
Conclusions
This case report underlines the critical importance of considering cardiac myxomas in the differential diagnosis of acute decompensated heart failure. Early diagnosis and prompt surgical intervention are crucial for favorable outcomes in patients with cardiac myxomas. This demonstrates that tailored management strategies are essential for addressing the unique challenges posed by these tumors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Atrial myxoma mimicking mitral stenosis Cardiol Res Spartalis M Tzatzaki E Spartalis E 128130820172872533010.14740/cr 558w PMC 5505297 · doi ↗ · pubmed ↗
- 2Cardiac myxomas: clinical presentation, diagnosis and management Heart Griborio-Guzman AG Aseyev OI Shah H Sadreddini M 82783310820223449354710.1136/heartjnl-2021-319479 · doi ↗ · pubmed ↗
- 3Cardiac myxomas: causes, presentations, diagnosis, and management Ir J Med Sci Saad EA Mukherjee T Gandour G 67768819320243773791610.1007/s 11845-023-03531-2 · doi ↗ · pubmed ↗
- 4Misattribution of dyspnea: unveiling atrial myxoma as the true culprit Cureus Al Zweihary AM 016202410.7759/cureus.58790 PMC 1111213338784305 · doi ↗ · pubmed ↗
- 5Huge left atrial myxoma obstructs the mitral valve and causes massive pleural effusion Chonnam Med J Lee WC Shih JY Wu NC 1381396020243884160910.4068/cmj.2024.60.2.138PMC 11148305 · doi ↗ · pubmed ↗
- 6A giant left atrial myxoma causing mitral valve pseudostenosis - a mimicker J Community Hosp Intern Med Perspect Abdelazeem B Khan H Changezi H Munir A 5235271120213421166210.1080/20009666.2021.1930867 PMC 8221166 · doi ↗ · pubmed ↗
- 7Cardiac myxoma embolization causing ischemic stroke and multiple partially thrombosed cerebral aneurysms Stroke Kesav P John S Joshi P Gaba WH Hussain SI 0452202110.1161/STROKEAHA.120.03167933213289 · doi ↗ · pubmed ↗
- 8Cerebral aneurysms caused by atrial myxoma-a systematic review of the literature J Pers Med Chojdak-Łukasiewicz J Budrewicz S Waliszewska-ProsółM 13202210.3390/jpm 13010008 PMC 986136436675669 · doi ↗ · pubmed ↗