Flexor Hallucis Longus Transfer With Concurrent Gastrocnemius Augmentation in Neglected Tendoachilles Tears: A Case Series
Vijayanand B, Kannan KC, Karthikeyan S

TL;DR
This case series explores a surgical treatment for neglected Achilles tendon ruptures using a combination of tendon transfer and muscle augmentation, showing significant improvement in patients.
Contribution
The study introduces a combined surgical approach for neglected Achilles tendon tears using FHL transfer and gastrocnemius augmentation.
Findings
Three patients with neglected Achilles tendon ruptures showed significant clinical improvement after surgery.
AOFAS scores improved from an average of 35 to 85, and VAS pain scores decreased from 8 to 2 at six months.
The procedure is presented as an effective treatment for large Achilles tendon defects.
Abstract
The Achilles tendon, the body's largest tendon, is often vulnerable to rupture, primarily as a result of sudden dorsiflexion of a plantar-flexed foot. This injury predominantly affects individuals in their youth and middle age. In this case series, we describe three middle-aged men with neglected insertional Achilles tendon ruptures, each presenting an average 10 cm defect. They underwent a surgical procedure involving flexor hallucis longus (FHL) tendon transfer with concurrent gastrocnemius augmentation. The FHL tendon was repositioned proximally and securely tenodesed to the proximal stump of the excised Achilles tendon. Following this intervention, substantial clinical improvements were observed at the six-month follow-up, with the American Orthopaedic Foot and Ankle Society (AOFAS) score improving from 35 to 85 and the Visual Analog Scale (VAS) pain score decreasing from 8 to 2.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
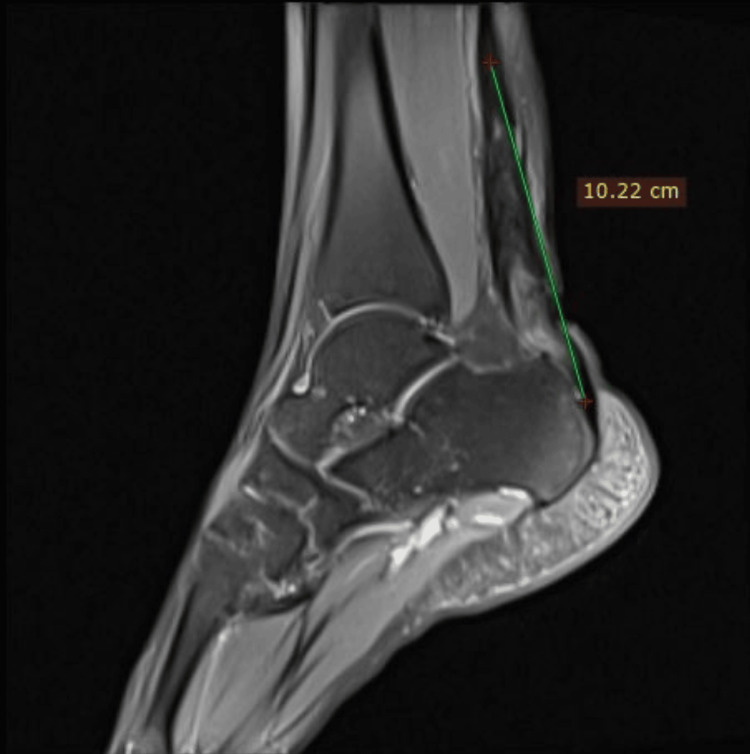 Figure 1
Figure 1 Figure 2
Figure 2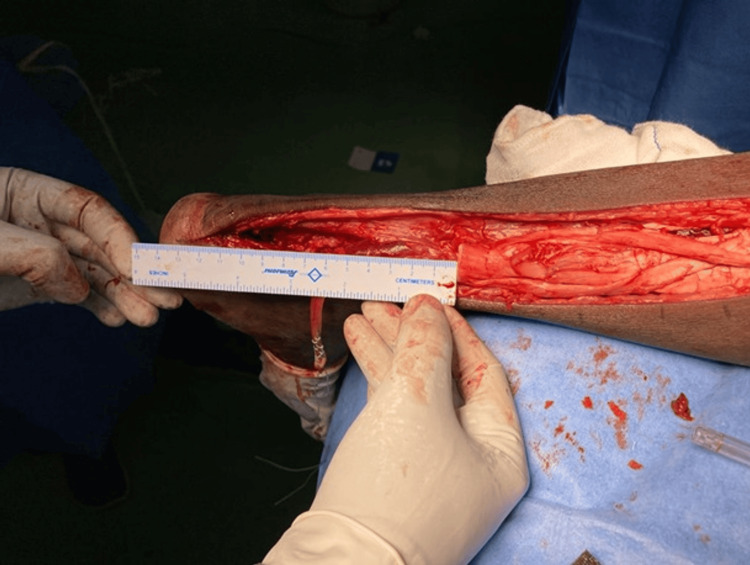 Figure 3
Figure 3 Figure 4
Figure 4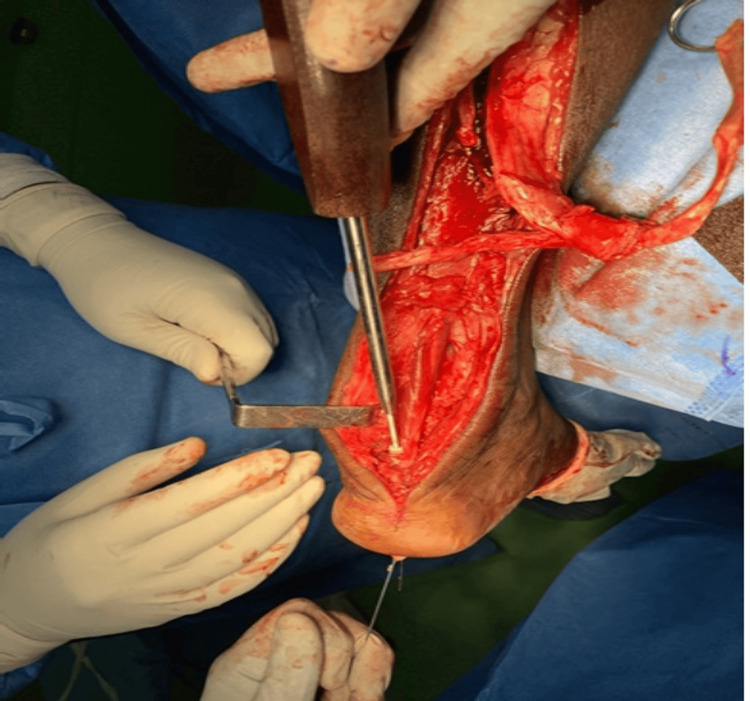 Figure 5
Figure 5 Figure 6
Figure 6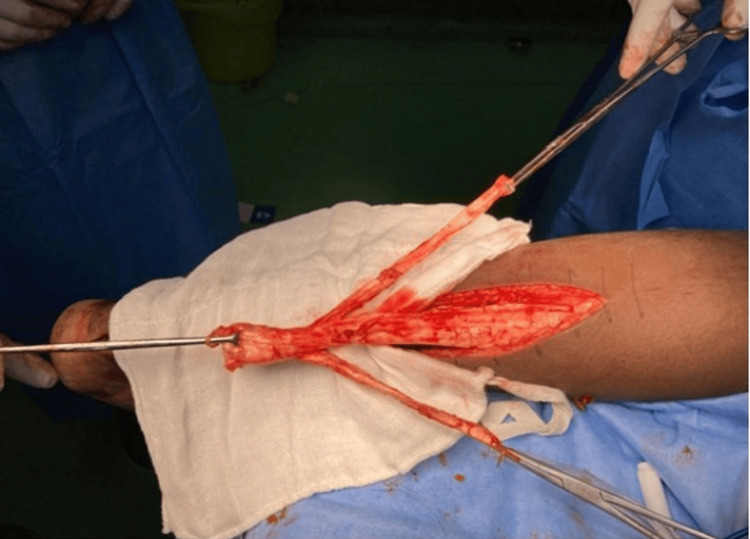 Figure 7
Figure 7 Figure 8
Figure 8 Figure 9
Figure 9 Figure 10
Figure 10| P. No | Gender | Age | Occupation | Side | Pre-op gap as per MRI | Post-debridement gap |
| 1. | Male | 51 | Manual labourer | Right | 10.22 cm | 12 cm |
| 2. | Male | 48 | Farmer | Left | 12.05 cm | 13.5 cm |
| 3. | Male | 41 | Machine operator | Left | 12 cm | 13 cm |
| Sl. No | Chronicity of tear | Pre-op AOFAS score | 6 month post-operative AOFAS score | 1 year follow-up AOFAS score | Total duration of follow-up |
| 1. | 4 months | 68 | 89 | 99 | 12 months |
| 2. | 3 months | 76 | 85 | 100 | 15 months |
| 3. | 4 months | 81 | 90 | 98 | 15 months |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTendon Structure and Treatment · Sports injuries and prevention · Foot and Ankle Surgery
Introduction
Techniques such as angioplasty or tendon transfers can effectively manage chronic Achilles tendon ruptures. Kuwada et al. classified chronic tendo-Achilles tears into four types based on the defect size: type 1 with less than 50% tear recommended treatment is cast immobilisation for eight weeks; type 2 where the defect is less than 3 cm simple end-to-end anastomosis is recommended; type 3 where the defect is 3-6 cm end-to-end anastomosis with autogenous or synthetic graft is recommended; type 4 where the defect is greater than 6 cm (chronic cases) gastrocnemius recession/free tendon grafts/tendon transfer is recommended [1]. The transfer of the flexor hallucis longus (FHL) tendon for chronic Achilles tendon conditions has been shown to not only alleviate pain but also enhance overall function [2,3]. Following flexor hallucis longus tendon transfer, the maximum plantar flexion strength is reduced by 16% to 35% when compared to the native Achilles tendon [4]. Patients also tend to experience diminished performance in single- and two-leg heel-rise tests. However, there is a lack of research that investigates patients' return to work as well as their ability to walk or engage in activities such as jumping. In the following article, we present three cases of chronic tendo-Achilles rupture managed by flexor hallucis longus transfer with tendo-Achilles augmentation.
Case presentation
Case 1
A 51-year-old male manual labourer presented with a history of difficulty walking following an injury to the back of his right heel four months ago. The Thompson squeeze test and single-leg heel raise test were positive. MRI showed chronic rupture of the tendo Achilles with tendonitis with a gap of 10.22 cm and Haglund deformity (Figure 1). The patient underwent flexor hallucis longus transfer and tendo-Achilles augmentation as he was categorised under the type 4 Kuwada classification. The patient was put in a prone position, with his ankle and foot free over the edge of the table, allowing a full range of movement. A posterior midline longitudinal incision was made, and the paratenon was opened. The retracted tendo Achilles was identified and debrided (Figure 2). Post-debridement of the edges revealed a gap of 12 cm (Figure 3). Flexor hallucis longus was identified and harvested from Henry's master knot (Figure 4). The tendon was prepared and sized to be 5 mm. A transosseous tunnel of diameter 6 mm was made 1 cm anterior to the tendo-Achilles insertion site in the calcaneum from the superior to inferior direction. The prepared graft was pulled through the tunnel and fixed with a 6 mm interference screw (Figure 5) at 20° of plantar flexion (Figure 6). Then augmentation was done using flaps taken along the aponeurosis of the tendo Achilles and turned down by 180° (Figure 7), which was sutured to the transferred flexor hallucis longus (Figure 8). After thorough lavage, the paratenon was closed, followed by skin closure in layers. Figure 9 shows the immediate post-op X-ray. An above-knee cast was applied, which was revised with increasing angles of dorsiflexion as tolerated every two weeks. Ankle ROM and partial weight bearing were allowed by six weeks and full weight bearing by 12 weeks. The preop American Orthopaedic Foot and Ankle Society (AOFAS) score was 68. Six-month post-operative and one-year post-operative AOFAS scores were 89 and 99, respectively.
Pre-operative MRI of the ankle showing torn and retracted tendo-Achilles with gap of 10.22 cmCase 1
After posterior midline incision and opening of the paratenon, the torn stumps of the retracted tendo-Achilles is seenCase 1
Post debridement of the torn stumps showing a defect of 12 cmCase 1
The flexor hallucis longus is harvested from the master knot of Henry and prepared for transferCase 1
Transosseous transfer of flexor hallucis longus onto the posterosuperior aspect of calcaneum using interference screwCase 1
Post transfer of flexor hallucis longus, the ankle is maintained in 20° of plantar flexionCase 1
Gastrocnemius aponeurotic flaps taken on either side for turn down procedureCase 1
Completed flexor hallucis longus transfer with tendo-Achilles augmentationCase 1
Post-operative X-ray following flexor hallucis longus transfer with tendo-Achilles augmentationCase 1
Case 2
A 48-year-old male farmer by occupation with a history of laceration to the back of his heel on the left side that was sutured at a local hospital presented to us after three months of difficulty walking. On examination, the patient had a scar over the posterior aspect of the ankle with a palpable defect over the tendo-Achilles insertion region. The single-leg heel raise and Thompson test were positive. An MRI was done, which showed a chronic retracted tendo-Achilles tear with a gap of 12 cm. Flexor hallucis longus tendon transfer with tendo-Achilles augmentation was done using the same procedure as described in case 1, since the post-debridement gap of the tendo Achilles was more than 6 cm by Kuwada classification. The subsequent treatment course involved placing the patient in an above-knee cast with the foot in a plantar flexed position for four to six weeks, with gradual adjustments until 20° ankle dorsiflexion is achieved. After six weeks, the patient was permitted partial-weight-bearing ambulation with crutches and an ankle-foot boot. By 12 weeks, the patient had started full-weight-bearing walking. Figure 10 shows the completed flexor hallucis longus transfer with tendo-Achilles augmentation. The preop AOFAS score was 76. Six-month post-operative and one-year post-operative AOFAS scores were 85 and 100, respectively.
Intraoperative image showing the completed flexor hallucis longus transfer with tendo-Achilles augmentationCase 2
Case 3
A 41-year-old male machine operator presented with an inability to do a single-leg heel raise on his left side after a direct hit to his heel four months ago. An MRI showed a chronic retracted tendo-Achilles avulsion with a gap of 12 cm. Flexor hallucis longus tendon transfer with tendo-Achilles augmentation was done following similar surgical steps and post-operative protocol. Full-weight bearing was started after three months. The preop AOFAS score was 81. Six-month post-operative and one-year post-operative AOFAS scores were 90 and 98, respectively.
Results
All three patients were followed up for one year. The data of the three patients with chronic retracted tendo-Achilles rupture treated by flexor hallucis longus transfer and tendo-Achilles augmentation is tabulated below (Table 1). All the patients were classified as type IV by the Kuwada classification as the gap was more than 6 cm.
All three patients were put on above-knee casts with 20° of plantar flexion in the post-operative period. The cast was gradually altered once every two weeks to obtain a final dorsiflexion of 20° by six to eight weeks. Partial weight bearing, as tolerated, was started by six weeks and progressed to full weight bearing by 12 weeks. By six months, all the patients were able to do single-leg heel raises without support. The power of the flexor hallucis longus was reduced when compared to the preoperative state, but it did not interfere with the patient’s gait postoperatively in all three cases. At six months and one year, the AOFAS score was calculated, which is recorded in the below table (Table 2).
The results show that this procedure gives better functional outcomes to the patients with regard to the ankle and foot scores. Also, all three patients in our study returned to their occupation by six to nine months post-surgery. One patient developed a superficial infection of the suture site, which was treated with regular dressings and oral antibiotics. The other two patients did not have any post-operative complications.
Discussion
Addressing chronic Achilles tendon ruptures presents a formidable challenge for orthopaedic surgeons [5]. These chronic ruptures, distinguished by their distinct pathophysiological characteristics from acute cases, often entail the formation of significant gaps within the tendon. When these gaps are bridged by scar tissue, it can lead to functional impairments in the ankle, manifesting as ankle weakness and gait disturbances [6]. This pathophysiological complexity may be further exacerbated by the infiltration of substantial amounts of fat into the tendon gap.
Chronic Achilles tendon ruptures are prone to misdiagnosis, and up to 20% of cases may progress to a neglected state [4]. Following an Achilles tendon rupture, patients frequently experience a notable reduction in plantar flexion strength, which leads to an altered gait pattern. A modified Thompson test can be used for the clinical evaluation of tendo-Achilles tears. The test exhibited a higher rate of positive results when conducted with the patient in a prone position, with the knee flexed at 90°, as opposed to when the knee was extended. However, the inability to perform a single-leg heel rise represents a pivotal clinical sign, often necessitating the consideration of reconstruction surgery. Surgical reconstruction, as highlighted in our study, holds the potential to fully restore Achilles tendon strength, leading to marked improvements in patient mobility. However, it is imperative to acknowledge that the procedures involved in the reconstruction and augmentation of chronic Achilles tendon ruptures are challenging, and the selection of surgical techniques should be influenced by the size of the defect [1].
In our study, we observed a notable contrast with previous reports. It has been reported that between 50% and 86% of patients were able to perform a single-limb heel raise test on the operated side after the transfer of the flexor hallucis longus tendon, with comparatively poorer outcomes in cases of chronic ruptures [7,8]. In our study, a complete improvement in single-limb heel raise capability was observed after flexor hallucis longus transfer, indicating more favourable outcomes even in the context of chronic Achilles tendon ruptures. In the study by Yeoman et al. [9], they successfully managed 11 patients with chronic Achilles tendon ruptures by employing the Flexor Hallucis Longus technique in conjunction with interference screw fixation, achieving consistent and favourable outcomes with minimal complications. Furthermore, Oksanen et al. [4] reported a notable hypertrophy of approximately 52% in the transferred Flexor Hallucis Longus muscle, as observed through MRI evaluation following a chronic tendo-Achilles tear.
Interestingly, a comparable phenomenon was also observed in our current study. This observation suggests that the flexor hallucis longus tendon possesses a remarkable capacity for adaptation, which could be instrumental in achieving positive results in the context of Achilles tendon rupture management. Furthermore, Tay et al. [10] and Peterson et al. [11] reported that chronic Achilles tendon ruptures treated with two turndown flaps and flexor hallucis longus augmentation yielded satisfactory results during a two-year follow-up when addressing central defects of approximately 12 cm. In our study, we observed improvements in the AOFAS score within 12 months, indicating a satisfactory overall improvement in patient outcomes.
These findings emphasise the complexity and variability of managing chronic Achilles tendon ruptures. The choice of diagnostic tools, surgical techniques, and post-operative assessments can significantly impact patient outcomes and highlight the need for further research and evaluation in this challenging clinical area.
Conclusions
In conclusion, our study demonstrates that the reconstructive technique using flexor hallucis longus transfer with concurrent gastrocnemius augmentation can yield good clinical and functional outcomes. We have found this surgical technique to be highly valuable in addressing the challenging cases of neglected Achilles tendon ruptures. These results underscore the effectiveness of flexor hallucis longus tendon transfer combined with gastrocnemius augmentation as a viable treatment option, but a large sample size will be required to further evaluate and validate the same, especially for neglected insertional Achilles tendon tears that present substantial defects. This approach holds the promise of not only enhancing functional outcomes but also providing significant improvement in gait patterns for affected patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Classification of tendo Achillis rupture with consideration of surgical repair techniques J Foot Surg Kuwada GT 36129(4)1990 https://scholar.google.com/scholar?hl=en&as_sdt=0%2C 5&q=Kuwada+GT.+Classification+of+tendo+Achillis+rupture+with+consideration+of+surgical+repair+techniques.+J+Foot+Surg.+1990%3B 29%284%29%3A 361.&btn G=2229913 · pubmed ↗
- 2Repair of chronic Achilles tendon rupture with flexor halluces longus tendon transfer Foot Ankle Wapner L 443449141993 https://scholar.google.com/scholar?q=intitle:Repair%20of%20chronic%20Achilles%20tendon%20rupture%20with%20flexor%20halluces%20longus%20tendon%20transfer 825343610.1177/107110079301400803 · doi ↗ · pubmed ↗
- 3Surgical reconstruction of chronic Achilles tendon ruptures using various methods Orthopedics Park YS Sung KS 213218352012 https://scholar.google.com/scholar?q=intitle:Surgical%20reconstruction%20of%20chronic%20Achilles%20tendon%20ruptures%20using%20various%20methods 2231040910.3928/01477447-20120123-13 · doi ↗ · pubmed ↗
- 4Hypertrophy of the flexor hallucis longus muscle after tendon transfer in patients with chronic Achilles tendon rupture Foot Ankle Surg Oksanen MM Haapasalo HH Elo PP Laine HJ 253257202014 https://scholar.google.com/scholar?q=intitle:Hypertrophy%20of%20the%20flexor%20hallucis%20longus%20muscle%20after%20tendon%20transfer%20in%20patients%20with%20chronic%20Achilles%20tendon%20rupture 2545766110.1016/j.fas.2014.06.003 · doi ↗ · pubmed ↗
- 5Operative versus nonoperative treatment of Achilles tendon rupture. A prospective randomized study and review of the literature Am J Sports Med Cetti R Christensen SE Ejsted R Jensen NM Jorgensen U 791799211993 https://scholar.google.com/scholar?q=intitle:Operative%20versus%20nonoperative%20treatment%20of%20Achilles%20tendon%20rupture.%20A%20prospective%20randomized%20study%20and%20review%20of%20the%20literature%2C 829162810.1177/036354659302100606 · doi ↗ · pubmed ↗
- 6Chronic Achilles tendon disorders: tendinopathy and chronic rupture Clin Sports Med Maffulli N Via AG Oliva F 607624342015 https://scholar.google.com/scholar?q=intitle:Oliva%2C%20%E 2%80%9C Chronic%20Achilles%20tendon%20disorders%3A%20tendinopathy%20and%20chronic%20rupture%2C%E 2%80%9D 2640958610.1016/j.csm.2015.06.010 · doi ↗ · pubmed ↗
- 7An outcome study of chronic Achilles tendinosis after excision of the Achilles tendon and flexor hallucis longus tendon transfer Foot Ankle Int Martin RL Manning CM Carcia CR Conti SF 691697262005 https://scholar.google.com/scholar?q=intitle:An%20outcome%20study%20of%20chronic%20Achilles%20tendinosis%20after%20excision%20of%20the%20Achilles%20tendon%20and%20flexor%20hallucis%20longus%20tendon%20transfer 1617449810.1177/107110070502600905 · doi ↗ · pubmed ↗
- 8Outcome of single incision flexor hallucis longus transfer for chronic achilles tendinopathy Foot Ankle Int Will RE Galey SM 315317302009 https://scholar.google.com/scholar?q=intitle:Outcome%20of%20single%20incision%20flexor%20hallucis%20longus%20transfer%20for%20chronic%20achilles%20tendinopathy 1935635510.3113/FAI.2009.0315 · doi ↗ · pubmed ↗